Keywords
China, chronic disease, disabled persons, health status, primary care, risk factors
How this fits in with quality in primary care
What do we know?
The prevalence of chronic diseases in different populations is well documented. When risk factors for chronic diseases are identified early, intervention can be promoted by primary healthcare practitioners to prevent mortality and morbidity.
What does this paper add?
The prevalence of risk factors and chronic diseases has not been documented for people with disabilities in China. This preliminary report of the medical profile of disabled persons in Mainland China found that chronic illnesses and associated risk factors were not related to type or severity of disability in this sample. Most abnormal findings were related to age.
Introduction
Disabled persons are often more vulnerable, have poorer health[1] and have lower life expectancy than people without disabilities.[2] Their limited ability to self-care may lead to social exclusion and contribute to poor health.[3]
The prevalence of chronic diseases in different general populations is well documented. However, the prevalence of chronic diseases and their risk factors are less well known in disabled populations. When a person with an existing disability develops a chronic disease, the double burden of morbidity is placed not only on the individual but also on the family. Risk factors for chronic disease, if identified early, may be amenable to effective intervention and lead to reductions in morbidity and mortality.[3–5] This in turn may improve quality of life, reduce healthcare costs and reduce the economic burden on the patient and the family.[6,7]
In 2002, the China Disabled Person Federation, the national organisation for people with various types of disabilities, implemented key initiatives to ensure that all disabled persons in China have access to rehabilitation services, equal rights and an opportunity to participate in society.[8,9] As part of this initiative, Shanghai Zhabei District Disabled Persons’ Federation implemented a ‘rehabilitation service for all disabled with needs’ programme in 2004.[9] A component of this programme is a free medical assessment for all registered disabled persons in Zhabei district. The purpose of this comprehensive medical screening is to examine the ‘health’ of disabled persons in Zhabei district and identify anymedical conditions that may require further investigation, intervention or preventative action.
This free medical examination for disabled persons (classified as disabled using the International Classification of Disability, Functioning and Health) in Shanghai’s Zhabei District is currently in progress. The purpose of this paper is provide a preliminary report on the medical profile of the first 961 disabled persons who underwent the comprehensive medical examination as part of the above-mentioned programme. This study also examined the association between any abnormal findings, the type and severity of disabilities and socio-demographic factors.
Methods
Population
This cross-sectional observational study was conducted in Zhabei district in North Central Shanghai. Zhabei district has a population of about 800 00010 with 18 000 registered disabled persons.[11] Inclusion in the disabled persons registry is voluntary. Entry in the registry, however, requires physical examination by a qualified medical practitioner to certify and classify the type and severity of the disability. In this study, disability was classified using the International Classification of Functioning, Disability and Health[12] and included various categories of impairment including visual, speech and hearing, physical, intellectual and mental. The severity of disability was also assessed and classified into four levels according to standard criteria, 11 Level 1 indicating the most severe, Levels 2 and 3 moderately severe to moderate and Level 4 representing mild.
Participants
In 2008, Zhabei District Disabled Persons’ Federation conducted a needs analysis of 10 311 registered disabled persons living in the district.[13] Using this database, registered residents in Zhabei District were invited, in batches according to their registration number, to attend the nearest community health centre for physical examination.
All people registered with a disability were eligible for a physical examination except those who were hospitalised and the severely ill (bedridden).The medical examinations for the disabled were to be conducted over five years, from 2008 to 2012. This paper reports the results of the first 961 disabled persons who were examined in 2008.
Physical examinations
Registered disabled persons were examined at one of eight community health service centres located in the district between May and October 2008. The physical examination included chest X-ray, blood test (uric acid, blood glucose, total cholesterol and triglycerides) and electrocardiogram and ultrasound scans of the liver, gallbladder, spleen and kidneys. Any pre-existing medical conditions and abnormalities in the medical examination were noted by doctors, who summarised the results of the medical examination onto a standardised form. This form included demographic data such as the person’s gender, age, marital status, education level, employment status, socio-economic status (if receiving a minimum living allowance from the government), disability type and the severity of the disability. Any changes in the person’s medical and social conditions were also updated at this medical examination. This form was later archived at the Disabled Person Rehabilitation Service Guidance Center.
