Keywords
Chemotherapy, Adjuvant; Combined Modality
Therapy; Deoxycytidine Kinase; gemcitabine; Pancreatic
Neoplasms; Radiotherapy, Adjuvant; RRM1 protein, human;
S100A2 protein, human; SLC29A1 protein, human
Abbreviations
dCK: deoxycytidine kinase; EORTC: European
Organization of Research and Treatment of Cancer; ESPAC:
European Study Group for Pancreatic Cancer; hENT1: human
equilibrative nucleoside transporter 1; RRM1: ribonucleotide
reductase subunit 1; RTOG: Radiation Therapy Oncology Group
What We Know Before the 2011 American Society
of Clinical Oncology (ASCO) Annual Meeting?
Only 10-20% of patients have classically resectable
disease at the time of pancreatic cancer diagnosis.
Surgical resection remains the only curative modality
for pancreatic cancer. Nevertheless, the prognosis of
patients after complete resection is poor, with 3-year
disease-specific survival rate at 27% (95% confidence
interval (CI): 23-32%) and median survival of 15-19
months [1, 2, 3]. Therefore, judicious use of efficacious
adjuvant therapies is necessary to improve the survival
of resected pancreatic cancer patients. There is now
substantial high level evidence to support the use of
adjuvant chemotherapy in resected pancreatic cancer
[4, 5, 6, 7]. However, the role for adjuvant chemoradiotherapy
remains more controversial.
There are numerous randomized controlled trials that
support the use of adjuvant chemotherapy after
resection of pancreatic cancer [4, 5, 6,]. The European
Study Group for Pancreatic Cancer (ESPAC-1) trial
demonstrated a survival benefit for adjuvant
chemotherapy but not adjuvant chemoradiotherapy and
even a possible detrimental effect for adjuvant
chemoradiation [4]. The Charité Onkologie Clinical-
001 (CONKO-001) study randomized patients with
resected pancreatic cancer to gemcitabine for 6 months
or observation [5]. Adjuvant chemotherapy showed a
trend towards improved overall survival. The use of
gemcitabine versus 5-FU was further defined by the
ESPAC-3 trial, which demonstrated equivalent survival
for both treatments, but more favorable safety profile
with gemcitabine [6]. There was also a trend toward
improved survival in the gemcitabine arm in patients
with node positive disease or those with positive
resection margins [6]. To further support the role of
adjuvant chemotherapy, the Boeck et al. [7] metaanalysis
demonstrated adjuvant chemotherapy provided
a significant increase in median survival.
The role for adjuvant chemoradiation is less well
defined as there are conflicting results from trials.
Despite the controversy, the level of evidence is strong
enough to support the use of adjuvant chemoradiotherapy
in the management of resected pancreatic
cancer in the United States. However, in Europe it is
common practice for patients to receive adjuvant
chemotherapy alone. There are three randomized
controlled trials investigating the role of adjuvant chemoradiation in resected pancreatic cancer [4, 8, 9].
The Gastrointestinal Study Group (GITSG) study
showed a survival benefit in patients who received
bolus 5-FU with radiotherapy, but has been criticized
for a sample size of 43 patients [8]. The European
Organization of Research and Treatment of Cancer
(EORTC) trial did not demonstrate a survival
advantage for patients treated with adjuvant chemoradiation
compared to observation [9]. There was a
trend toward survival in the chemoradiotherapy arm
compared to observation in the subset of patients with
pancreatic ductal carcinoma [9]. Radiation therapy in
the EORTC trial was suboptimal as the dose was
inadequate (40 Gy) and the radiation was delivered
with a split course. The ESPAC-1 evaluated adjuvant
concurrent chemoradiation therapy (bolus 5-FU/splitcourse
radiation), chemotherapy alone (5-FU/
leucovorin), chemoradiation therapy followed by
chemotherapy, and observation [4]. The results
demonstrated that the chemotherapy-only arm had a
significant benefit over the observation arm in median
survival and the chemoradiation therapy arm showed
worse median survival compared to the observation
arm [4]. This study was criticized for a confusing 2x2
factorial design, possible selection bias and suboptimal
radiotherapy (split course/poor quality control). An
additional phase 3 trial, Radiation Therapy Oncology
Group (RTOG) 9704, showed a benefit of adding
gemcitabine to infusional 5-FU combined with
radiotherapy at the cost of more grade 4 hematological
toxicity [10].
