Mikihiko Yasuda1, Yusuke Niina1, Masahiko Uchida1, Nao Fujimori1, Taichi Nakamura1, Takamasa Oono1, Hisato Igarashi1, Kousei Ishigami2, Yumi Yasukouchi3, Kazuhiko Nakamura1, Tetsuhide Ito1, Ryoichi Takayanagi1
Departments of 1Medicine and Bioregulatory Science, 2Clinical Radiology, and 3General Internal
Medicine, Graduate School of Medical Sciences, Kyushu University. Fukuoka, Japan
- *Corresponding Author:
- Tetsuhide Ito
Department of Medicine and Bioregulatory Science, Graduate
School of Medical Sciences, Kyushu University, 3-1-1 Maidashi,
Higashi-ku, Fukuoka 812-8582, Japan
Phone: +81-92.642.5285
Fax: +81-92.642.5287
E-mail: itopapa@intmed3.med.kyushu-u.ac.jp
Received April 1st, 2010 - Accepted May 11th, 2010
Keywords
Adipose Tissue; Cholangiopancreatography, Endoscopic Retrograde; Exocrine Pancreatic Insufficiency; Pancreas
INTRODUCTION
Lipomatous pseudohypertrophy of the pancreas is an extremely rare disease, and only about a dozen cases of typical lipomatous pseudohypertrophy of the pancreas without abnormality or narrowing of the pancreatic duct have been reported. Lipomatous pseudohypertrophy of the pancreas is characterized by the replacement of pancreatic acinar cells with adipose tissue, although the pancreatic duct and islets are preserved [1, 2]. We recently treated a patient with lipomatous pseudohypertrophy of the pancreas who presented with symptoms of dyspepsia. The patient had concurrent Hashimoto’s disease and marked exocrine dysfunction which was indicated by the typical imaging findings of lipomatous pseudohypertrophy of the pancreas. We herein present a report of this case with lipomatous pseudohypertrophy of the pancreas diagnosed solely by typical imaging findings and serological data.
CASE REPORT
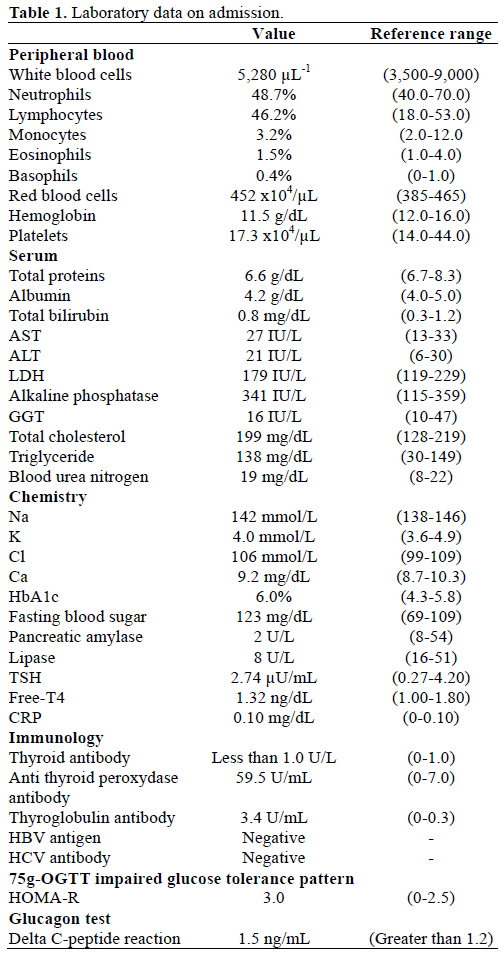
A 64-year-old female presented with epigastric abdominal pain as her principal complaint and a past history of hypothyroidism, which was diagnosed at the age of 50 years; she was undergoing treatment at a nearby clinic. Her familial history revealed that her father had colorectal cancer, her mother had thyroid disease, and her brother had esophageal cancer. The patient did not smoke or drink. For the previous two years, she had experienced an unpleasant epigastric feeling after eating oily foods. She had suffered from regular episodes of lower-back pain for the previous six months, and presented at our hospital. Computed tomography (CT) images revealed fatty replacement over the entire pancreas; hence, the patient was hospitalized for detailed examination and treatment. At the time of admission, her height was 159 cm, weight was 54 kg; and body-mass index was 21.6 kg/m2. Furthermore, physical examination did not show any abnormalities. Hematology and serum chemistry analysis (Table 1) revealed normal levels of white blood cells and platelets, mild anemia, normal levels of total protein, albumin and hepatobiliary enzymes, and a marked decrease in pancreatic amylase and lipase levels. Pancreatic exocrine function determined by an N-benzoyl-tyrosyl-p-aminobenzoic acid (BT-PBA) test was substantially low at 28.1%. The 75-gram oral glucose tolerance test (OGTT) revealed a borderline diabetic pattern; however, the preprandial blood glucose level was normal and HbA1c was slightly elevated to 6.0%. Endocrine insulin secretion determined by the glucagon tolerance test was within the normal range, with a delta C-peptide reaction of 1.5 ng/mL
An esophagogastroduodenoscopy showed normal findings. Diseases such as reflux esophagitis and gastric ulcer were not observed. Ultrasonography (Figure 1) revealed a markedly heterogeneous pancreatic parenchyma demarcated from the neighboring tissues. The main pancreatic duct was not narrowed or dilated, and no tumor was detected. A CT image is shown in Figure 2. Plain CT (Figure 2a) revealed that the density of the pancreatic parenchyma had uniformly decreased to the same level as that of the surrounding fatty tissue. Contrast-enhanced CT (Figure 2b) revealed that the entire pancreatic parenchyma was absent and only a contrast-enhancing net-like shadow was visible. The magnetic resonance imaging (MRI) image is shown in Figure 3. The T1-weighted image could confirm that the entire pancreas was completely absent on T1-weighted images (fat suppression) (Figure 3). Endoscopic retrograde cholangiopancreatography (ERCP; Figure 4) showed no anomalous arrangement of the pancreaticobiliary ducts or pancreatic duct anomaly. Furthermore, obstruction, narrowing or dilatation of the main pancreatic duct was not observed. The branches of the pancreatic ducts appeared normal on the ERCP image. No abnormalities were observed in the bile duct.
