Zachary Myles, MPH, Epidemiologist*
Division of Environmental Hazards and Health Effects, National Center for Environmental Health,
Centers for Disease Control and Prevention, Atlanta, Georgia, USA
Ketra Rice, PhD, MS, Prevention Effectiveness Fellow
Division of Cancer Prevention and Control, National Center for Chronic Disease
Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, USA
Amy Degroff, PhD, MPH, Program Evaluator
Division of Cancer Prevention and Control, National Center for Chronic Disease
Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, USA
Jackie Miller, MD, Medical Director
Division of Cancer Prevention and Control, National Center for Chronic Disease
Prevention and Health Promotion, Centers for Disease Control and Prevention, Atlanta, Georgia, USA
Corresponding Author:
Zachary Myles
Division of Environmental Hazards and Health Effects
National Center for Environmental Health
Centers for Disease Control and Prevention
4770 Buford Highway NE MS F60 Atlanta, GA 30341
Tel: (770) 488-3895
Fax: (770) 488-1540
E-mail: hkt4@cdc.gov
Introduction
Having a usual source of care has been strongly associated with women getting cancer screenings.[1] This study describes provider network characteristics of the Centers for Disease Control and Prevention’s (CDC’s) National Breast and Cervical Cancer Early Detection Program (NBCCEDP), the only nationally organized screening program in the United States.[2] The composition of a provider network is a significant indicator of the effectiveness of clinical service delivery.[3]
In 1991, attempting to increase screening and reduce late stage morbidity, the CDC initiated the NBCCEDP. [4] Currently implemented in all 50 states, 16 Tribes/Territories, and the District of Columbia, the NBCCEDP aims to assist low income women gain access to breast and cervical cancer screening, diagnostic, and treatment services.[4] Women are eligible for the program if they are 40-64 years of age, are at or below 250% of the federal poverty level (FPL), and are uninsured or have insurance that does not cover breast or cervical screening examinations. The NBCCEDP has served more than 4.6 million women, provided more than 11 million breast and cervical cancer screening examinations, found about 167,000 precancerous cervical lesions and has diagnosed more than 64,000 breast and over 3,500 cervical cancers.[4]
A recent supplemental issue of Cancer Causes & Control includes 16 articles demonstrating the impact of the NBCCEDP. [5] During July 2012-June 2013, the NBCCEDP provided more than 500,000 screening examinations and diagnosed approximately 6,000 breast cancers and 270 invasive cervical cancers among the program’s priority population of low-income, uninsured, and underinsured women.[6] Data on the NBCCEDP provider network were collected through a web-based survey during July 2012-June 2013. This article is the first time that details of the NBCCEDP provider network have been reported. These data are being used to better understand where services are delivered, improve program implementation, and guide program policy.
Methods
We surveyed all 67 NBCCEDP grantees about their first year (July 2012-June 2013) under a new 5-year grant cycle. Information Management Systems (IMS), CDC’s data contractor for the NBCCEDP, administered the survey through a web-based platform in November 2013 (OMB No. 0920- 0879). Grantees reported the total number of sites or clinics that were delivering NBCCEDP screening services by setting. These settings included federally qualified health centers (FQHCs)/community health centers (CHCs), Indian Health Service (IHS)/other tribal organization sites/clinics, non-FQHC individual offices/clinics (including local health departments), health care systems/clinics associated with insurers (eg, Kaiser Permanente), and “other” sites/clinics. We computed the total number of NBCCEDP provider sites or clinics across all provider settings, conducted stratum analyses to derive summary statistics (mean, median, and range), and identified the regional distribution by setting. Grantees that reported “unknown” for all five provider settings were excluded from analysis.
Results
Table 1 presents summary statistics for the number of provider sites participating in the NBCCEDP by provider setting. Nearly all grantees completed the survey, with 64 (95.5%) reporting ≥1 provider sites or clinics in one or more provider settings identified through the survey. Forty-nine grantees (76.6%) reported delivering screening services in FQHCs/CHCs, 48 (75.0%) in individual offices/clinics, 33 (51.6%) in IHS/other tribal organization sites/clinics, 30 (44.8%) in health care systems/clinics associated with insurers, and 9 (14.1%) in other sites/clinics.