Despite the lack of randomized controlled trials,
evidence supporting the role of adjuvant chemoradiotherapy
in resected pancreatic cancer, several
single institution and retrospective series demonstrate a
benefit for adjuvant chemoradiotherapy [11, 12, 13, 14]. The Johns Hopkins-Mayo Clinic Collaborative
Study demonstrated that adjuvant chemoradiation (5-
FU based chemo- and radio-therapy to 50.4 Gy)
following pancreaticoduodenectomy was associated
with improved survival compared to observation alone
in their two institutional trial of 1,092 patients [11].
Furthermore, a retrospective review of 472 patients at
the Mayo Clinic found a survival benefit for adjuvant
chemoradiation after R0 pancreaticoduodenectomy
[12]. Several Surveillance, Epidemiology and End
Results (SEER) analysis have also demonstrated
efficacy for radiation therapy in pancreatic cancer [13, 14].
There may be a role for chemoradiation in the
treatment of patients with R1 resections [15, 16]. A
meta-analysis by Stocken et al. demonstrated a 25%
significant reduction in the risk of death with
chemotherapy with no significant reduction in the risk
of death with adjuvant chemoradiation [15]. However,
their subgroup analyses demonstrated that chemoradiotherapy
was more effective than chemotherapy alone in
patients with positive resection margins [15]. Similarly,
the meta-analysis by Butturini et al. demonstrated a
possible benefit to chemoradiation in patients with
positive resection margins [16].
The optimal time to initiate adjuvant chemotherapy
after pancreatic cancer surgery is unknown. Adjuvant
chemotherapy or chemoradiotherapy has been started
from 2 to 10 weeks after surgery, with most trials
starting adjuvant therapy within 8 weeks [1, 2, 5]. Once
adjuvant chemotherapy has been initiated, predicting
the response of patients has been the subject of
intensive research. The calcium-binding protein
S100A2 has been validated in a retrospective cohort of
patients treated with pancreatectomy for pancreatic
cancer as an independent predictor of survival, with
high expression correlated with disease progression
and poor outcome [17, 18]. Additionally, with
gemcitabine-based chemotherapy being a mainstay of
therapy, markers of the efficacy of gemcitabine such as
expression of the human equilibrative nucleoside
transporter 1 (hENT1), deoxycytidine kinase (dCK)
and ribonucleotide reductase subunit1 (RRM1) proteins
have been tentatively identified in vitro and in vivo
[19].
Despite the use of adjuvant chemotherapy or adjuvant
chemoradiotherapy after surgical resection, survival
still remains poor. Future studies in pancreatic cancer
will help to further define the role of adjuvant
chemoradiotherapy, elucidate the most efficacious
chemotherapeutic and biologic agents, optimize dosing
and timing of chemotherapy/radiation therapy and
individualize treatment based on predicting response to
chemotherapy and radiation therapy.
What Did We Learn at ASCO 2011 Annual
Meeting?
Chemotherapy versus Chemoradiotherapy
Drudi et al. (Abstract #4042) [20] conducted a pooled
analysis of all randomized controlled trials from 1966-
2010 investigating the role of adjuvant treatments, including both adjuvant chemotherapy and adjuvant
chemoradiation, in resected pancreatic cancer patients.