Figure 1. Ultrasonography. The pancreatic parenchyma is markedly
heterogeneous and demarcated from the neighboring tissues by a
hazy borderline. The main pancreatic duct is not narrowed or
enlarged, and no space-occupying lesion is visible.
Figure 2. Computed tomography. a. Plain: the density of the
pancreatic parenchyma is uniformly decreased to the same level as
that of the surrounding fatty tissue. b. Contrast-enhanced: the entire
pancreatic parenchyma is absent and only a contrast-enhancing netlike
shadow is observed.
Figure 3. Magnetic resonance imaging. a. T1-weighted image. b. T1-
weighted image (fat suppression): the entire pancreas is completely
absent.
Figure 4. Endoscopic retrograde cholangiopancreatography: There is
no anomalous arrangement of the pancreaticobiliary ducts or any
anomaly of the pancreatic ducts. Obstruction, narrowing or dilatation
of the main pancreatic duct is not observed. The pancreatic duct
branches appear normal. No abnormalities of the bile duct are
observed.
On the basis of the above findings, we diagnosed the case as lipomatous pseudohypertrophy of the pancreas for the following reasons: the entire pancreas was substantially replaced with fat and pancreatic exocrine dysfunction was noted while pancreatic endocrine function was maintained; moreover, no anomaly of the pancreatic duct or obstruction of the main pancreatic duct was found. Since the patient showed the signs and symptoms of pancreatic exocrine dysfunction, we started treatment with an appropriate dose of digestive enzymes (berizyme 6 g/day and pancreatin 6 g/day). The patient showed improvement and is now receiving treatment at the outpatient clinic.
DISCUSSION
The replacement of the entire pancreas with increasing amounts of adipose tissue and the consequent enlargement of the pancreas were first described by Hantelmann [1] in 1931. This disease was later named lipomatous pseudohypertrophy of the pancreas. Siegler [2] characterized lipomatous pseudohypertrophy of the pancreas as follows: 1) increase in the size and weight of the pancreas and morphologically uniform enlargement of the pancreas; 2) almost complete absence of the pancreatic exocrine tissue due to pathological replacement with adipose tissue; and 3) preservation of the system of ducts and islets.
Lipomatous pseudohypertrophy of the pancreas might be caused by viral infection and an abnormal metabolism [3], but the specific etiology remains unknown due to the very low number of cases. Complication with chronic hepatic disease is relatively common, and only a few researchers have confirmed the association between lipomatous pseudohypertrophy of the pancreas and hepatic illness [4, 5, 6]. However, some patients do not have any hepatic disorders, as in this case, and therefore, further investigation of this topic is required.
When making a differential diagnosis, the following disorders need to be considered in relation to lipomatous pseudohypertrophy of the pancreas: obesity, diabetes and age-related pancreatic fat infiltration. Olsen [7] investigated the autoptic findings of 349 cases and observed that different levels of pancreatic fat infiltration were present in all cases, indicating that pancreatic infiltration is associated with aging and obesity. Many patients with diabetes often show similar fat infiltration. However, the imaging findings of these patients revealed a remnant pancreatic parenchyma with uneven fat infiltration, which is different from the uniform fatty replacement obtained in the present case. Meanwhile, fatty replacement associated with the obstruction of the main pancreatic duct induced by pancreatic cancer or chronic pancreatitis should be distinguished from lipomatous pseudohypertrophy of the pancreas. In the present case, ERCP did not reveal any narrowing or obstruction of the main pancreatic duct, and CT, MRI and endoscopic ultrasonography did not indicate any tumor in the pancreas. Further, liposarcoma should also be distinguished from lipomatous pseudohypertrophy of the pancreas; factors such as the presence/absence of jaundice, morphological uniformity/non-uniformity, and imaging of the pancreatic ducts are useful in identifying lipomatous pseudohypertrophy of the pancreas.
