Keywords
Focal atrial tachycardia; Mixed connective tissue disease; Scleroderma; Systemic sclerosis; Systemic lupus erythematosus; Rheumatoid arthritis; Polymyositis; Arrhythmia
Introduction
Mixed Connective Tissue Disease (MCTD) was first described in 1972. It consist of mixed features of several autoimmune in origin connective tissue disorders such as Systemic Lupus Erythematosus (SLE), Systemic Sclerosis (SS), Polymyositis and Rheumatoid Arthritis (RA), in association with the presence of high titer of autoantibody to U1 ribonucleoprotein RNP [1]. The prevalence of cardiac involvement in MCTD was previously reported as 13% to 65%. The most frequently observed manifestations were pericarditis (30% to 43%), mitral valve prolapse (25% to 32%), while other manifestations include conduction disturbances and pulmonary hypertension [2]. To authors knowledge, there have been minimal case report on arrythmias related to cardiac manifestation of mixed connective tissue disease. Here, we describe a case of mixed connective tissue disease who presented with palpitation and was noted to have focal atrial tacycardia.
Case Report
A 44-years-old lady with a background history of mixed connective tissue disease (MCTD) diagnosed in 1992 with overlap syndrome of rheumatoid arthritis, systemic lupus erythematosus, and scleroderma fulfilling the proposed criteria of MCTD by Alarcon-Segovia and Kahn’s presented to our outpatient clinic for further management of arrhythmia. She has been managed by her rheumatologist prior to this since 1992 when she first presented with history of multiple joint pains and swelling, early morning stiffness lasting more than three hours, mouth ulcers, Raynaud’s phenomenon, digital vasculitis, early sclerodactyly, telengieactasia and puckering of angle of mouth. ENA antibody was positive, while anti ds DNA and RF were negative. She was in remission since 2012 and was on stable dose of 10 mg weekly methotrexate and T. prednisolone 5 mg daily.
She presented to her rheumatologist recently with palpitations and was thus referred to a private hospital. She was haemodynamically stable at that time, with a heart rate of 150 beats per minute, and was not in cardiac failure. On auscultation, her lungs were clear and cardiovascular examination was unremarkable. Electrocardiogram (ECG) showed regular narrow complex tachycardia (Figure 1) for which she was treated as supraventricular tachycardia and was given intravenous adenosine 6 mg bolus. Subsequent ECG showed atrial tachycardia with variable conduction (Figures 2 and 3). She was then given intravenous amiodarone infusion, and was discharged with T. bisoprolol, T. digoxin, and T. dabigatran with an outpatient referral to our centre for further management of atrial tachycardia. An echocardiogram done showed normal left ventricular size with good left ventricular systolic function; rheumatic mitral valve (anterior mitral valve leaflet had thickened tip and doming during diastole, with thickened, calcified, immobile posterior mitral valve leaflet) and mild to moderate mitral stenosis and mild mitral regurgitation. Other valves appeared normal.
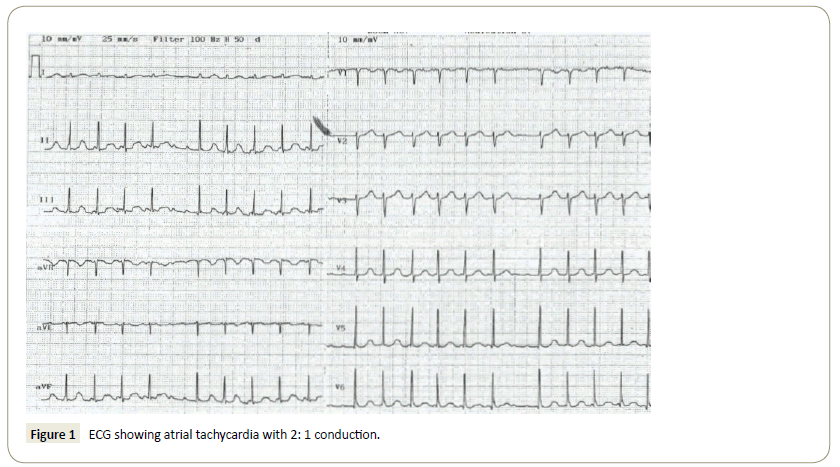
Figure 1: ECG showing atrial tachycardia with 2: 1 conduction.
