Keywords
Autoimmune Diseases; Biological Markers; Pancreas; Pancreatic Neoplasms; Pancreatitis, Chronic
Abbreviations
AIP: autoimmune pancreatitis; CP: chronic pancreatitis; DTT: dithiotreitol; FFPE: formalin-fixed paraffinembedded; LC-MS/MS: liquid chromatography coupled with tandem mass spectrometry; PC: pancreatic cancer
Supplementary tables
Available at https://www.serena. unina.it/index.php/jop/article/view/1508/1747
INTRODUCTION
Diseases of the pancreas affect more than 1 million individuals in the United States annually, resulting in nearly $3 billion in direct and indirect medical costs [1]. Clarification of the biomolecular mechanisms of pancreatic diseases, such as pancreatitis and pancreatic cancer, is vital in identifying diagnostic biomarkers of early disease and developing targeted treatments to modify and/or retard disease progression.
Autoimmune pancreatitis is a benign idiopathic inflammatory disease of the pancreas resulting in masses and duct strictures. A recent study from Japan determined the prevalence of this rare disease to be 0.8/100,000 [2]. Another study estimated that 5-6% of patients classified previously as having idiopathic chronic pancreatitis have had diagnoses reclassified as autoimmune pancreatitis [3, 4]. Autoimmune pancreatitis may closely resemble pancreatic carcinoma, both clinically and radiographically, and thus the two pancreatic diseases can be difficult to differentiate [5, 6]. Current laboratory tests and biopsies by fine needle aspiration are limited in distinguishing the two diseases and cannot definitively rule out malignancy. In fact, over 10% of patients undergoing surgery for suspected pancreatic cancer, instead have autoimmune pancreatitis [7]. Therefore, improved diagnostic methods are needed to distinguish the two diseases. To that end, we propose a mass spectrometry-based proteomic study of formalin-fixed paraffin-embedded (FFPE) tissue for the discovery of biomarker candidates. We have applied previously similar techniques to differentiate late stage chronic pancreatitis from pancreatic cancer [8]; however, we now present the use of this technique in a more clinically relevant context that is the unmet need of distinguishing between autoimmune pancreatitis and pancreatic cancer.
Formalin fixing and paraffin embedding tissue is the standard technique for preserving specimens in hospital pathology departments. FFPE tissue banks are a rich resource for retrospective protein biomarker investigation. These types of specimens have historically been used to investigate the cellular localization of specific proteins via antibody-based immunohistochemistry [9]. Immunohistochemistry requires a priori knowledge of the proteins to be specifically targeted making it unsuitable for large-scale protein identification. State-of-the-art proteomics techniques offer an unbiased exploratory approach, which if applied to tissue repositories, may enhance our understanding of pancreatic disease pathogenesis and pathophysiology, potentially identifying novel targets for immunohistochemistry analysis.
Mass spectrometry-based proteomics is quickly becoming the model strategy for unbiased largescale protein investigation [10]. Archived FFPE pancreatic tissue specimens offer a robust sample set with which to investigate altered biochemical pathways and uncover potential biomarkers of pancreatic disease. Analogous techniques have been applied previously to FFPE tissues from various organs [11]. The major objectives of this proteomic investigation are: 1) to identify proteins present in FFPE pancreatic tissue using liquid chromatography-coupled with tandem mass spectrometry (LC-MS/MS), and 2) to compare the proteomic profiles of autoimmune pancreatitis, chronic pancreatitis, and pancreatic cancer FFPE pancreas tissue specimens. To our knowledge, we report the first comparison of FFPE pancreas tissue from autoimmune pancreatitis, chronic pancreatitis, and pancreatic cancer.
METHODS
Study Design and Setting
Proteomic analysis of archived formalin-fixed paraffin-embedded (FFPE) pancreas tissue in an academic center.
MATERIALS
FFPE tissue specimens were provided by Dana- Farber/Harvard Cancer Center (Boston, MA, USA). Heptane (product #51750) was from Sigma-Aldrich (St. Louis, MO, USA). Pep-clean C18 spin columns (product #89870) were from Thermo Scientific (Waltham, MA, USA). Sequencing-grade modified trypsin (V5111) was obtained from Promega (Madison, WI, USA). Other reagents and solvents were purchased from Sigma-Aldrich (St. Louis, MO, USA) and Burdick & Jackson (Morristown, NJ, USA), respectively.
Formalin Fixing and Paraffin Embedded of Pancreatic Tissue
FFPE tissue specimens were fixed in 10% neutral-buffered formalin for 48 h (Dana- Farber/Harvard Cancer Center, Research Pathology Core Laboratory). Routine paraffin treatment was performed as follows: specimens were treated twice with 70% ethanol for 45 minutes, twice with 80% ethanol for 60 minutes, twice with 95% ethanol for 60 minutes, thrice with 100% ethanol for 60 minutes, twice with #83 xylene substitute for 60 minutes, and twice with paraffin for 60 minutes. Tissue sections of 5 μm thickness were cut from the FFPE whole-mount pancreatic tissue block, mounted on standard glass slides, and heated for 60 min at 60°C. Slides were stored at room temperature until use.
Experimental Workflow
The experimental analysis is outline in Figure 1: 1) FFPE tissue specimens were obtained from the Dana-Farber/Harvard Cancer Center core facility; 2) a 1.5 cm x 1 cm x 5 μm slice of the FFPE tissue was scraped from the slide into a microcentrifuge tube; 3) paraffin was removed with heptane; 4) disulfide bonds were reduced with dithiotreitol (DTT) and alkylated with iodoacetamide; 5) sample was digested overnight with trypsin; 6) peptides were isolated with C18 spin columns; 7) LC-MS/MS analysis was performed; and 8) database searching and bioinformatics processing was performed.