Abnormal chest X-rays were defined as: changes in pulmonary markings, old tuberculosis calcification, aortic cardiac changes and thoracic deformity. Evidence of myocardial ischaemia, ST-T change, T wave change, bradycardia, tachycardia, ST wave change, arrhythmia, ischaemia, low voltage, high voltage and conduction blockade were classified as abnormal electrocardiogram findings. Ultrasonographic diagnosis of fatty liver, macrovesicular hepatic fat infiltration and presence of hepatic cyst were classified as liver abnormality. [14] Presence of gallstone(s), thickening of gallbladder wall, gallbladder polyps and cholecystitis were classified as gallbladder abnormalities. Kidney abnormality was defined as having renal calculus or renal cyst and splenomegaly was considered an abnormal finding.
Predisposing conditions to chronic diseases, in particular hypertension, elevated blood glucose, lipids and triglyceride levels were diagnosed using standard criteria.[15] Adult hypertension was defined as systolic blood pressure �140 mmHg and (or) diastolic pressure �90 mmHg; elevated blood glucose was defined as levels exceeding the normal range of 3.9 to 6.1mmol/L (70�110 mg/dl) and elevated triglyceride and lipid were defined as levels exceeding 2.26 mmol/L(>200 mg/ dl) and 6.21 mmol/L(� 240 mg/dl) respectively.
Two common chronic diseases, heart diseases and diabetes were also identified. Heart disease included cardiovascular diseases such as cardiac arrhthymias and coronary atherosclerosis (coronary heart disease). Diagnoses were based on clinical manifestations or/ and ECG findings.[16] The diagnosis of diabetes was based on the criteria recommended by the WorldHealth Organization (2006): fasting plasma glucose�7.0mmol/L or 2-h blood plasma glucose�11.1 mmol/L orOGTT- 2h <11.1 mmol/L.[17]
Data analysis
Demographic data, results of the physical examination and chronic disease status were derived from the standardised forms from the eight health community centres. The use of this database was approved by the Human Research Ethics Committee of Fudan University, Shanghai, China. Data entry was validated using the double-entry technique. All statistical analyses were performed with SPSS software (Version 15; SPSS, Chicago, IL, USA). Descriptive statistics are provided to present the demographic profile of the disabled and the prevalence of abnormal physical examination findings, prevalence of risk factors for chronic diseases such as hypertension, elevated glucose, lipids and triglyceride levels and prevalence of heart disease and diabetes. Any unspecified categories for age, disability type, disability level, education level, employment status, socio-economic status and marital status were treated as missing values. Chi-squared tests or Fisher’s exact tests were used to test the differences in distribution of disability types by participants’ demographic characteristics and to assess the differences between age group, gender, disability type and disability level for each abnormalfinding and major chronic disease. Backwards stepwise logistic regression was used to assess the influence of age, gender, disability type, disability level, education level, employment status, socio-economic status or marital status on the prevalence of risk factors identified and chronic diseases diagnosed. The final model of the regression analysis for each condition was reported. All statistical tests were two-tailed; probability values of less than 5% were considered significant.
Results
Socio-demographic data
The average age of those screened was 53 (12.5) years. The socio-demographic characteristics of the subjects are shown in Table 1. There were similar proportions of males (52%) and females (48%) (P=0.32). The majority of subjects were between 40 and 59 years of age (64%), were married (70%) and were not on the minimum allowance support (87%). Most were retired from paid employment (63%), and the majority (52%) had junior high school (Year 7 to Year 9) education.

In this sample, 44.9% had physical disability, followed by visual impairment (28.8%) and intellectual disability (12.5%). Most disabled persons (72.9%) were classified as having a moderate level of severity (Level 2 and 3) (Table 1).