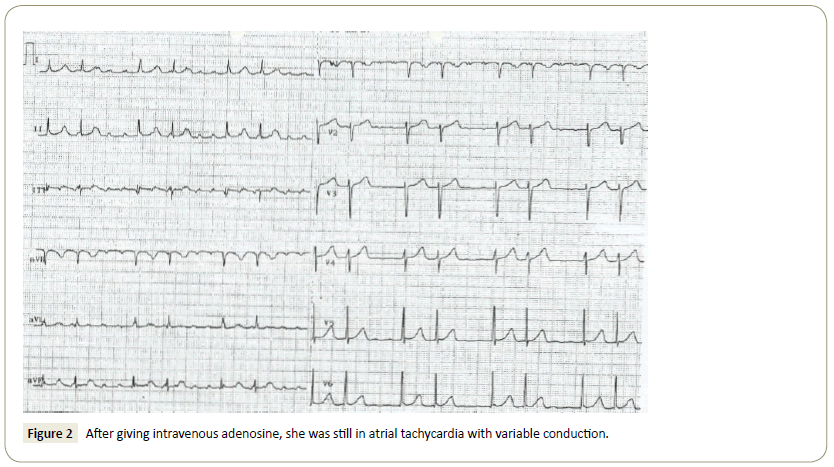
Figure 2: After giving intravenous adenosine, she was still in atrial tachycardia with variable conduction.
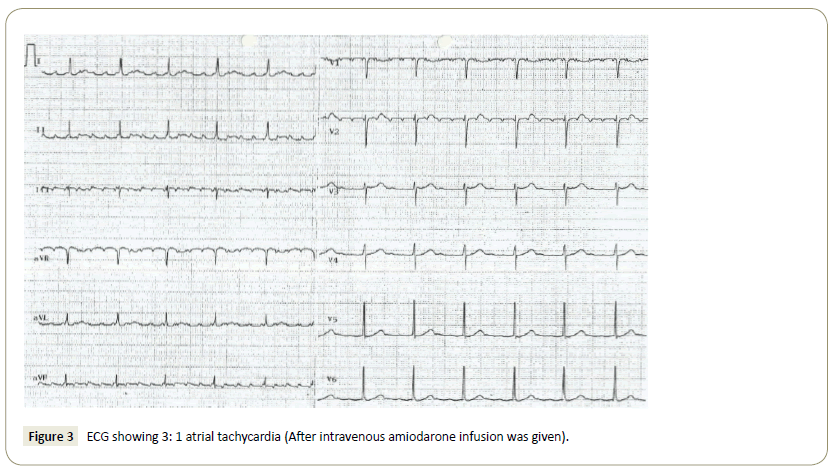
Figure 3: ECG showing 3: 1 atrial tachycardia (After intravenous amiodarone infusion was given).
Upon review in our clinic, she gives history of intermittent palpitation since the past one year but has never sought medical attention prior to this. Physical examination revealed a well, thin built middle aged lady with tightening of facial skin, microstomia and a beaklike face. There was presence of sclerodactyly with amputation of terminal phalanx of right middle finger. Systemic review was otherwise normal. Blood pressure was 110/70 mmHg, heart rate was 54 beats per minute, with regular rhythm. ECG during clinic review showed sinus rhythm (Figure 4). Treatment options of medical therapy versus ablation were discussed with the patient, and she opted for ablation.
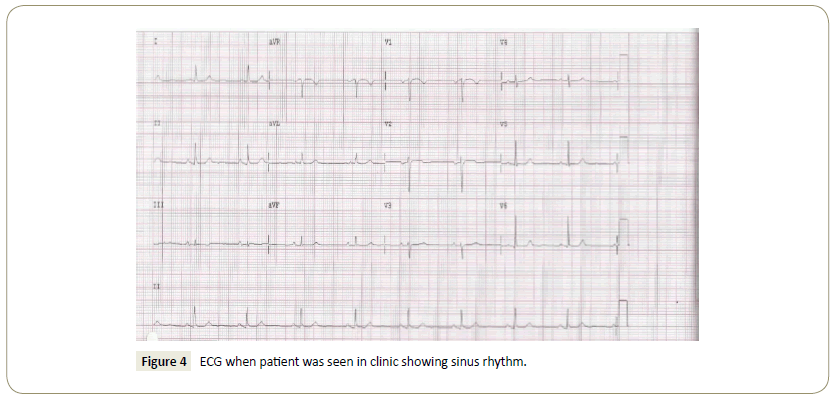
Figure 4: ECG when patient was seen in clinic showing sinus rhythm.
Atrial tachycardia ablation with 3D mapping using CARTOTM was done subsequently under sedation. The right femoral vein was cannulated and wires were introduced to the right atrium. A three dimensional mapping of the atria was done with activation suggestive of focal atrial tachycardia at postcrista to midcrista. Radiofrequency was thus delivered with immediate termination of atrial tachycardia. There was no further tachycardia induced post ablation. ECG post successful ablation is shown in Figure 5.