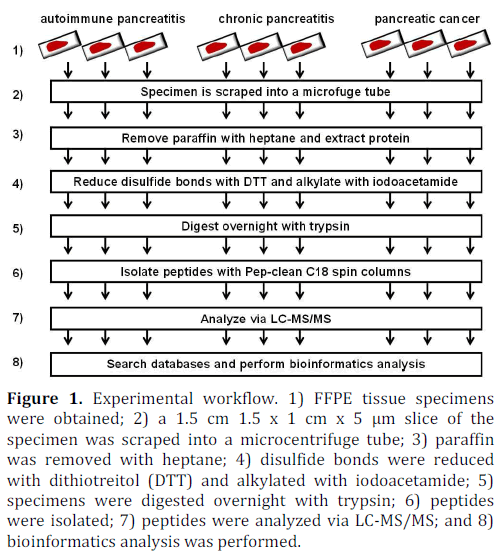
Figure 1. Experimental workflow. 1) FFPE tissue specimens were obtained; 2) a 1.5 cm 1.5 x 1 cm x 5 μm slice of the specimen was scraped into a microcentrifuge tube; 3) paraffin was removed with heptane; 4) disulfide bonds were reduced with dithiotreitol (DTT) and alkylated with iodoacetamide; 5) specimens were digested overnight with trypsin; 6) peptides were isolated; 7) peptides were analyzed via LC-MS/MS; and 8) bioinformatics analysis was performed.
Sample Preparation for Mass Spectrometry Analysis
The sample preparation protocol for mass spectrometry analysis was assembled from several sources [11, 12, 13, 14, 15]. After removing the excess paraffin from the tissue slice, the FFPE pancreatic tissue specimen from each glass slide was scraped, using a clean razor blade, into a 2 mL microcentrifuge tube. To remove the remaining paraffin, 0.5 mL of heptane was added to each sample, followed by vigorous vortexing for 10 seconds and incubation at room temperature for 1 h. Twenty-five microliters of methanol was then added to each tube, followed by vigorous vortexing for 10 seconds and centrifugation (20,000 g for 2 min at 4°C). Immediately following centrifugation, the upper (heptane) layer was discarded and the lower layer was allowed to evaporate. Proteins were then extracted by resuspending the dried material in 250 μL of 6 M guanidine-HCl/50 mM ammonium bicarbonate/20 mM DTT, pH 8.5, briefly sonicating, and incubating at 70°C for 1 h. After cooling to room temperature, iodoacetamide was added to a final concentration of 40 mM and the sample was incubated in the dark for 1 h. The alkylation reaction was quenched by adding 3 μL of 2 M DTT.
In preparation for tryptic digestion, the sample was diluted 1:6 with 50 mM ammonium bicarbonate (pH 8.1) to reduce the concentration of guanidine-HCl to 1 M. Each sample was incubated with 2.5 μg of trypsin. Following the incubation, the reaction was acidified with formic acid to a final concentration of 0.1% and evaporated via vacuum centrifugation. To remove substances which may interfere with mass spectrometry, peptides were isolated with C18 spin columns according to the manufacturer’s instructions. Samples were again vacuum centrifuged until dry and stored at -80°C until analysis. Immediately prior to analysis, the peptides were resuspended in sample loading buffer (5% formic acid, 5% acetonitrile, 90% water).
Mass Spectrometry
Mass spectrometry analysis was performed at the Proteomics Center at Children’s Hospital Boston, MA, USA. The resuspended peptides were fractionated using reversed-phase high pressure liquid chromatography (HPLC; Thermo Scientific, Waltham, MA, USA) and the gradient-eluted peptides were analyzed using an LTQ FT Ultra mass spectrometer (Thermo Scientific, Waltham, MA, USA). The liquid chromatography columns (15 cm x 100 μm inner diameter) were packed in-house with Magic C18 (5 μm, 100 Å; Michrom BioResources, Auburn, CA, USA), into PicoTips (New Objective, Woburn, MA, USA). Samples were analyzed with a 90 minute linear gradient (0-35% acetonitrile with 0.2% formic acid) and data were acquired in a datadependent manner, in which MS/MS fragmentation was performed on the six most intense peaks of every full MS scan.
ETHICS
The study was approved by our Institutional Review Committee. This protocol was approved by the Institutional Review Board at Brigham and Women’s Hospital and Children’s Hospital Boston (IRB # 2007-P-002480/1).
Written informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the “World Medical Association (WMA) Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008.
STATISTICS
Bioinformatics and Data Analysis
Raw files were converted to mascot generic files (mgf) using MSconvert [16] for downstream database searching in ProteinPilot (v.4; AB SCIEX, Foster City, CA, USA). All data generated were searched against the UniProt human database (downloaded November 11, 2011) using the Paragon algorithm [17], which is integrated into the ProteinPilot search engine. Search parameters were set as follows: 1) sample type: identification; 2) Cys alkylation: iodoacetamide; 3) instrument: Orbitrap/FT (1-3 ppm) or LTQ FT Ultra mass spectrometer (Thermo Scientific, Waltham, MA, USA) MS/MS; 4) special factors: none; 5) identification focus: none; 6) database: UniProt human; and 7) search effort: thorough identification. A 1% false discovery rate (FDR) for protein identifications was determined using the Posterior Error Probability algorithm integrated into ProteinPilot. Relative protein quantification was performed using label-free spectral counting, which compared the number of identified tandem mass spectra for the same protein across multiple data sets [18, 19].
RESULTS
Proteomic Analysis of FFPE Tissue Identified Several Hundred Proteins Using Mass Spectrometry-Based Proteomic Techniques
FFPE tissue from nine histologically-classified archived specimens (autoimmune pancreatitis, n=3; chronic pancreatitis, n=3; and pancreatic cancer, n=3) were subjected to mass spectrometry-based proteomic analysis, as depicted in Figure 1. The analysis of each specimen, was performed using a single 1.5 cm x 1 cm x 5 μm slice of FFPE tissue. Mass spectrometric analysis of all 9 FFPE specimens identified a total of 386 non-redundant proteins, which we list in Supplementary Table 1. A nonredundant protein is one that has been counted only once, regardless the number of specimens in which it has been identified.
Non-Redundant Proteins Were Exclusive to Each Pancreatic Disease Cohort
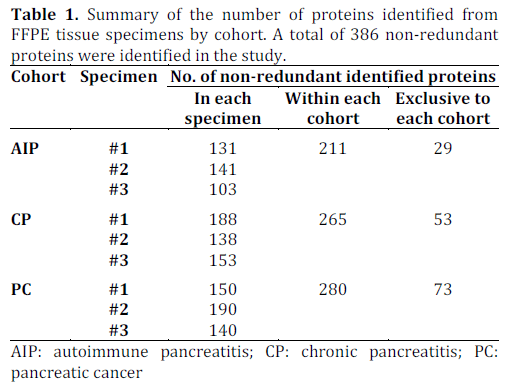
We summarize the number of non-redundant proteins identified in this study in Table 1. Considering each specimen individually, we identified 131, 141, and 103 non-redundant proteins in each autoimmune pancreatitis (AIP) specimen; 188, 138, and 153 non-redundant proteins in each chronic pancreatitis (CP) specimen; and 150, 190, and 140 non-redundant proteins in each pancreatic cancer (PC) specimen. We then merged the three lists of proteins identified in each cohort to determine the number of non-redundant proteins identified within each cohort, as listed in Table 1. The numbers of non-redundant proteins identified in each cohort were: 211 in autoimmune pancreatitis, 265 in chronic pancreatitis, and 280 in pancreatic cancer.