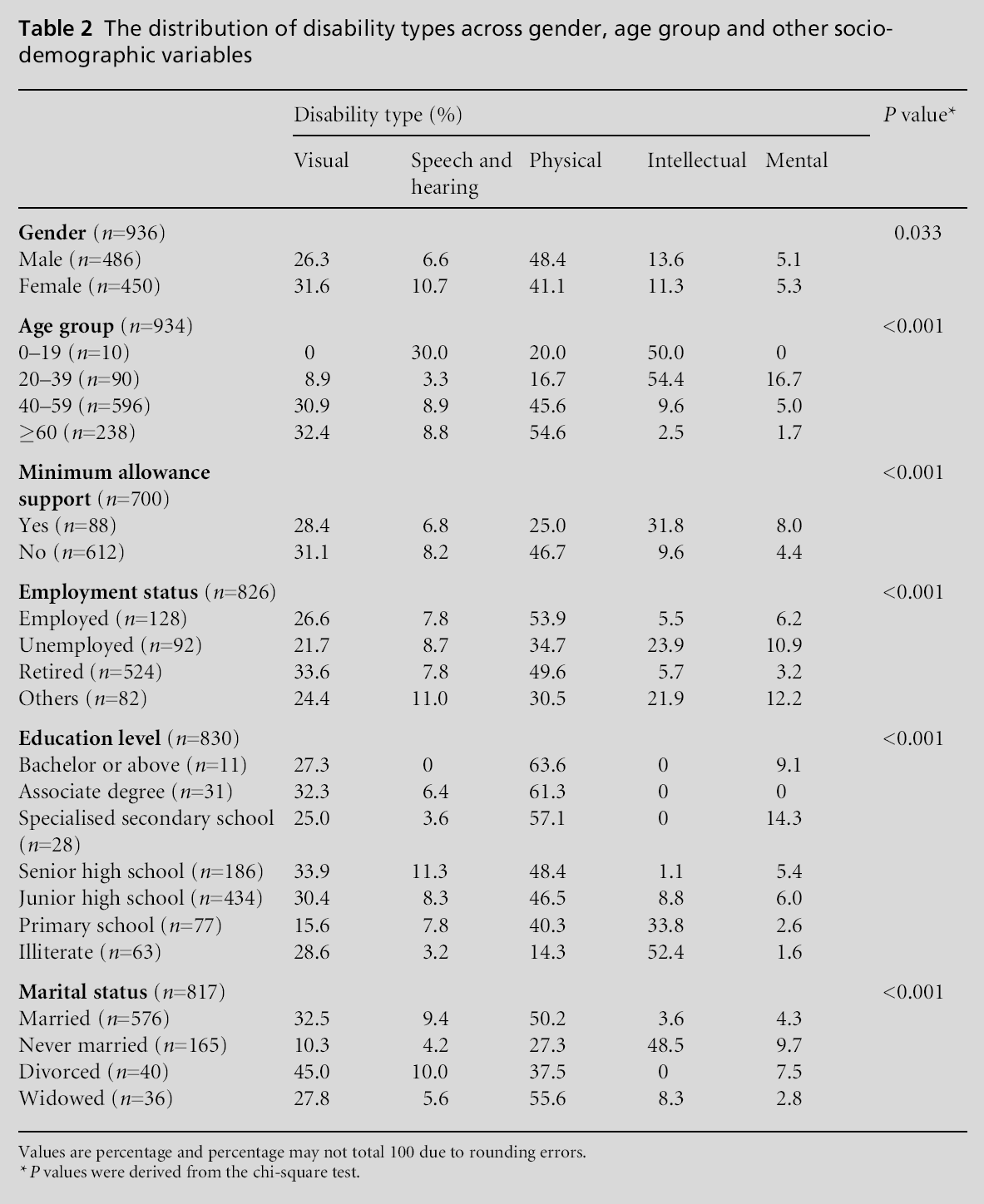
There were significant differences in the distribution of type of disability and gender (P=0.03); more females had visual impairment (31.6%) and speech and hearing impairment (10.7%) compared with males (26.3% visual impairment and 6.6% speech and hearing impairment, respectively). In contrast, there were more males (48.4%) than females (40.1%) with physical disability (Table 2). The differences between disability type and socio-demographic profile are summarised in Table 2.