Figure 5: ECG post ablation showing sinus rhythm.
The patient was discharged well the next day. Previous medications (digoxin, bisoprolol, and pradaxa) was stopped and she was planned for review in two months’ time.
Discussion
Connective tissue diseases include Sjogren’s syndrome, rheumatoid arthritis, systemic lupus erythematosus, relapsing polychondritis, progressive systemic sclerosis, dermatomyositis and polymyositis, antiphospholipid syndrome, adult-onset Still’s disease and mixed connective tissue disorders. These diseases are acquired immunologically, and are mediated inflammatory disorders characterized by abnormal function or structure of one or more of the elements of the connective tissue, namely collagen, elastin or the mucopolysaccharides. It is characterized by production of autoantibody and other immune-mediated dysfunction [3].
Mixed connective tissue disease (MCTD) is an autoimmune condition that affects almost all major organs in the body, most commonly affecting females (80%) between ages of 4-80 years old [4]. There are four sets of criterias used in defining MCTD, namely the Sharp, Alarcon-Segovia, Kakusawa, and Kahn criteria. Upon reevaluation of these criteria by Amigues et al. it is concluded that the criteria that best define MCTD were those proposed by Alarcon-Segovia, with 62.5% sensitivity and 86.2% specificity, and this is comparable to Kahn’s criteria [5]. In MCTD, cardiac disease involvement has been reported to be as high as 65% [4]. Prevalence of symptomatic cardiac disease, in which common symptoms are chest pain, dyspnoea, and palpitation are reported to be ranging from 24% to 63% [1]. The most frequently observed cardiac manifestation; as stated earlier were pericarditis (30% to 43%) followed by mitral valve prolapse (25%-32%), conduction disturbances, abnormal left ventricular diastolic filling pattern, and pulmonary hypertension, which is associated with poor prognosis [1,6].
Subclinical cardiac involvement were detected using tests such as electrocardiogram (ECG), Holter monitor, and echocardiogram, which was detected to be present in 6% to 38% of patients [1]. In terms of evaluation of the coronary arteries, several methods are available, such as coronary magnetic resonance angiography. However, its use is reduced due to the limited temporal and spatial resolution, partial volume artefacts, reliance on multiple breath-holds, and poor visualisation of the entire coronary artery. Invasive coronary angiography is considered as the gold standard technique, however it is an invasive and expensive procedure, with some periprocedural morbidity and mortality. Other coronary imaging method that is commonly used that is relatively fast and simple is coronary computed tomography angiography (CTA) procedure [7].
In MCTD, the most common ECG abnormalities observed are conduction disturbances such as hemiblock, bundle branch block, and atrioventricular block. Using echocardiogram, 12% to 38% subclinical cardiac involvement were detected. The high prevalance of subclinical cardiac involvement emphasizes the subtlety of cardiac disease in MCTD [1].
The pathophysiology behind cardiac involvement in MCTD is not well understood. It however appears to resemble other connective tissue disorders. In two postmortem studies, it was concluded that myocarditis might be responsible for diastolic dysfunction and conduction abnormalities [1]. It was noted at autopsy of myositis patients that similar changes to those in the myocardium were noticed in the conducting system including lymphocytic infiltration, fibrosis of the sinoatrial node, and contraction band necrosis [6]. Pericardial effusion and pericarditis was hypothesized to be due to serositis that might be related to rheumatoid arthritis-like and lupus-like spectrum of MCTD [1]. Other contributing factors to impaired left ventricular function and arrythmias are vascular changes in the heart such as vasculitis, intima proliferation, media sclerosis and microvessel disease of the heart with vasospasm angina [6].
An article review on cardiac arrhythmias and conduction disturbances in autoimmune rheumatic diseases describes arrythmia prevalence in patients with rheumatoid arthritis (RA), systemic sclerosis (SS), and systemic lupus erythematosus (SLE) separately. In RA, coronary artery disease gives a major contribution to acute coronary syndrome and ventricular arrythmias. Rhythm disturbances were also contributed by accelerated coronary atherosclerosis, coronary vasculitis, superimposed coronary thrombosis, myocarditis, and pulmonary hypertension. In SLE, sinus tachycardia, atrial fibrillation, and atrial ectopic beats are most frequent. Supraventricular arrythmias are associated with transient episodes, and may be related to exacerbations of SLE or myocarditis, while sinus tachycardia occur in 50% of the population. Sinus bradycardia and prolonged QT interval have been described in patients with anti-small cytoplasmic ribonucleoproteins (anti-Ro/SSA) antibody. Malignant ventricular arrythmias are rarely reported. In SS, atrial and ventricular arrythmias are common, which may be asymptomatic. They present with transient atrial fibrillation, flutter, or paroxysmal supraventricular tachycardia (20%-30%). 67% patients with SS were demonstrated to have ventricular tachycardia, while 7%-13% with non-sustained ventricular tachycardia [8].