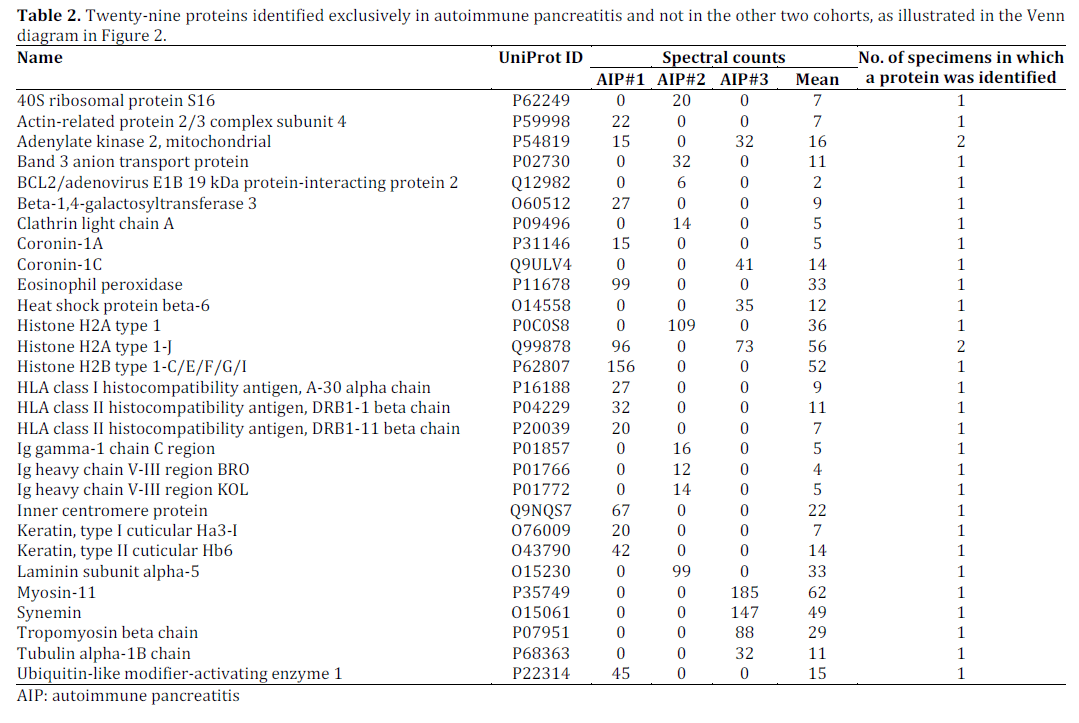
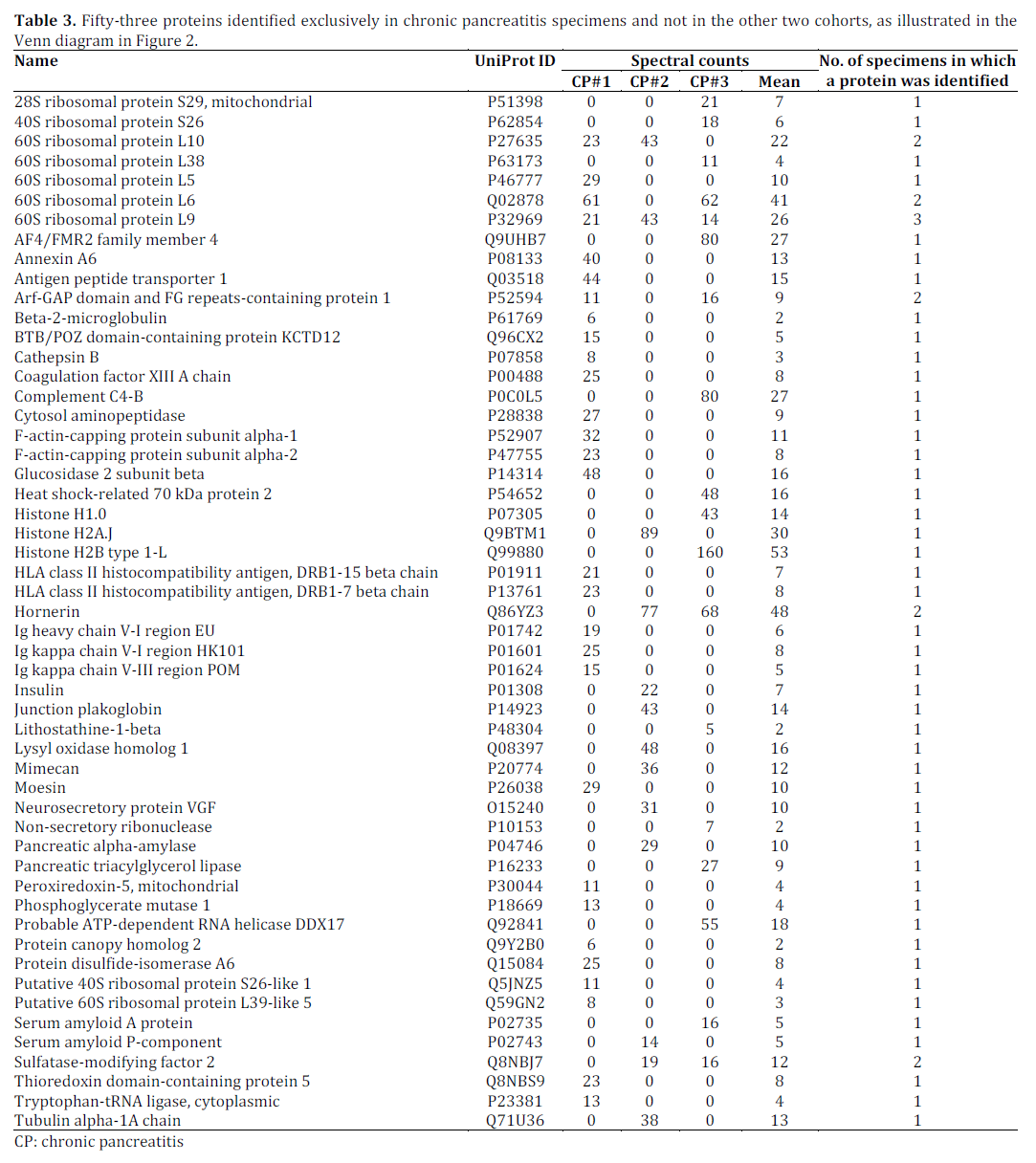
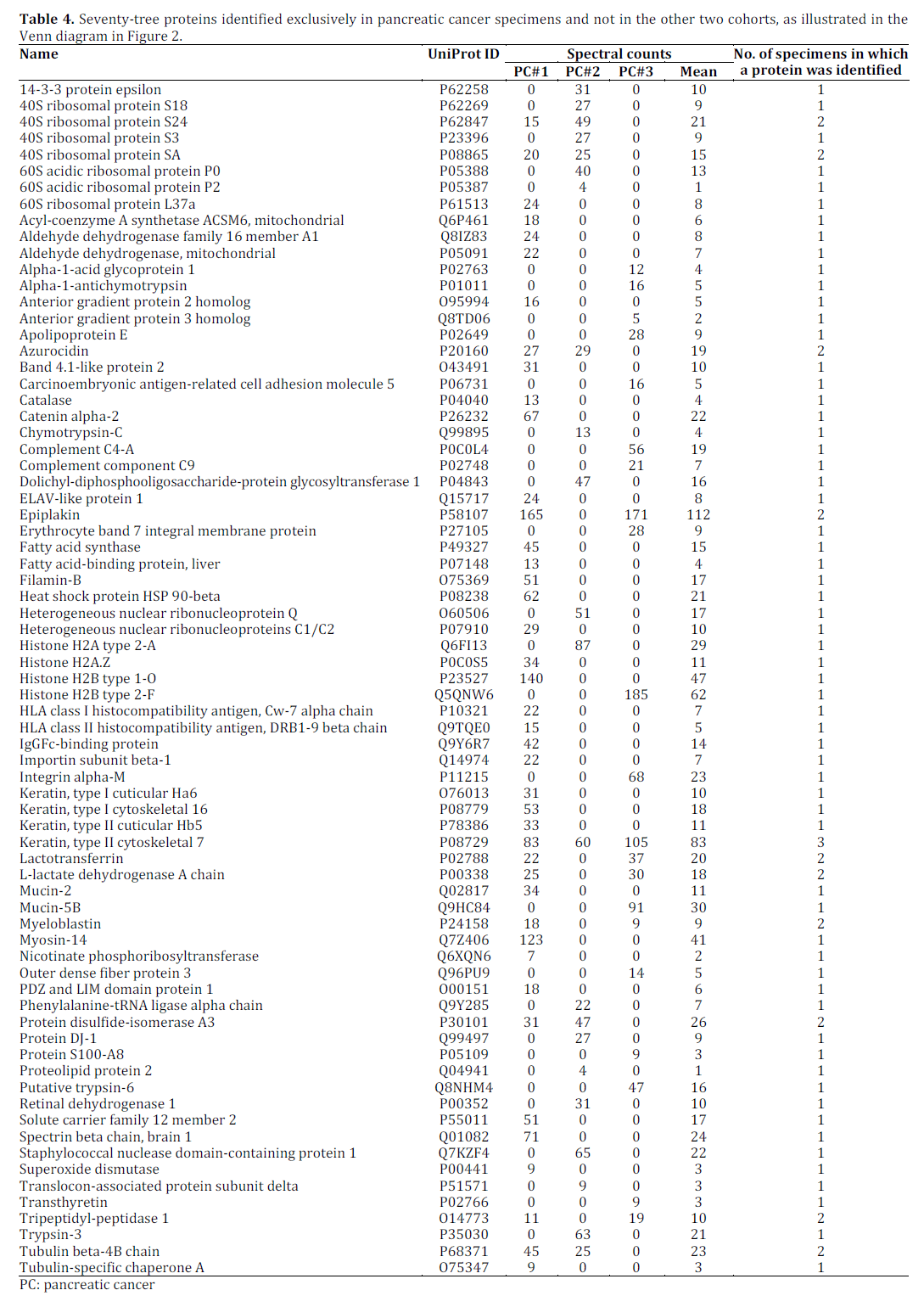
We then compared proteins among cohorts to identify those exclusive to each cohort and those common to the three cohorts (Figure 2). We identified 29 proteins exclusive to the autoimmune pancreatitis cohort (Table 2), 53 proteins exclusive to the chronic pancreatitis cohort (Table 3), and 73 proteins exclusive to the pancreatic cancer cohort (Table 4). Proteins identified exclusively in the autoimmune pancreatitis specimens include immunoglobulins and histocompatibility antigens. Epiplakin, protein disulfide-isomerase, and mucin 2 were among the proteins that were identified exclusively in the pancreatic cancer