Namita Jain1*, Jaya Chaudhary1, Sapna Yadav1 and Nikhil Bansal2
1Department of Obstetrics and Gynaecology, Mahatma Gandhi Medical College, Rajasthan, India
2Department of Interventional Radiology, Mahatma Gandhi Medical College, Rajasthan, India
Corresponding Author:
Namita Jain
Assistant Professor, Department of Obstetrics and Gynaecology
Mahatma Gandhi Medical College, Rajasthan, India
Tel: 0141 277 1777
E-mail: namita.hardonian@gmail.com
Received date: Feb 18, 2019; Accepted date: March 04, 2019; Published date: March 07, 2019
Citation: Jain N, Chaudhary J, Yadav S, Bansal N (2019) A Rare Case of Acquired Uterine Arterio-Venous Malformation Misdiagnosed as Molar Pregnancy Managed Successfully with Uterine Artery Embolization. Gynecol Obstet Case Rep Vol.5: No.1: 71.
Keywords
Malformation; Bleeding; Embolization
Introduction
Uterine arterio-venous malformation (AVM) is encountered rarely in clinical practice as a cause of heavy menstrual bleeding. It can be congenital or acquired (secondary to any form of insult/injury) [1]. Women usually present with heavy or irregular bleeding (life-threatening sometimes) not responding to conventional management. Diagnosis is dependent on proper history taking and radiological imaging. Imaging used to diagnose uterine AVM can be pelvic ultrasound with Doppler, CT and MRI angiography [2].
Uterine AVM is characterized by negative β-hCG values and seen as multiple anechoic spaces in myometrium, with a typical spectral Doppler appearance of turbulent flow with low resistance and high velocity [3,4]. Initial step in the management is hemodynamic stabilization with intrauterine tamponade. Hysterectomy is the most definitive treatment, but with the emergence of minimally invasive procedures like uterine artery embolization which in addition spares the uterus for future fertility is currently chosen as a first line of management for such cases. Restoration of normal menstrual cycles and successful pregnancies have been noted after the procedure [5].
A considerable overlap exists between the presentation and its appearance with other conditions like sub-involution of the placental bed, retained products of conception (RPOC) and gestational trophoblastic disease [6]. It can co-exist with incomplete miscarriage and gestational trophoblastic disease. Here comes the importance of accurate diagnosis as the management of these pathologies is suction and evacuation (S&E) which is contra-indicated in uterine AVM. Various case reports have been described on AVM diagnosed following a molar pregnancy. Due to the lack of good quality radiological diagnostic assessment and clinical awareness, it could be mistaken as molar pregnancy.
Case Report
A 22-year-old woman presented with heavy bleeding during periods for last 2 years which increased further for last 2 months associated with heaviness in lower abdomen not responding to medical management (hormonal and nonhormonal). She conceived spontaneously 4 years back. At 2.5 months amenorrhea, USG suggested missed abortion. She underwent S&E, but she continued to bleed after the procedure. Repeat S&E was done. Ultrasounds done did not suggest any increased vascularity. She again conceived for the second time and aborted a well formed male baby at 5 months, following which she continued to bleed. Again a repeat D&C was done in view of RPOCs and 2 units of blood was transfused. Third time, she conceived with ovulation induction with clomiphene citrate 100 mg. At 5th week, an USG was done, suggestive of gestational sac corresponding to POG, but it was also suggestive of molar pregnancy (because of increased myometrial vascularity) with β-hCG of 14000. S&E was done and tissue sent for histopathological examination which was reported as products of conception. She was followed till her β-hCG came <5 IU/L. Her ultrasound reports were reviewed and color doppler was done. Each ultrasound report suggested increased myometrial vascularity with impression of uterine arterio-venous malformation (Figures 1-3).
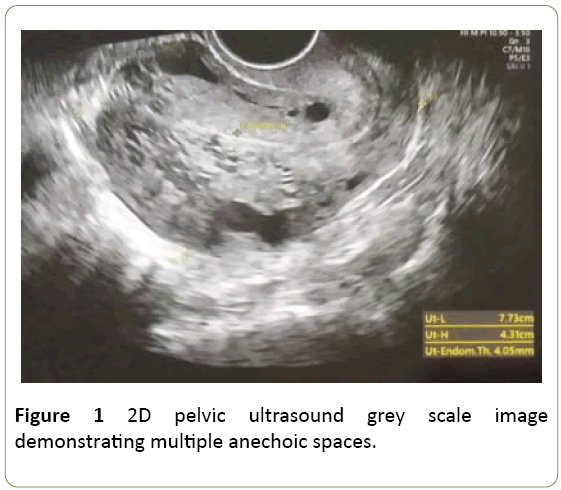
Figure 1: 2D pelvic ultrasound grey scale image demonstrating multiple anechoic spaces.