Physical examination – abnormal results
Of the 961 people screened, 126 (13.1%) had normal findings on all tests. Table 3 presents the types and distribution of abnormal findings from the medical examination in this population. A high proportion in this sample (41%) presented with liver abnormality, which included either fatty liver, macrovesicular hepatic fat infiltration or the presence of liver cysts. Apart from chest X-ray and uric acid levels there were no significant differences for other abnormalities between genders (Table 3).

Due to the relatively small numbers in the younger age groups (0–19 years and 20–39 years) these groups were merged into one group for analyses. Results showed that those aged 60 years and above had a significantly higher prevalence of abnormal chest Xray and ECG and kidney disease than the younger groups (Table 3).
Prevalence of predisposing factors for chronic diseases
This study screened for risk factors for chronic disease such as hypertension, elevated glucose, abnormal blood lipids and triglyceride levels.3 Of the 961 people screened, 147 (15.3%) were diagnosed as having hypertension, 12.3% had an elevated glucose level, 17.1% had an elevated lipid profile and 10.6% had elevated triglyceride levels (Table 4).

The proportion of those with hypertension, elevated blood glucose and elevated triglycerides was significantly higher in those aged 60 years and above compared to the younger age groups (Table 4). The prevalence of hypertension was the highest in the physically disabled (18.6%) followed by the visually disabled (16.3%).
Prevalence of chronic diseases
Of the 278 disabled persons who had abnormal ECG, only 69 (7.2% of the 961 screened) were diagnosed with heart disease (Table 5). This was most prevalent in those aged 60 years and older (12.0%).

Blood tests suggested that 118 people had elevated blood sugar (Table 4), of whom 58 were diagnosed with diabetes (Table 5). Diabetes was diagnosed in 11.2% in the group aged 60 and above. This was significantly higher compared to other age groups (P=0.001). There were, however, no differences between gender, disability types and the severity of disability (Table 5).
Univariate factors associated with predisposing conditions to chronic diseases and chronic disease status
When all socio-demographic variables were entered into the logistic regression for the four predisposing factors for chronic diseases (hypertension, elevated glucose, lipids and triglyceride levels), males were more likely to have hypertension and elevated triglyceride levels compared to females (hypertension: OR: 1.75; 95% CI 1.05, 2.93; triglyceride levels: OR=1.84, 95% CI: 1.05, 3.20). Older persons (OR=1.04, 95% CI: 1.02, 1.07) and the unemployed (OR=4.77, 95% CI: 1.45, 15.8) were more likely to have elevated blood glucose levels compared to the younger and employed disabled, respectively. There were no socio-demographic factors associated with elevated lipid levels (Table 6).

Chronic diseases
Age and gender were not found to be associated with heart disease but divorced individuals were more likely to be diagnosed with heart disease compared with their married counterparts (OR= 3.72; 95% CI: 1.37, 10.09) (Table 6). For diabetes, those who were not on the minimum living allowance support were more likely to have this medical condition than individuals on a minimum living allowance (OR=3.09; 95% CI: 1.05, 9.15). Age was also found to be significantly associated with diabetes (OR=1.08, 95% CI: 1.04, 1.12).
Discussion
This study reports the preliminary findings of the medical profile, with particular reference to chronic diseases and their risk factors, of 961 disabled persons living in Zhabei District in Shanghai Mainland China. To our knowledge, there are no reports of this size on the general health and chronic disease status of a disabled population from other countries, therefore comparison with other disabled groups cannot be made. The results of this study will be compared with general ‘healthy’ Chinese populations rather than western general populations due to known cultural and social differences affecting health.