specimens. Hornerin and several ribosomal subunits were identified exclusively in the chronic pancreatitis specimens. Our analysis also identified 139 nonredundant proteins common to all three cohorts, 24 common to only autoimmune pancreatitis and chronic pancreatitis (Supplementary Table 2), 19 common to only autoimmune pancreatitis and pancreatic cancer (Supplementary Table 3) and 49 common to only pancreatic cancer and chronic pancreatitis (Supplementary Table 4).
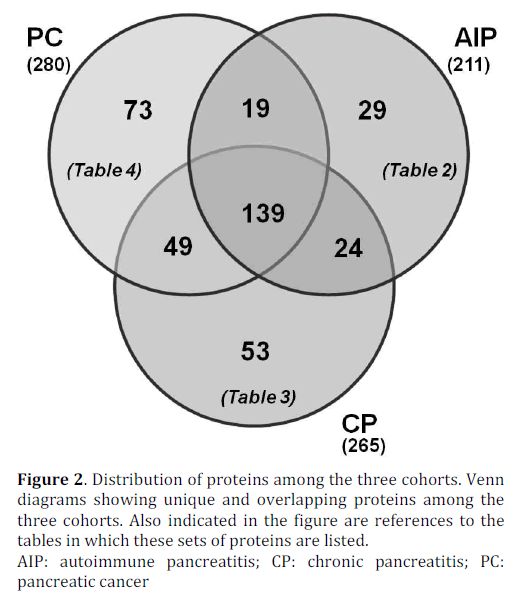
Figure 2. Distribution of proteins among the three cohorts. Venn diagrams showing unique and overlapping proteins among the three cohorts. Also indicated in the figure are references to the tables in which these sets of proteins are listed.