The purpose of the analysis was to determine if
adjuvant treatment, adjuvant chemotherapy or adjuvant
chemoradiation confer a survival benefit at 5 years
compared with no adjuvant treatment. There were a
total of 2,410 pooled patients from 12 randomized
controlled trials; 1,337 patients were treated with
adjuvant treatment (1,008 with adjuvant chemotherapy
and 329 with adjuvant chemoradiation), and 1,073
received no adjuvant treatment. The authors
demonstrated significant 5 year survival benefit for
adjuvant treatment and adjuvant chemotherapy (odds
ratio equal to 0.62, P=0.001 and odds ratio equal to
0.63, P=0.021, respectively), but not for adjuvant
chemoradiation (odds ratio equal to 0.92, P=0.71). This
pooled analysis demonstrated that adjuvant chemotherapy
improves 5-year survival in resected pancreatic
cancer patients but not adjuvant chemoradiotherapy.
This study served to further strengthen the role of
adjuvant chemotherapy in the management of resected
pancreatic cancer. These results concur with the results
of previous meta-analyses demonstrating a survival
benefit for adjuvant chemotherapy [7, 15].
Cetuximab plus Gemcitabine
The addition of cetuximab to adjuvant gemcitabine was
investigated in an open label, multi-center, phase II
trial reported by Fensterer et al. (Abstract #4039) [21].
Patients underwent R0 or R1 resection for pancreatic
cancer, then were treated with adjuvant chemotherapy
consisting of 6 cycles of gemcitabine with weekly
cetuximab for 24 weeks. There were 76 patients
enrolled, and 73 patients received at least one dose of
cetuximab. Median age was 64 years; 22.4% had R1
resection and 69.1% had K-ras mutation. Median
disease free survival was 11.9 months, and the disease
free survival rate at 18 months was 33.5%, failing to
demonstrate superiority over 35% as hypothesized by
the authors. Median overall survival was 21.5 months
(95% CI: 16.9-28.2 months). Grade 3 or 4 toxicities
were neutropenia in 11% of patients, thrombocytopenia
in 8.2%, dermatologic in 6.9%, and allergic reaction in
6.9%. The authors conclude that the addition of
cetuximab to gemcitabine in the adjuvant treatment of
pancreatic cancer does not improve disease free
survival over the use of gemcitabine alone (Table 1).
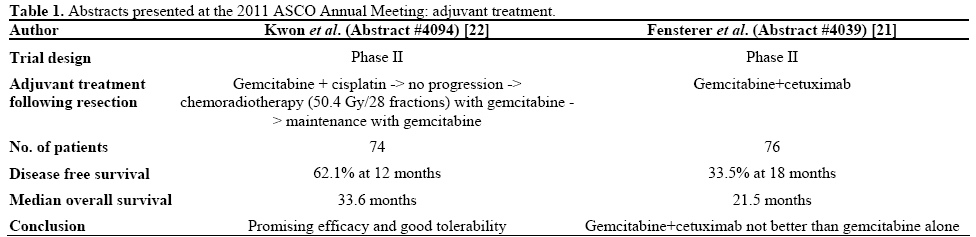
Gemcitabine, Cisplatin with Radiation
Kwon et al. (Abstract #4094) [22] conducted a phase II
trial of adjuvant gemcitabine and cisplatin chemotherapy
followed by chemoradiation with gemcitabine
and 5,040 cGy of radiation, then 4 cycles of
maintenance gemcitabine. There were 74 patients with
stage IB-IIB pancreas cancer who had undergone
resection enrolled between 2005 and 2009. The median
age was 61 year and the median follow-up was 45
months (range: 10.2-64.6 months). Of the patients
enrolled, 57 completed chemotherapy followed by
chemoradiation. One-year disease free survival (DFS) rate was 62.1%, median disease free survival was 17.4
months, and median overall survival was 33.6 months.
The majority of recurrences (66.2%) were distant
metastases. Increasing stage and involved lymph nodes
were associated with reduced disease free survival
(P<0.001 and P=0.01, respectively). Fifty-three of 74
patients (71.6%) had grade 3 or 4 hematologic toxicity,
with 4 patients experiencing febrile neutropenia. These
finding suggest promising efficacy with acceptable
toxicity for adjuvant multimodality therapy (Table 1).