The most prevalent abnormal findings were related to the liver, with almost 41% having either fatty liver, macrovesicular hepatic fat infiltration or liver cysts identified during the examination. The next most prevalent finding was an abnormal ECG which was identified in 28.9% of cases. Most of the abnormal findings were, however, related to increasing age, which is consistent with previous findings in Chinese populations.[18,19]
The community prevalence of non-alcoholic fatty liver is reported to be about 15% in Chinese populations. [20] More specifically, prevalence of fatty liver in the general population in Shanghai was about 17%.[21] The relatively high proportion of liver abnormalities (41%) in this study may be due to the inclusion of relatively benign liver conditions such as hepatic cysts and the pre-cursor of fatty liver disease (macrovesicular hepatic fat accumulation) in this group and therefore direct comparisons with normal population is not possible. We acknowledge that it is not possible from these data to draw firm conclusions about the significance of these findings.
Abnormal ECG findings covered a myriad of criteria, including myocardial ischaemia, ST-T change, T wave change, bradycardia, tachycardia, ST wave change, arrhythmia, ischaemia, low voltage, high voltage and conduction blockade. However, of the 28.9% (n=278) who had abnormal ECG findings, only 7.2% (n=69) were diagnosed with heart disease. Therefore, some of these abnormal findings may have had a benign aetiology, although one cannot safely draw this conclusion.
Risk factors for chronic diseases
This study identified a number of disabled persons with risk factors which can predispose to chronic diseases such as cardiovascular diseases, Type 2 diabetes and stroke. One hundred and forty-seven disabled persons in this sample (15.3%) were diagnosed as having hypertension. A large-scale international collaborative study on cardiovascular diseases (InterASIA 2000–2001), in Chinese adults aged between 35 and 74 years, reported a prevalence rate of hypertension of 27.2% .[22] In 2008, China conducted the fourth nationwide health survey on more than 180 000 people from 56 400 households in 94 counties (cities, districts), 470 towns and 940 villages and found that the prevalence of hypertension in the general Chinese populationwas 54.9%.[23] Although our data suggests that the prevalence of hypertension in this special population is relatively lower than the general population in China, early intervention needs to be offered to these patients to further minimise the risk of cardiovascular disease, stroke and kidney diseases.[3]
A higher proportion of those with physical disability (18.9%) had hypertension compared to those with other types of disability, although there were no significant differences between groups. Increasing physical activity is commonly recommended as a management for hypertension and other chronic diseases.[3] Rehabilitation services for disabled persons need to be aware of this since those with physical disabilities are less mobile and less physically active and therefore adaptive equipment, devices or specially organised activities may be required to enable them to increase their physical activity levels.
This study found that those aged 60 years and above were more likely to be hypertensive and have elevated blood glucose and triglyceride levels compared to the younger age groups. These findings are consistent with rates in the general Chinese population.[18,19,22,24,25]
In this study, we found that males were more likely to be hypertensive and more likely to have elevated triglyceride levels compared with females. Direct comparison with other studies in Chinese populations is not possible as most previous studies did not investigate associations between gender and disease status. However, the most recent national health survey in China showed that there was higher prevalence of hypertension in females (60.9%) compared with males (48.8%).[23]
Our data suggest that the group who were unemployed were more likely to have abnormally elevated blood glucose compared to the group who were employed. High glucose levels predisposes to Type 2 diabetes. Elevated glucose levels can be effectively modified by change of lifestyle such as diet and increasing physical activity levels. As types of disabilities and levels of severity were not associated with elevated blood glucose, other unidentified factors, such as diet and physical activity levels may have contributed to their high glucose levels and this warrants further investigation.
Chronic diseases
We found that 29 out of 241 (12%) of those aged 60 and above were diagnosed with heart disease. About 7% of the disabled aged below 40 years were diagnosed with heart disease, a proportion higher than those aged 40 to 59 years (Table 5). This is possibly due to co-morbidities present in some congenital or genetic disorders.26 This highlights the need not only to focus on heart disease diagnosis and management in the older age group but also those who are younger and especially those diagnosed with genetic or congenital disorders.