DISCUSSION
We have successfully applied LC-MS/MS analysis to FFPE tissue of autoimmune pancreatitis, chronic pancreatitis, and pancreatic cancer specimens. In total, we have identified 386 non-redundant proteins among all 9 specimens. By comparing these proteins, we have identified those that were found exclusively in autoimmune pancreatitis (29 proteins), chronic pancreatitis (53 proteins), and pancreatic cancer (73 proteins). A previously published study analyzed pancreatic cancer FFPE tissue using a Liquid Tissue (Expression Pathology, Rockville, MD, USA) workflow for a global proteomics analysis [20]. FFPE tissue processing techniques and mass spectrometry strategies analogous to those which we performed have been used previously to study tissues of other organ systems, including prostate [21], cochlea [14], liver [13, 22], glioblastoma [23], renal carcinoma [24], kidney glomeruli [25], mesenchymal tissue [12], and B-cell lymphoma cells [26], as well as our own recent study comparing pancreatic cancer and chronic pancreatitis [8]. We, however, present the first comparative LC-MS/MS analysis of FFPE pancreas tissue from individuals with autoimmune pancreatitis, chronic pancreatitis, and pancreatic cancer.
Our mass spectrometry-based analysis revealed several proteins as exclusive to specimens from particular cohorts and which may merit further investigation. Genetic and immunologic factors impact the pathogenesis of certain pancreatic diseases [27], and several proteins identified exclusively in a particular disease cohort may directly reflect the presence of that disease process. Histocompatibility antigen (HLA) DRB1-1 beta chain (HLA-DRB1 beta chain) may be correlated to autoimmune pancreatitis. Studies have demonstrated that HLA class II DRB1-1 beta chain allele (HLA-DRB1*0401) may have a protective role in autoimmune pancreatitis [28], while others have investigated allelic polymorphisms in the genes of the major histocompatibility complex (MHC) region, in particular HLA-DRB1*0401, suggest this allele is a susceptibility factor in patients with chronic pancreatitis [27]. Also identified exclusively in autoimmune pancreatitis, Ig gamma-1 chain (IGHG1) has been shown to down-regulate the cytotoxic activity of natural killer cells through inhibition of antibody-dependent cellular cytotoxicity [29].
Proteins identified exclusively in pancreatic cancer samples included: epiplakin, mucin2 (MUC2), and protein disulfide-isomerase A3. In a mouse model study, epiplakin was found in centroacinar cells and duct cells in the adult pancreas. Its presence has been observed in pancreatic intraepithelial neoplasia, previously identified as pancreatic ductal adenocarcinoma precursor lesions [30]. Mucins are large multifunctional glycoproteins that play an important role in the ductal structures within the pancreas. MUC2 has been shown to be expressed mainly in intraductal papillar mucinous neoplasms (IPMNs), but is occasionally also detected in aggressive pancreatic tumors [31]. Protein disulfide-isomerase A3 (ERp57) is a member of the protein disulfide-isomerase (PDI) family that is involved in the cleavage of disulfide bonds between cysteine residues. This enzyme has been implicated mainly in Alzheimer’s disease, but also has been associated with the pathogenesis of cancers, including pancreatic cancer [32]. Hornerin and several ribosomal subunits were identified exclusively in the chronic pancreatitis specimens; however, there is currently no other evidence that these proteins have a role in the development or progression of chronic pancreatitis. Following orthogonal validation, the proteins described above maybe potential diagnostic biomarkers of their respective diseases, as well as targets for directed investigations into disease pathogenesis and progression. Further biological and biochemical studies (e.g., immunohistochemistry using larger cohorts), must be performed to analyze further these selected proteins.
A comparison of frozen verses FFPE tissue would reveal further insight into the utility of FFPE specimens in pancreatic research. However, standardized conditions for frozen tissue are not well established. Such conditions include the initial freezing state (e.g., flash-freezing in liquid nitrogen or dry ice) or procedures for long-term storage (e.g., storage in liquid nitrogen or -80°C). In contrast, FFPE specimens are typically processed with standardized methodologies and are inherently stable at room temperature or below. Studies have also indicated that fresh-frozen tissue do not properly maintain cellular morphology [33, 34]. Moreover, recent studies of follicular lymphoma [11], renal carcinoma [24], ear canal [14], breast cancer [35], and liver [15], have identified similar numbers of proteins using either FFPE tissue or frozen tissue. However, no such comparison has been performed using pancreatic tissue. A systematic study of a statistically significant number of FFPE and frozen pancreatic tissue may provide further evidence as to the benefits of one method over the other for mass spectrometry-based proteomic analyses.
Diagnostic specificity and relatively standardized specimen preservation renders FFPE tissue analysis superior to other organ-specific biomarker discovery strategies that typically analyze body fluids, such as blood derivatives, urine, or proximal fluids [36, 37, 38, 39]. As such, recent efforts have attempted to further standardize collection, handling, and storage of various body fluid specimens [36, 37, 40, 41, 42, 43, 44, 45, 46]. Nevertheless, meaningful inter-laboratory data comparisons have historically been limited due to differences in specimen handling. Moreover, the availability of vast archives of patient samples with clearly defined clinical histories, diagnoses, and outcomes enhances the robustness and utility of FFPE-based investigations. The value of tissuebased analysis is not limited to biomarker discovery; thorough analysis may also identify therapeutic targets and improve understanding of the molecular basis of pathogenesis, pathophysiology and clinical course. In addition, miRNA and/or mRNA studies can also be performed on FFPE tissue [47, 48, 49, 50]. Data from these studies can be compared to proteomics-based FFPE analysis, providing insight into organ- or diseasespecific translational regulation. However, to achieve the maximum analytical depth, more efficient protein (or peptide) extraction protocols must be developed and potential specimen preparation artifacts, such as amino acid residue modifications, must be reduced or eliminated.