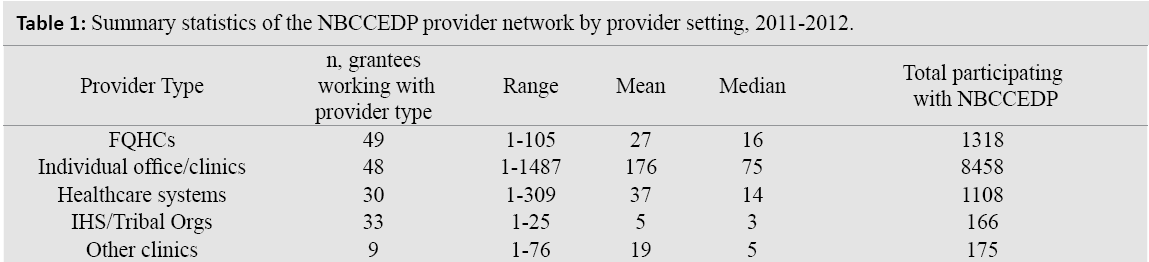
In total, 11,225 provider sites or clinics delivered NBCCEDP screening services during the year examined. NBCCEDP’s overall provider network included 1,318 (11.8%, mean = 27, median = 26, range = 1-105) FQHCs/ CHCs; 8,458 (75.3%, mean = 176, median = 75, range = 1-1,487) individual offices/clinics; 166 (0.5%, mean = 5, median = 3 range = 1-25) IHS/other tribal organization sites/ clinics; 1,108 (9.9%, mean = 37, median = 14 range = 1-309) health care systems/clinics; and 175 (1.6%; mean = 19, median = 5 range 1-76) other sites/clinics.
Regionally, grantees with the largest provider networks were in the East North Central (2,370) and South Atlantic (1,979) divisions, while grantees with the smallest provider networks were in the West South Central (255) and New England divisions (283) (Figure 1). By provider setting, FQHCs/CHCs were most common in the South Atlantic division (203), while individual offices/clinics were most common in the East North Central division (2,118). Health care systems/clinics were most common in the Mid-Atlantic division (335).
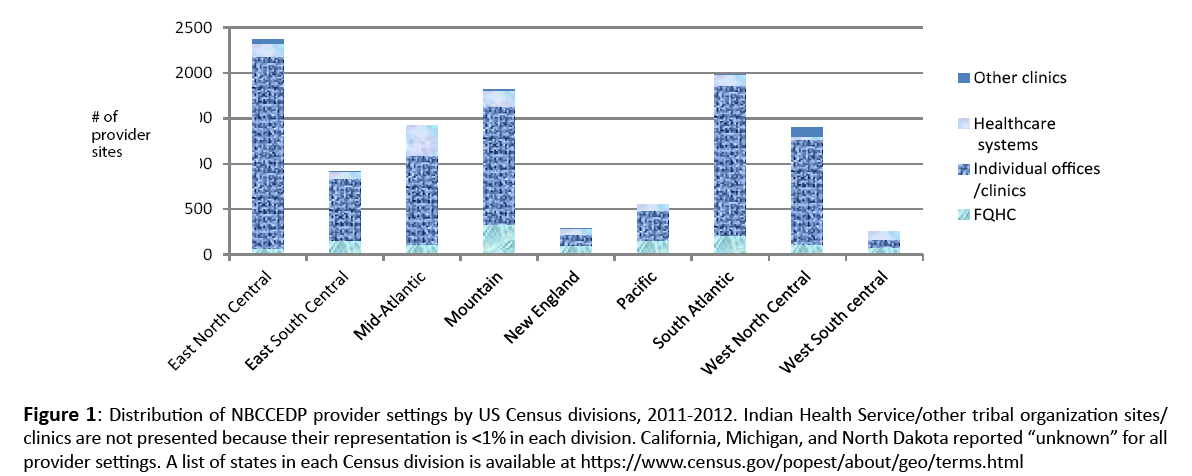
Figure 1: Distribution of NBCCEDP provider settings by US Census divisions, 2011-2012. Indian Health Service/other tribal organization sites/ clinics are not presented because their representation is <1% in each division. California, Michigan, and North Dakota reported “unknown” for all provider settings. A list of states in each Census division is available at https://www.census.gov/popest/about/geo/terms.html
Discussion
More than 11,000 provider sites delivered NBCCEDP screening services during 2012-2013, with 75% or more of grantees serving clients in FQHCs/CHCs and individual offices/ clinics and more than 50% of grantees providing screening to American Indian/Alaska Native populations through IHS/ other tribal organization sites/clinic. This finding suggests that NBCCEDP grantees are delivering services in provider sites where underserved populations are reached.