Our study indicated those who were divorced were more likely to have heart disease compared to those who were married or widowed. This finding, in part, supports the longitudinal study ‘40 Years of the Charleston Heart Study’ which reported that divorced people faced a higher risk of mortality compared to those who were never divorced or separated.27
The InterASIA study in 2004 reported the prevalence of Type 2 diabetes in Chinese adults to be 5.5%28 and the prevalence of Type 2 diabetes in Chinese adults aged 15–74 years in Shanghai was 8.6%.29 In this study, 6% of the 961 disabled people screened were diagnosed with diabetes using the standardised WHO classification. This figure is similar to the general population across China. This study found that those who are older were more likely to have diabetes, consistent with the general Chinese population in Henan province.[19]
The Chinese Government provides a minimum income allowance for those disabled with no other means of support such as those without family, with no immediate relatives and with no employment or income.[30] In this study, a large proportion of the disabled (87%) were not on the minimum allowance benefit indicating that they were financially better off than those who received a minimum living allowance from the government. In this study, those who were financially better off were more likely to be diagnosed with diabetes compared with the lower income group. This finding warrants further investigation and may be related to a more fatty diet associated with greater affluence. However, this has not been demonstrated conclusively in this observational study.
All physical examinations of disabled persons in this study were conducted at community health centres and therefore may have excluded the very elderly, those without social support or the more severely disabled individuals. The lack of correlation between severity of disability and rates of chronic disease or abnormal physical findings may therefore have limited validity in this population. It is also acknowledged that causal relationship between disability and chronic diseases is not established in this study.
Although all people registered with a disability were eligible for physical examination except those who were hospitalised and the severely ill (bedridden), the extent to which disabled persons and their families chose to remain outside this registry or decided not to participate in the physical examination is unknown. However, we believe that this study is important because; i) people included were a random selection of ‘disabled’ persons, other than those who were severely disabled and therefore unable to attend for physical examination, and ii) we hypothesised that this group would have more medical conditions recorded by the medical team than were reported in the general Chinese population.
We report that abnormal physical findings were not related to the different types of disability, nor the severity of disabilities. As in the able-bodied general population, most abnormal findings were related to age. Therefore similar approaches to preventing and treating chronic diseases may be applied to disabled populations. The disabled potentially face the double burden of disability and chronic diseases as they grow older.
Acknowledgements
We would like to acknowledge the support of Shanghai Zhabei District Disabled Persons’ Federation for this project.
Funding
Not externally funded.
Ethical Approval
This study was approved by the Human Research Ethics Committee of Fudan University, Shanghai, China.
Peer Review
Not commissioned; externally peer reviewed.
Conflicts of Interest
None.
References
- Sutton JP and DeJong G. Managed care and people with disabilities: framing the issues. Archives of Physical Medicine and Rehabilitation 1998;79:1312–16.
- Lai DJ, Lee LM and Lee ES. Effects of handicap on life expectancy: the case of China. Public Health 2000; 114:330–5.
- WHO. Preventing Chronic Diseases: a vital investment. A WHO global report. Geneva: WHO, 2005.
- Australian Institute of Health and Welfare. Prevention of Cardiovascular Disease, Diabetes and Chronic Kidney Disease: targeting risk factors. Canberra: AIHW, 2009.
- Endres M, Heuschmann PU, Laufs U and Hakim AM. Primary prevention of stroke: blood pressure, lipids, and heart failure. European Heart Journal 2011;32:545–52.
- Peters EJ, Childs MR, Wunderlich RP, Harkless LB, Armstrong DG and Lavery LA. Functional status of persons with diabetes-related lower-extremity amputations. Diabetes Care 2001;24:1799–804.
- Bodenheimer T, Wagner EH and Grumbach K. Improving primary care for patients with chronic illness. Journal of the American Medical Association 2002;288:1909–14.