The identification of a greater number of proteins than presented herein would be possible by overcoming procedural limitations. For example, harsh FFPE tissue preparation conditions can limit protein identification. More specifically, irreversible formalin-induced intra- and intermolecular crosslinking in FFPE specimens often hinders the solubility of proteins, complicating the extraction of these proteins and, potentially, larger peptides [51]. During tissue fixation, formalin adds a methylene hydrate group to the side chain of certain amino acids resulting in a crosslinking methylene bridge (both inter- and intra-peptide) which will likely prevent peptide identification [52, 53]. Moreover, chemical modifications of side chain moieties of lysyl, arginyl, tyrosyl, histidyl, and seryl are common during FFPE preparation [33], and further limit protein identifications. In addition, in nucleic acid extraction from FFPE tissue, extensive periods of fixation significantly reduces RNA extraction [54] and typically results in DNA fragmentation [55], and by extension, such effects may also be prevalent in proteins. As FFPE sections generally consist of different cell types, sample heterogeneity may be an issue. If a more homogeneous sample is needed, laser-capture microdissection (LCM) and serial sectioning may be implemented for such analyses [25, 56, 57]. Cellular microdissection decreases sample complexity thereby increasing analytical depth. Improvements in sample fixation and analysis may overcome these obstacles, and greatly increase the depth of the proteomic analysis of wellpreserved FFPE specimens. In addition, future MSbased studies will achieve greater depth of quantitative proteomic analysis by exploiting the higher resolution, high mass accuracy and higher scanning speeds possible with emerging mass spectrometry platforms, such as the Orbitrap Elite [58] and the Q-Exactive [59] (Thermo Scientific, Waltham, MA, USA).
CONCLUSION
We have shown that differentially-expressed proteins can be identified among FFPE tissues specimens originating from individuals with autoimmune pancreatitis, chronic pancreatitis, and pancreatic cancer. With improvements in experimental methods, LC-MS/MS-based proteomic analysis of FFPE pancreatic tissue specimens may provide novel therapeutic targets and/or a means of high-throughput validation of current diagnostic biomarkers. With further investigation, this knowledge may result in methods enabling the discrimination between autoimmune pancreatitis and pancreatic cancer, which represents an unmet medical need. Given the plethora of FFPE specimen archives, large databases of disease-specific proteins may be assembled for validation via orthogonal methods, such as immunohistochemistry studies. The methodology described herein, in addition to the proteins which we have identified as differentially expressed, may offer a scaffold upon which to build further FFPE-based studies of pancreatic diseases. The work which we present demonstrates the potential of using LCMS/ MS for the analysis of archived FFPE pancreatic tissue, particularly to differentiate autoimmune pancreatitis and pancreatic cancer, and provides a basis upon which biomarker studies can be developed further.
Acknowledgments
Funds were provided by the following NIH grants: 1 F32 DK085835-01A1 (J.A.P.), 1 R21 DK081703-01A2 (D.L.C.) and 5 P30 DK034854-24 (Harvard Digestive Diseases Center; D.L.C.). In addition, we would like to thank the Burrill family for their generous support through the Burrill Research Grant. We would also like to thank members of the Steen Lab at Children’s Hospital Boston, MA, USA, in particular John FK Sauld and Ali Ghoulidi, as well as Linda S Lee from the Center for Pancreatic Disease at Brigham and Women’s Hospital, Boston, MA, USA for their assistance.
Conflict of interest
The authors declare no competing interests
References
- NIH, Opportunities and Challenges in Digestive DiseasesResearch: Recommendations of the National Commission onDigestive Diseases, U.S. Department of Health and HumanServices, National Institutes of Health, NIH publ. no. 08-6514(2009) 159-167.
- I. Nishimori, A. Tamakoshi, M. Otsuki, Prevalence ofautoimmune pancreatitis in Japan from a nationwide survey in2002, J Gastroenterol, 42 Suppl 18 (2007) 6-8.
- R.K. Pearson, D.S. Longnecker, S.T. Chari, T.C. Smyrk, K.Okazaki, L. Frulloni, G. Cavallini, Controversies in clinicalpancreatology: autoimmune pancreatitis: does it exist?, Pancreas,27 (2003) 1-13.
- I. Nishimori, A. Tamakoshi, S. Kawa, S. Tanaka, K. Takeuchi, T.Kamisawa, H. Saisho, K. Hirano, K. Okamura, N. Yanagawa, M.Otsuki, Influence of steroid therapy on the course of diabetesmellitus in patients with autoimmune pancreatitis: findings froma nationwide survey in Japan, Pancreas, 32 (2006) 244-248.
- D.L. Finkelberg, D. Sahani, V. Deshpande, W.R. Brugge,Autoimmune pancreatitis, The New England journal of medicine,355 (2006) 2670-2676.
- R. Pannala, S.T. Chari, Autoimmune pancreatitis, Curr OpinGastroenterol, 24 (2008) 591-596.
- R. Law, M. Bronner, D. Vogt, T. Stevens, Autoimmunepancreatitis: a mimic of pancreatic cancer, Cleveland Clinicjournal of medicine, 76 (2009) 607-615.
- J.A. Paulo, L.S. Lee, P.A. Banks, H. Steen, D.L. Conwell,Proteomic analysis of formalin-fixed paraffin-embeddedpancreatic tissue using liquid chromatography tandem massspectrometry, Pancreas, 41 (2012) 175-185.
- S.R. Shi, R.J. Cote, C.R. Taylor, Antigen retrieval techniques:current perspectives, J Histochem Cytochem, 49 (2001) 931-937.
- H. Steen, M. Mann, The ABC's (and XYZ's) of peptidesequencing, Nature reviews, 5 (2004) 699-711.
- B.A. Reimel, S. Pan, D.H. May, S.A. Shaffer, D.R. Goodlett, M.W.McIntosh, L.M. Yerian, M.P. Bronner, R. Chen, T.A. Brentnall,Proteomics on Fixed Tissue Specimens - A Review, CurrProteomics, 6 (2009) 63-69.
- B.M. Balgley, T. Guo, K. Zhao, X. Fang, F.A. Tavassoli, C.S. Lee,Evaluation of archival time on shotgun proteomics of formalinfixedand paraffin-embedded tissues, Journal of proteomeresearch, 8 (2009) 917-925.
- X. Jiang, S. Feng, R. Tian, M. Ye, H. Zou, Development ofefficient protein extraction methods for shotgun proteomeanalysis of formalin-fixed tissues, Journal of proteome research,6 (2007) 1038-1047.
- D.E. Palmer-Toy, B. Krastins, D.A. Sarracino, J.B. Nadol, Jr.,S.N. Merchant, Efficient method for the proteomic analysis offixed and embedded tissues, Journal of proteome research, 4(2005) 2404-2411.
