Raffaele Pezzilli, Roberto De Giorgio, Rosa Ceciliato, Davide Campana, Lydia Piscitelli, Paola Tomassetti, Roberto Corinaldesi
Department of Internal Medicine and Gastroenterology, Sant’Orsola-Malpighi Hospital. Bologna, Italy
- *Corresponding Author:
- Raffaele Pezzilli,
Dept. of Internal Medicine and Gastroenterology
Sant’Orsola-Malpighi Hospital 40138
Bologna Italy
Phone +39-051.636.4148
Fax +39-051-549.653
E-mail pezzilli@orsola-malpighi.med.unibo.it
Received: 03 January 2004 Accepted: 16 January 2004
Keywords
Diagnostic Imaging; Hypercalcemia; Lymphoma; Pancreatic Diseases; Pancreatic Neoplasms
Question
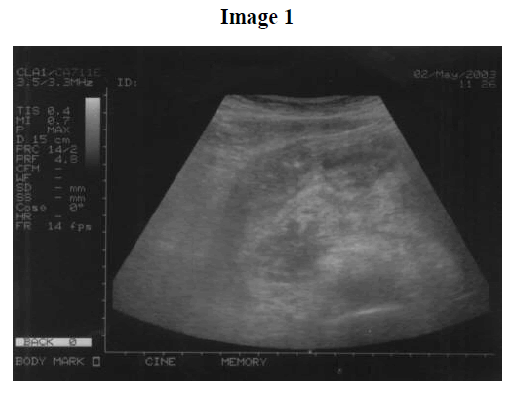
A 54 year-old man was admitted for a recent onset of epigastric pain radiated to the back. His clinical history was unremarkable. On admission, laboratory findings revealed leukocyte count of 17.18 103/μL, hemoglobin of 11.1 g/dL, hematocrit 32.2%, ESR of 11 mm/h, amylase 2,540 IU/L (reference values: 0-220 IU/L), lipase 2,820 IU/L (reference values: 0-270 IU/L). Abdominal examination revealed a tender, palpable epigastric mass. Thoracic and cardiovascular system were normal. An abdominal ultrasonography showed an abnormal pancreatic echotexture with a mass localized to the head of the gland (Image 1). A contrast-enhanced CT scan confirmed the presence of a retroperitoneal mass involving the head of the pancreas (Image 2).

During hospitalization the patient developed hypercalcemia (16.6 mg/dL), which was treated medically, and the abdominal pain persisted although serum pancreatic enzymes progressively decreased. An ultrasoundguided biopsy of the retroperitoneal mass was performed.
What is the diagnosis?
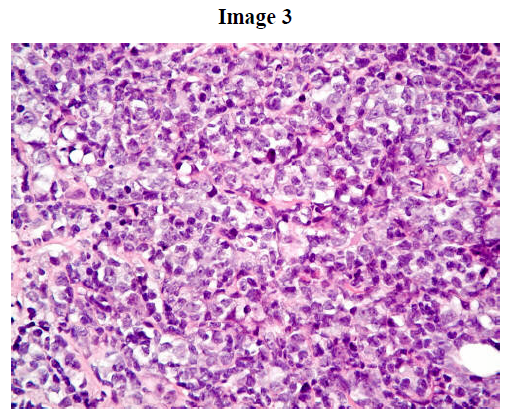
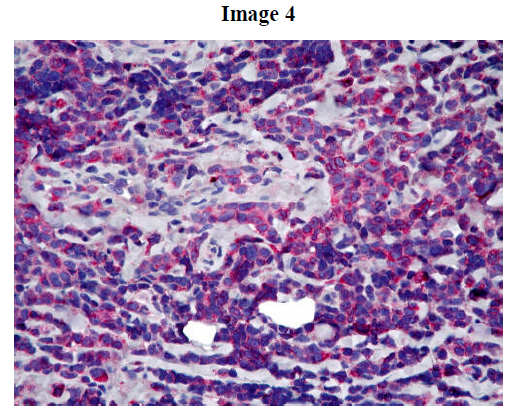
The histology of the retroperitoneal mass biopsy showed an aggressive type of T-cell lymphoma (Image 3, H&E staining) confirmed by immunohistochemical characterization revealing a lymphoid population positive for T-cell markers: CD2+, CD3+ (general marker for T lymphocytes; Image 4) and BCL2+. Both B-cell (CD20, CD79, PAX5, CD10, BCL6) and anaplastic-type (ALKc and CD30) tumoral markers were negative.
The patient was treated with a MACOP-B regimen (methotrexate, adriamycin, cyclophosphamide, vincristine, prednisone, and bleomycin), however the lymphoma progressed with central nervous system involvement and the patient died four months later.
Malignant lymphomas arising in the pancreas and/or in peripancreatic lymph nodes are rare, accounting for about 1% of non-Hodgkin lymphomas [1] and less than 0.7% of all pancreatic malignancies [2]. Clinical and diagnostic criteria to define pancreatic lymphomas have been established by Behrns et al. [3]. According to these criteria, a lymphoma localized to the pancreas is defined as a mass with involvement of peripancreatic lymph nodes, without distant lymph nodes and hepatic or splenic metastases.
References
- Freeman C, Berg JW, Cutler SJ. Occurrence and prognosis of extranodal lymphomas. Cancer 1972; 29:252-60. [PMID 5007387]
- Baylor SM, Berg JW. Cross-classification and survival characteristics of 5,000 cases of cancer of the pancreas. J Surg Oncol 1973; 5:335-58. [PMID 4355621]
- Behrns KE, Sarr MG, Strickler JG. Pancreatic lymphoma: is it a surgical disease? Pancreas 1994; 9:662-7. [PMID 7809023]