- China Disabled Persons’ Federation. Rehabilitation. 2008. www.cdpf.org.cn/english/rehabilitation/content/ 2008–04/10/content_84874.htm
- Luo Z, Lu J and Yu H. Innovative Practice of Disability Rehabilitation in Shanghai. Shanghai, China: Fudan University Press, 2008.
- Shanghai Zhabei Government. Zhabei District, Shanghai Population and Family Planning. www.shzb.gov.cn/en/ index.php
- CSSD. The Second National Sample Survey of Disabled People. Shanghai, China: China Statistics Press, 2007.
- WHO. The International Classification of Functioning, Disability and Health. Geneva: WHO, 2001.
- Qian NS, Xie JY and Zheng G. Basic rehabilitation service needs of people with disability at Zhabei District in Shanghai. Chinese Journal of Rehabilitation Theory and Practice 2009;15:188–90.
- Fatty Liver and Alcoholic Liver Disease Study Group of Chinese Liver Disease Association. Diagnostic criteria of nonalcoholic fatty liver disease. ZhonghuaGanZang Bing ZaXhi. 2003;11:71.
- Medical Administration Department of Ministry of Public Health PRC. National Guide to Clinical Laboratory Procedures (3e). Dong Nan University Press, 2006.
- Chen H. The Practice of Internal Medicine (12e). Beijing, China: People’s Medical Publishing House, 2005.
- WHO. Definition and Diagnosis of Diabetes Mellitus and Intermediate Hyperglycemia: report of a WHO/IDF consultation. Geneva: WHO, 2006. www.who.int/diabetes/ publications/Definition%20and%20diagnosis%200f%20 diabetes_new.pdf
- Qing D, Li W, Hu B, Chen T, Wang W and Ma L. Epidemiological analysis on prehypertension in Beijing and Nanjing cities. Chinese Journal of Health Education 2009;25:807–10.
- Tian R, Zhao Z, Yuan H et al. Epidemiologic survey and correlation factors analysis of diabetes mellitus and metabolic syndrome inHenanprovince. Journal of Chinese Practical Diagnosis and Therapy 2009;23:1052–5.
- Fan JG and Farrell GC. Epidemiology of non-alcoholic fatty liver disease in China. Journal of Hepatology 2009; 50:204–10.
- Fan JG, Zhu J, Li XJ et al. Prevalence of and risk factors for fatty liver in a general population of Shanghai, China. Journal of Hepatology 2005;43:508–14.
- Gu D, Reynolds K, Wu X et al. Prevalence, awareness, treatment, and control of hypertension in China. Hypertension 2002;40:920–7.
- An Analysis Report of a National Health Service Survey in China, 2008. Centre for Health Statistics and Information, 2008.
- Wang R, Zhao Y, He X et al. Impact of hypertension on health-related quality of life in a population-based study in Shanghai, China. Public Health 2009;123:534–9.
- Tian H, Song G, Xie H, Zhang H, Tuomilehto J and Hu G. Prevalence of diabetes and impaired fasting glucose among 769,792 rural Chinese adults. Diabetes Research and Clinical Practice 2009;84:273–8.
- Kapell D, Nightingale B, Rodriguez A, Lee JH, Zigman WB and Schupf N. Prevalence of chronic medical conditions in adults with mental retardation: comparison with the general population. Mental Retardation 1998;36:269–79.
- Sbarra DA and Nietert PJ. Divorce and death: forty years of the Charleston Heart Study. Psychological Science 2009;20:107–13.
- Hu D, Sun L, Fu P et al. Prevalence and risk factors for type 2 diabetes mellitus in the Chinese adult population: the InterASIA Study. Diabetes Research and Clinical Practice 2009;84:288–95.
- Li R, Lu W, Jia W et al. Cross sectional investigation of prevalence of type 2 diabetes in Shanghai. Zhonghua Yi XueZaZhi 2006;86:1675–80.
- Zhang D. Policies and Effects of Poverty Reduction for the Disabled in China. 2007. conferences.ifpri.org/2020 Chinaconference/pdf/005ZhangDongmei.pdf