- H. Xu, L. Yang, W. Wang, S.R. Shi, C. Liu, Y. Liu, X. Fang, C.R.Taylor, C.S. Lee, B.M. Balgley, Antigen retrieval for proteomiccharacterization of formalin-fixed and paraffin-embeddedtissues, Journal of proteome research, 7 (2008) 1098-1108.
- D. Kessner, M. Chambers, R. Burke, D. Agus, P. Mallick,ProteoWizard: open source software for rapid proteomics toolsdevelopment, Bioinformatics, 24 (2008) 2534-2536.
- I.V. Shilov, S.L. Seymour, A.A. Patel, A. Loboda, W.H. Tang, S.P.Keating, C.L. Hunter, L.M. Nuwaysir, D.A. Schaeffer, The ParagonAlgorithm, a next generation search engine that uses sequencetemperature values and feature probabilities to identify peptidesfrom tandem mass spectra, Mol Cell Proteomics, 6 (2007) 1638-1655.
- M.Q. Dong, J.D. Venable, N. Au, T. Xu, S.K. Park, D. Cociorva,J.R. Johnson, A. Dillin, J.R. Yates, 3rd, Quantitative massspectrometry identifies insulin signaling targets in C. elegans,Science, 317 (2007) 660-663.
- H. Liu, R.G. Sadygov, J.R. Yates, 3rd, A model for randomsampling and estimation of relative protein abundance inshotgun proteomics, Anal Chem, 76 (2004) 4193-4201.
- W. Cheung, M.M. Darfler, H. Alvarez, B.L. Hood, T.P. Conrads,N. Habbe, D.B. Krizman, J. Mollenhauer, G. Feldmann, A. Maitra,Application of a global proteomic approach to archival precursorlesions: deleted in malignant brain tumors 1 and tissuetransglutaminase 2 are upregulated in pancreatic cancerprecursors, Pancreatology : official journal of the InternationalAssociation of Pancreatology, 8 (2008) 608-616.
- B.L. Hood, M.M. Darfler, T.G. Guiel, B. Furusato, D.A. Lucas,B.R. Ringeisen, I.A. Sesterhenn, T.P. Conrads, T.D. Veenstra, D.B.Krizman, Proteomic analysis of formalin-fixed prostate cancertissue, Mol Cell Proteomics, 4 (2005) 1741-1753.
- P. Ostasiewicz, D.F. Zielinska, M. Mann, J.R. Wisniewski,Proteome, Phosphoproteome, and N-Glycoproteome AreQuantitatively Preserved in Formalin-Fixed Paraffin-EmbeddedTissue and Analyzable by High-Resolution Mass Spectrometry, JProteome Res, (2010).
- T. Guo, W. Wang, P.A. Rudnick, T. Song, J. Li, Z. Zhuang, R.J.Weil, D.L. DeVoe, C.S. Lee, B.M. Balgley, Proteome analysis ofmicrodissected formalin-fixed and paraffin-embedded tissuespecimens, J Histochem Cytochem, 55 (2007) 763-772.
- S.R. Shi, C. Liu, B.M. Balgley, C. Lee, C.R. Taylor, Proteinextraction from formalin-fixed, paraffin-embedded tissuesections: quality evaluation by mass spectrometry, J HistochemCytochem, 54 (2006) 739-743.
- L.F. Waanders, K. Chwalek, M. Monetti, C. Kumar, E. Lammert,M. Mann, Quantitative proteomic analysis of single pancreaticislets, Proceedings of the National Academy of Sciences of theUnited States of America, 106 (2009) 18902-18907.
- D.K. Crockett, Z. Lin, C.P. Vaughn, M.S. Lim, K.S. Elenitoba-Johnson, Identification of proteins from formalin-fixed paraffinembeddedcells by LC-MS/MS, Lab Invest, 85 (2005) 1405-1415.
- G.M. Cavestro, L. Frulloni, T.M. Neri, P. Seghini, A. Nouvenne,A. Zanetti, P. Bovo, F. Di Mario, L. Okolicsanyi, G. Cavallini,Association of HLA-DRB1*0401 allele with chronic pancreatitis,Pancreas, 26 (2003) 388-391.
- T.L. Freitag, C. Cham, H.H. Sung, G.F. Beilhack, I. Durinovic-Bello, S.D. Patel, R.T. Bronson, D. Schuppan, G. Sonderstrup,Human risk allele HLA-DRB1*0405 predisposes class IItransgenic Ab0 NOD mice to autoimmune pancreatitis,Gastroenterology, 139 (2010) 281-291.
- X. Li, R. Ni, J. Chen, Z. Liu, M. Xiao, F. Jiang, C. Lu, The presenceof IGHG1 in human pancreatic carcinomas is associated withimmune evasion mechanisms, Pancreas, 40 (2011) 753-761.
- T. Yoshida, N. Shiraki, H. Baba, M. Goto, S. Fujiwara, K. Kume,S. Kume, Expression patterns of epiplakin1 in pancreas,pancreatic cancer and regenerating pancreas, Genes Cells, 13(2008) 667-678.
- E. Levi, D.S. Klimstra, A. Andea, O. Basturk, N.V. Adsay, MUC1and MUC2 in pancreatic neoplasia, J Clin Pathol, 57 (2004) 456-462.
- Z. Zhao, H. Liu, X. Wang, Z. Li, Separation and identification ofHSP-associated protein complexes from pancreatic cancer celllines using 2D CN/SDS-PAGE coupled with mass spectrometry, JBiomed Biotechnol, 2011 (2011) 193052.
- C.H. Fox, F.B. Johnson, J. Whiting, P.P. Roller, Formaldehydefixation, J Histochem Cytochem, 33 (1985) 845-853.
- R.J. McKenna, Jr., W.V. Houck, New approaches to theminimally invasive treatment of lung cancer, Curr Opin PulmMed, 11 (2005) 282-286.
- K.F. Becker, C. Schott, S. Hipp, V. Metzger, P. Porschewski, R.Beck, J. Nährig, I. Becker, H. Höfler, Quantitative protein analysisfrom formalin-fixed tissues: implications for translational clinicalresearch and nanoscale molecular diagnosis, The Journal ofPathology, 211 (2007) 370-378.
- V. Thongboonkerd, Proteomics of human body fluids :principles, methods, and applications, Humana Press, Totowa,N.J., 2007.