We present the NBCCEDP provider network as it was during 2012-2013, before full implementation of the Patient Protection and Affordable Care Act (ACA).[7] Enrollment into Medicaid (expanded under the ACA) and the health insurance marketplace may affect the number of women eligible for future NBCCEDP screening services, and these provider networks may change with time.
The NBCCEDP’s provider network provides an infrastructure that allows grantees to implement evidence-based strategies designed to reach health care providers and clients (eg, provider and client reminders, provider assessment and feedback).[8] These strategies can support cancer screening for thousands of people who are newly insured under the ACA.[9]
Our analysis has some limitations. First, data were provided through self-report by grantee respondents and were not verified. Three grantees (California, Michigan, and North Dakota) did not report provider site numbers. In addition, because the NBCCEDP does not cover the entire state in some areas, our results cannot be generalized to overall regions or national provider networks.
This analysis provides the first description of the NBCCEDP’s service delivery network. To increase population-level screening, Plescia et al.[2] called for collaborations between the public health community and health care providers to increase organized cancer screening programs. Through its extensive provider collaborations, NBCCEDP grantees are well-positioned to advance these relationships and encourage the implementation of evidence-based strategies, while continuing to screen populations with the greatest need.
Conflict of Interest
There are no conflict of interest disclosures to report for any author.
Acknowledgement
We recognize and thank our colleagues with Information Management Services, Inc. for their outstanding work in developing the web-based instrument and collecting and validating survey data.
Disclamer
The findings and conclusions in this manuscript are those of the authors and do not necessarily represent the official position of the Centers for Disease Control and Prevention (CDC).
References
- SelvinE, Brett KM. Breast and cervical cancer screening: sociodemographicpredictors among white, black, and Hispanic women. Am J Public Health.2003;93:618-623.
- Plescia M, Wong F, Pieters J, Joseph D. The National Breast and Cervical Cancer Early Detection Program in the era of health reform: a vision forward. Cancer. 2014;120(suppl 16):2620-2624.
- Markovitz AR, Alexander JA, Lantz PM, Paustian ML. Patient-centered medical home implementation and use of preventive services: the role of practice socioeconomic context. JAMA Intern Med. 2015; 175: 598-606.
- National Breast and Cervical Cancer Early Detection Program (NBCCEDP). About the Program. https://www.cdc.gov/cancer/nbccedp/about.html .
- Cancer Causes & Control. 2015; 26:649-809.
- National Breast and Cervical Cancer Early Detection Program (NBCCEDP).About the program.Retrieved from https://www.cdc.gov/cancer/nbccedp/about.htm.
- The Henry J. Kaiser Family Foundation. Health reform implementation timeline. Retrieved from https://kff.org/interactive/implementation-timeline/.
- Sabatino SA, Habarta N, Baron RC, et al. Interventions to increase recommendation and delivery of screening for breast, cervical, and colorectal cancers by healthcare providers: systematic reviews of provider assessment and feedback and provider incentives. Am J Prev Med 2008;35(1 suppl):S67-S74.
- Shaw FE, Asomugha CN, Conway PH, Rein AS. The Patient Protection and Affordable Care Act: opportunities for prevention and public health. The Lancet 2014; 384:75-82.