10% of supraventricular tachycardia are due to focal atrial tachycardia (AT). It may initiate other forms of atrial arrythmias such as atrial fibrillation (AF) and atrial flutter [9]. The prevalence of this type of tachycardia in asymptomatic subjects was reported as 0.34%, while in symptomatic patients 0.46%. Persistent form of focal AT may lead to tachycardia induced cardiomyopathy and subsequently congestive cardiac failure [10]. Focal AT is defined as activation of the atria from a discrete focus located at atrial myocardium area which is less than 2 cm in diameter, followed by a centrifugal spread. Common foci for focal AT are along the crista terminalis (CT), tricuspid annulus (TA), ostium of the coronary sinus (CS) and the parahissian region in the right atrium. In the left atrium, it is predominantly at the ostia of the pulmonary veins (PVs) and, less commonly, at the mitral annulus, LA appendage, and left-sided septum [9].
Focal AT has a variable clinical course. It can occur at any age, from birth to old age. Spontaneous remission is common, especially in childhood and adolescence. The focus may originate in the presence of structural heart disease, in which abnormal myocardium are seen with areas of myocardial fibrosis, myocyte hypertrophy, inflammatory infiltration, and fatty substitution. However, the majority histological analysis conducted from originating AT focus site of myocardium has shown normal findings [9]. In one large series, among 345 patients with focal AT who underwent radiofrequency ablation only 4% of patients (n=14) had preexisting structural heart disease [11]. In the case that we illustrate here, it is unclear whether any structural heart disease as a result of MCTD was present to cause focal AT, or whether focal AT was triggered by chronic rheumatic heart disease; or whether it occur as an isolated event in a normal myocardium. Myocardial biopsy to determine the structural heart disease is too invasive, while the alternative cardiac MRI had low sensitivity for diagnosis of myocarditis [2].
Conclusion
In conclusion, a case of focal AT itself is uncommon, and for it to occur in a patient with underlying mixed connective tissue disease and chronic rheumatic heart disease, who is likely to have structural heart disease is even more so. We were unable to conclude at this point whether the focal AT is caused by structural heart disease due to MCTD or chronic rheumatic heart disease, however, given the rarity of structural heart disease causing focal atrial tachycardia, and the possibility of linkage of focal AT with patient’s underlying disease is high, we believe this case is worth to be reported. Regardless of the underlying cause, management of focal AT is still via ablation. Although usually after a successful focal AT ablation a follow up is deemed unnecessary, in this patient’s case we are following her up to monitor for future arrythmias in view of her underlying medical condition.
References
- Ungprasert P, Wannarong T, Panichsillapakit T, Cheungpasitporn W, Thongprayoon C, et al. (2014) Cardiac involvement in mixed connective tissue disease. Int J Cardiol 171: 326-330.
- Shinkawa Y, Yagita M, Fujita M (2016) Myocarditis in mixed connective tissue disease: A case report. J Clin Case Rep 6: 1-679.
- Razek AA (2016) Imaging of connective tissue diseases of the head and neck. Neuroradiology J 29: 222-230.
- Mathew J Jr, Kim T, Nunu T, Jahanmir J (2016) Mixed connective tissue disease presenting as atrial fibrillation, fever, lymphadenopathy, and pericardial effusion. J Case Rep Images Med 2: 24-30.
- Farhey Y, Hess EV (1997) Mixed connective tissue disease. Arthritis Care Res 10: 333-342.
- Lundberg IE (2005) Cardiac involvement in autoimmune myositis and mixed connective tissue disease. Lupus 14: 708-712.
- Razek AA, Elrakhawy MM, Yossof MM, Nageb HM (2018) Inter-observer agreement of the Coronary Artery Disease Reporting and Data System (CAD-RADSTM) in patients with stable chest pain. Pol J Radiol 83: e151-159.
- Seferovi? PM, Risti? AD, Maksimovi? R, Simeunovi? DS, Risti? GG, et al. (2006) Cardiac arrhythmias and conduction disturbances in autoimmune rheumatic diseases. Rheumatology (Oxford) 45: 39-42.
- Rosso R, Kistler PM (2010) Focal atrial tachycardia. Heart96: 181-185.
- Higa S, Chen SA (2006) Focal atrial tachycardia. J Arrhythmia 22: 132-148.
- Ellenbogen EA (2014) Cardiac electrophysiology from cell to bedside. Atr tachycardia (6th Edn) 3: 48.