- S. Decramer, A. Gonzalez de Peredo, B. Breuil, H. Mischak, B.Monsarrat, J.L. Bascands, J.P. Schanstra, Urine in clinicalproteomics, Mol Cell Proteomics, 7 (2008) 1850-1862.
- D.M. Good, V. Thongboonkerd, J. Novak, J.L. Bascands, J.P.Schanstra, J.J. Coon, A. Dominiczak, H. Mischak, Body fluidproteomics for biomarker discovery: lessons from the past holdthe key to success in the future, J Proteome Res, 6 (2007) 4549-4555.
- Y.K. Paik, H. Kim, E.Y. Lee, M.S. Kwon, S.Y. Cho, Overview andintroduction to clinical proteomics, Methods Mol Biol, 428(2008) 1-31.
- J. Barratt, P. Topham, Urine proteomics: the present andfuture of measuring urinary protein components in disease,Cmaj, 177 (2007) 361-368.
- G.L. Hortin, D. Sviridov, Diagnostic potential for urinaryproteomics, Pharmacogenomics, 8 (2007) 237-255.
- H. Muller, H. Brenner, Urine markers as possible tools forprostate cancer screening: review of performance characteristicsand practicality, Clinical chemistry, 52 (2006) 562-573.
- N.P. Munro, D.A. Cairns, P. Clarke, M. Rogers, A.J. Stanley, J.H.Barrett, P. Harnden, D. Thompson, I. Eardley, R.E. Banks, M.A.Knowles, Urinary biomarker profiling in transitional cellcarcinoma, International journal of cancer, 119 (2006) 2642-2650.
- V. Thongboonkerd, Urinary proteomics: towards biomarkerdiscovery, diagnostics and prognostics, Molecular bioSystems, 4(2008) 810-815.
- J.A. Paulo, L.S. Lee, B. Wu, K. Repas, P.A. Banks, H. Steen, D.Conwell, Cytokine protein microarray analysis of pancreatic fluidin tandem with the endoscopic pancreatic function test (ePFT),Pancreatology, Submitted (2010).
- H. Tammen, Specimen collection and handling:standardization of blood sample collection, Methods Mol Biol,428 (2008) 35-42.
- L. Nonn, A. Vaishnav, L. Gallagher, P.H. Gann, mRNA andmicro-RNA expression analysis in laser-capture microdissectedprostate biopsies: valuable tool for risk assessment andprevention trials, Exp Mol Pathol, 88 (2010) 45-51.
- N. Ikenaga, K. Ohuchida, K. Mizumoto, J. Yu, H. Fujita, K.Nakata, J. Ueda, N. Sato, E. Nagai, M. Tanaka, S100A4 mRNA is adiagnostic and prognostic marker in pancreatic carcinoma, JGastrointest Surg, 13 (2009) 1852-1858.
- A. Liu, M.T. Tetzlaff, P. Vanbelle, D. Elder, M. Feldman, J.W.Tobias, A.R. Sepulveda, X. Xu, MicroRNA expression profilingoutperforms mRNA expression profiling in formalin-fixedparaffin-embedded tissues, Int J Clin Exp Pathol, 2 (2009) 519-527.
- L.M. Gjerdrum, H.N. Abrahamsen, B. Villegas, B.S. Sorensen,H. Schmidt, S.J. Hamilton-Dutoit, The influence ofimmunohistochemistry on mRNA recovery from microdissectedfrozen and formalin-fixed, paraffin-embedded sections, DiagnMol Pathol, 13 (2004) 224-233.
- M. Ahram, M.J. Flaig, J.W. Gillespie, P.H. Duray, W.M. Linehan,D.K. Ornstein, S. Niu, Y. Zhao, E.F. Petricoin, 3rd, M.R. Emmert-Buck, Evaluation of ethanol-fixed, paraffin-embedded tissues forproteomic applications, Proteomics, 3 (2003) 413-421.
- V.K. Rait, L. Xu, T.J. O'Leary, J.T. Mason, Modeling formalinfixation and antigen retrieval with bovine pancreatic RNase A II.Interrelationship of cross-linking, immunoreactivity, and heattreatment, Lab Invest, 84 (2004) 300-306.
- V.K. Rait, T.J. O'Leary, J.T. Mason, Modeling formalin fixationand antigen retrieval with bovine pancreatic ribonuclease A: Istructuraland functional alterations, Lab Invest, 84 (2004) 292-299.
- M. Benchekroun, J. DeGraw, J. Gao, L. Sun, K. vonBoguslawsky, A. Leminen, L.C. Andersson, M. Heiskala, Impact offixative on recovery of mRNA from paraffin-embedded tissue,Diagn Mol Pathol, 13 (2004) 116-125.
- R.L. Romero, A.C. Juston, J. Ballantyne, B.E. Henry, Theapplicability of formalin-fixed and formalin fixed paraffinembedded tissues in forensic DNA analysis, J Forensic Sci, 42(1997) 708-714.
- M.R. Emmert-Buck, R.F. Bonner, P.D. Smith, R.F. Chuaqui, Z.Zhuang, S.R. Goldstein, R.A. Weiss, L.A. Liotta, Laser capturemicrodissection, Science (New York, N.Y, 274 (1996) 998-1001.
- V. Patel, B.L. Hood, A.A. Molinolo, N.H. Lee, T.P. Conrads, J.C.Braisted, D.B. Krizman, T.D. Veenstra, J.S. Gutkind, Proteomicanalysis of laser-captured paraffin-embedded tissues: amolecular portrait of head and neck cancer progression, ClinCancer Res, 14 (2008) 1002-1014.
- A. Michalski, E. Damoc, O. Lange, E. Denisov, D. Nolting, M.Muller, R. Viner, J. Schwartz, P. Remes, M. Belford, J.J. Dunyach, J.Cox, S. Horning, M. Mann, A. Makarov, Ultra High ResolutionLinear Ion Trap Orbitrap Mass Spectrometer (Orbitrap Elite)Facilitates Top Down LC MS/MS and Versatile PeptideFragmentation Modes, Mol Cell Proteomics, 11 (2012) O111013698.
- A. Michalski, E. Damoc, J.P. Hauschild, O. Lange, A. Wieghaus,A. Makarov, N. Nagaraj, J. Cox, M. Mann, S. Horning, Massspectrometry-based proteomics using Q Exactive, a highperformancebenchtop quadrupole Orbitrap mass spectrometer,Mol Cell Proteomics, 10 (2011) M111 011015.