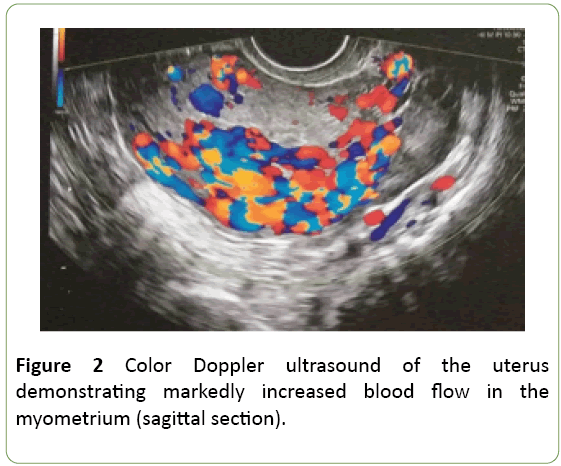
Figure 2: Color Doppler ultrasound of the uterus demonstrating markedly increased blood flow in the myometrium (sagittal section). Figure
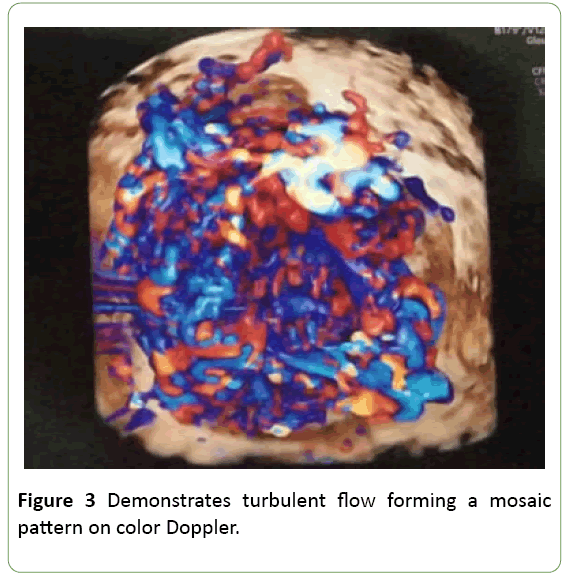
Figure 3: Demonstrates turbulent flow forming a mosaic pattern on color Doppler.
Bilateral uterine artery embolization was planned after informing all the pros and cons associated with the procedure with a written informed consent. Selective cannulation of both right and left uterine artery was done followed by obstructing them with polyvinyl alcohol particles mixed with gelfoam. Images are shown below before and after the embolization (Figures 4 and 5).
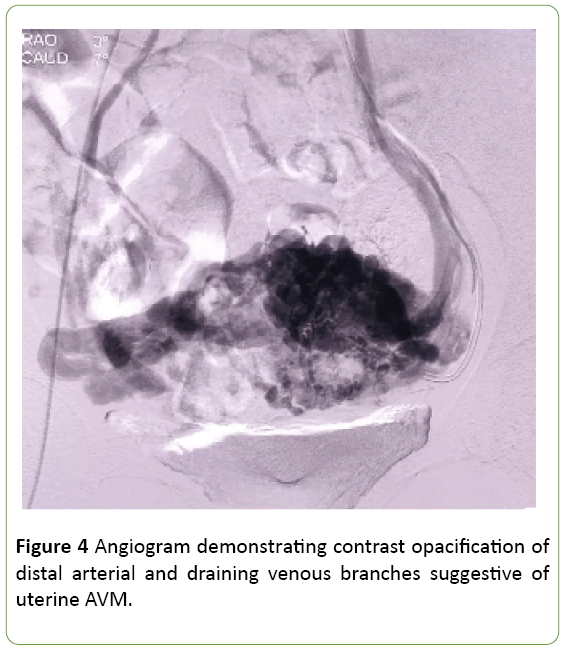
Figure 4: Angiogram demonstrating contrast opacification of distal arterial and draining venous branches suggestive of uterine AVM.
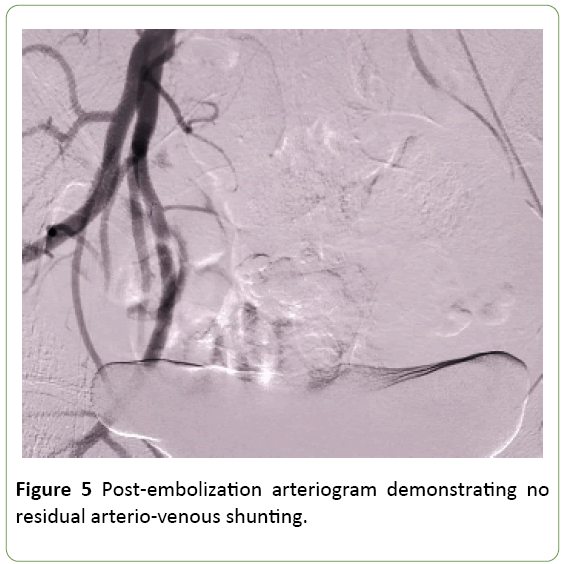
Figure 5: Post-embolization arteriogram demonstrating no residual arterio-venous shunting.
She was started on cyclical OCPs. Her symptoms along with her quality of life improved dramatically and the ultrasound depicted marked decrease in anechoic spaces with decreased vascularity after the procedure on her 3rd month follow-up.