Lipomatous pseudohypertrophy of the pancreas was originally discovered and reported in many young patients [1, 3]; however, in recent years, middle-aged and elderly people have commonly been reported to have lipomatous pseudohypertrophy of the pancreas [5, 8, 9]. In several patients, lipomatous pseudohypertrophy of the pancreas was diagnosed during autopsy or surgery [1, 3, 4, 5, 6, 8, 9, 10, 11]. In our case, lipomatous pseudohypertrophy of the pancreas was diagnosed by CT and MRI which showed typical images of fatty replacement over the entire pancreas. Given the recent advances in diagnostic imaging technology, additional cases of lipomatous pseudohypertrophy of the pancreas patients will be able to be diagnosed by imaging examinations, as in our case. It is important to confirm that the pancreatic ducts appear normal in CT and MRI images and no abnormality be detected in ERCP. Further, more pancreatic endocrine/ exocrine function test results should indicate more damage to pancreatic exocrine function as compared to endocrine function. Until now, few cases with malignant diseases have been reported. Altinel et al. have recently reported five cases of lipomatous pseudohypertrophy of the pancreas [12], but information about the main pancreatic duct was not noted. In this report, 4 patients underwent surgical resection, 3 of whom were diagnosed preoperatively as having ductal adenocarcinoma. The differences between lipomatous pseudohypertrophy of the pancreas and pancreatic cancer will have to be examined and compared when more case reports are available.
Since lipomatous pseudohypertrophy of the pancreas is a benign disease, follow-up observation is the basic approach after diagnosis. However, considerable pancreatic exocrine dysfunction is often present in lipomatous pseudohypertrophy of the pancreas, and certain symptoms may be induced as observed in this case. An appropriate dose of digestive enzymes should be prescribed for such patients. Furthermore, since the cause of lipomatous pseudohypertrophy of the pancreas is unknown and there have been few reports, periodic and strict follow-up observation is considered important. In conclusion, we have reported a case of lipomatous pseudohypertrophy of the pancreas presenting with indigestion, marked impairment of pancreatic exocrine function, and demonstrating typical imaging findings of lipomatous pseudohypertrophy of the pancreas. It has been suggested that the diagnosis of lipomatous pseudohypertrophy of the pancreas be based on histological findings, but this case has indicated the possibility that lipomatous pseudohypertrophy of the pancreas may be diagnosed solely by typical imaging findings and serological data.
Conflict of interest
The authors have no potential conflict of interest
References
- Hantelmann W. Fettsucht und Atrophie der BauchspecicheldrusebeiJungendlichen. Virchows Arch 1931; 282:630-42.
- Siegler DI. Lipomatouspseudohypertrophy of the pancreas associated with chronic pulmonary suppuration in an adult. Postgrad Med J 1974; 50:53-5. [PMID 4464502]
- Hoyer A. Lipomatouspseudohypertrophy of the pancreas with complete absence of exocrine tissue. J PatholBacteriol 1949; 61:93- 100.
- Yoshimura N, Hayashi S, Fukushima Y. Diffuse Mallory bodies in the liver, diffuse Lewy bodies in the brain and diffuse fat replacement (lipomatouspseudohypertrophy) of the pancreas in a patient with juvenile Parkinson's disease. ActaPatholJpn 1992; 42:826-31. [PMID 1471530]
- Sasaki M, Nakanuma Y, Ando H. Lipomatouspseudohypertrophy of the pancreas in a patient with cirrhosis due to chronic hepatitis. PatholInt 1998; 48:566-8. [PMID 9701022]
- Kuroda N, Okada M, Toi M, Hiroi M, Enzan H. Lipomatouspseudohypertrophy of the pancreas: further evidence of advanced hepatic lesion as the pathogenesis. PatholInt 2003; 53:98-101. [PMID 12588437]
- Olsen TS. Lipomatosis of the pancreas in autopsy material and its relation to age and overweight.ActaPatholMicrobiolScandA 1978; 86:367-73. [PMID 716899]
- Nakamura M, Katada N, Sakakibara A, Okumura N, Kato E, Takeichi M, et al. Huge lipomatouspseudohypertrophy of the pancreas. Am J Gastroenterol 1979; 72:171-4. [PMID 474558]
- Bralet MP, Terris B, Brégeaud L, Ruszniewski P, Bernades P, Belghiti J, Fléjou JF. Squamous cell carcinoma and lipomatouspseudohypertrophy of the pancreas.Virchows Arch 1999; 434:569- 72. [PMID 10394894]
- Robson HN, Scott GB. Lipomatouspseudohypertrophy of the pancreas.Gastroenterology 1953; 23:74-81. [PMID 13021337]
- Beresford OD, Owen TK. Lipomatouspseudohypertrophy of the pancreas. J ClinPathol 1957; 10:63-6. [PMID 13406076]
- Altinel D, Basturk O, Sarmiento JM, Martin D, Jacobs MJ, Kooby DA, Adsay NV. Lipomatouspseudohypertrophy of the pancreas: a clinicopathologically distinct entity. Pancreas 2010; 39:392-7. [PMID 19904221]