Discussion
The incidence of uterine AVM is difficult to estimate as most of the cases go unnoticed. Fewer than 150 cases has been reported in the literature. History of uterine curettage followed by excessive bleeding in a reproductive age women in association with pulsatile uterus or pulsation palpable in the adnexa should raise the suspicion of uterine AVM. Acquired AVMs might arise due to embedding of venous tissue in the scar within the myometrium [5].
First case of uterine AVM was reported in 1926 [7]. Some argued that it is being overdiagnosed due to frequent use of USG. So the term uterine AVM is strictly used for lesion with hypervascular mass with early filling on angiography or on histopathological examination of uterus [6]. Uterine AVM is characterized by negative β-hcg values but when associated with early pregnancy, it can be confused with gestational trophoblastic disease. To differentiate, a good clinical acumen is needed. In our case, S&E was done at a private clinic confusing an AVM with molar pregnancy. Whenever in doubt, MRI angiography should be considered to differentiate the condition.
Management of uterine AVM depends upon the hemodynamic status of the women, age of the women, reproductive history and future reproductive plans and degree of bleeding. Once the diagnosis is confirmed, clinical condition of the patient is the main determinant in choosing the treatment option. The definitive treatment hysterectomy is undertaken only if no future fertility is desired and women refused to come for follow-up, or if she has not responded to UAE. The goal of embolization is to eradicate abnormal arteriovenous communication while maintaining uterine perfusion. It is a preferred treatment option as it is minimally invasive and fertility sparing. Variety of material are available to perform the embolization like PVA particles, gelfoam, tissue glue etc. but no difference in clinical outcome with respect to the embolic agent was found [8]. Complications like pelvic pain is quite common after the procedure which can be taken care of by simple analgesics. Serious complications include uterovaginal or rectovaginal fistulas, neurological deficits due to accidental embolization of internal iliac artery. But such complications are rarely encountered [9].
In our case, women had multiple abortions, pelvic pain and heavy bleeding during periods. She was desirous of future fertility and she was not responding to medical management. Post embolization she was relieved of her pelvic pain and her periods became normal. A success rate of around 92% has been reported in the literature. In a study by Yang 11 out of 14 women were successfully treated with uterine artery embolization. These 11 women had a return of normal menstrual cycle in 1-2 months and remained symptom-free during the follow-up period which ranged 1-10 years. Four of these women became pregnant 1-5 years later [4].
In a retrospective audit at Canberra Hospital, 27 women who were treated for uterine AVMs achieved 34 pregnancies and 31 live births. Reassuringly, none of these women experienced any complications such as severe growth restriction or adherent placenta (accreta) [10]. With increased availability and technological advancement, clinician will be dealing more with such cases in future. Clinical awareness is needed to diagnose and differentiate it from other pregnancy related conditions to allow appropriate management of the condition.
Conclusion
To conclude, uterine AVM diagnosis is rarely encountered as a cause of abnormal uterine bleeding and can be misdiagnosed as GTD. Clinical awareness is mandatory before it can be accurately diagnosed. Due to the availability of UAE, hysterectomy is rarely required. Based on the available literature, UAE leads to restoration of normal periods and fertility without much increase in pregnancy complications. To further support this, more data is required.
Conflict of Interest
The authors have no Conflict of interest to report with this research.
References
- Annaiah TK, Sreenivasan SK (2015) Uterine arteriovenous malformations: clinical implications. The Obstetrician & Gynaecologist 17: 243-250.
- Timmerman D, Van den Bosch T, Peeraer K, Debriuwere E, Van Schoubroeck D, et al. (2000) Vascular malformations in the uterus: ultrasonographic diagnosis and conservative management. Eur J Obstet Gynecol Reprod Biol 92: 171-178.
- Polat P, Suna S, Kantarcy M, Alper F, Levent A (2002) Color doppler US in the evaluation of uterine vascular abnormalities. Radiographics 22: 47-53.
- Yang JJ, Xiang Y, Wan XR, Yang XY (2005) Diagnosis and management of uterine arteriovenous fistulas with massive vaginal bleeding. Int J Gynaecol Obstet 89: 114-119.
- Grivell RM, Reid KM, Mellor A (2005) Uterine arteriovenous malformations: a review of the current literature. Obstet Gynecol Surv 60: 761-767.
- Clarke MJ, Mitchell PJ (2003) Uterine arteriovenous malformation: a rare cause of uterine bleeding. Diagnosis and treatment. Australas Radiol 47: 302-305.
- Dubreuil G, Loubat E (1926) Aneurisme circoid de l’uterus. Ann Anat Pathol 3: 697-718.
- Ghai S, Rajan DK, Asch MR, Muradali D, Simons ME, et al. (2003) Efficacy of embolization in traumatic uterine vascular malformations. J Vasc Interv Radiol 14: 1401-1408.
- Kwon JH, Kim GS (2002) Obstetric iatrogenic arterial injuries of the uterus: diagnosis with US and treatment with transcatheter arterial embolization. Radiographics 22: 35-46.
- Eling R, Kent A, Robertson M (2012) Pregnancy after uterine arteriovenous malformation: case series and literature review. Australas J Ultrasound Med 15: 87-96.