Relationship Between Time to Adjuvant
Chemotherapy and Survival
Pisa et al. (Abstract #e14519) [23] evaluated a cohort
of 29 consecutive patients with resected nonmetastatic
pancreatic cancer who received adjuvant chemotherapy
with gemcitabine to attempt to identify a relationship
between time to adjuvant chemotherapy and survival
[7]. The median time to adjuvant chemotherapy was 47
days (range: 22-183 days), and the most common
reason for delay of adjuvant chemotherapy was postoperative
complications. No difference in age, gender,
stage or palliative chemotherapy used at progression
was identified between patients who started adjuvant
chemotherapy within 56 days (8 weeks) of surgery
versus those who started adjuvant chemotherapy after
56 days post-surgery. Median overall survival was 26.4
months in those who started adjuvant chemotherapy
within 56 days of surgery versus 14.8 months in those
who started adjuvant chemotherapy more than 56 days
after surgery (P=0.015). No significant difference was
seen in median progression free survival between the
groups. No patients died of toxicity or post-operative
complications. This underscores the need to keep time
to adjuvant chemotherapy under 8 weeks after surgery,
as has been the case in most clinical trials.
Prognostic Markers
S100A2 Expression as a Prognostic Marker
Tompero et al. (Abstract #4118) [24] performed a
secondary analysis of a subset of patients with head of
pancreas lesions treated adjuvantly on RTOG 9704 in
an attempt to validate S100A2 expression as a
prognostic marker in 150 specimens from patients
receiving adjuvant chemotherapy for pancreatic cancer.
Tissue microarray was used to quantify S100A2
expression, and patients were then stratified into four
groups based on the level of expression. For high vs.
no/low expression of S100A2, disease specific survival
was not significantly different at 1 or 2 years (P=0.09; Table 2). While S100A2 was not validated as a prognostic marker in this cohort of patients, the authors
recommend further study to try to resolve the
conflicting data about the role of S100A2 as a
prognostic biomarker.

hENT1, dCK, and RRM1
Marechal et al. (Abstract #4024) [25] conducted a
study using expression of hENT1, dCK, and RRM1 in
434 patients receiving adjuvant gemcitabine after
curative-intent resection of pancreatic cancer in an
attempt to associate expression of these proteins with
efficacy of gemcitabine. Among patients not treated
with gemcitabine-based chemotherapy, hENT1, dCK,
and RRM1 expression was not associated with overall
survival. In contrast, among the patients treated with
gemcitabine, hENT1 and dCK expression levels were
associated with changes in overall survival after
adjusting for tumor grade, size, lymph node
involvement and resection margin. In tumors with high
hENT1, gemcitabine was associated with better overall
survival (HR: 0.44; 95%CI: 0.28-0.69; P<0.001); in
tumors with high dCK, gemcitabine was associated
with better overall survival (HR: 0.57; 95% CI: 0.41-
0.78; P=0.001). In tumors with low hENT1or dCK
levels, gemcitabine was not associated with improved
overall survival. These findings suggest that expression
levels of hENT1 and dCK may predict response to
gemcitabine-based chemotherapy after curative-intent
surgery.
Conflict of interest
The authors have no potential
conflicts of interest
References
- Jemal A, Siegel R, Ward E, Hao Y, Xu J, Thun MJ. Cancer statistics, 2009. CA Cancer J Clin 2009; 59:225-49.
- Li D, Xie K, Wolff R, Abbruzzese JL. Pancreatic cancer. Lancet 2004; 363:1049-57.
- Saif MW. Controversies in the adjuvant treatment of pancreatic adenocarcinoma. JOP. J Pancreas (Online) 2007; 8:545-52.
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med. 2004 Mar 18;350(12):1200-10.
- Oettle H. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer. JAMA. 2007 Jan 17;297:267-277.
- Neoptolemos JP, Stocken DD, Bassi C, Ghaneh P, Cunningham D, Goldstein D, et al. Adjuvant chemotherapy with fluorouracil plus folinic acid vs gemcitabine following pancreatic cancer resection: a randomized controlled trial. JAMA. 2010 Sep 8;304(10):1073-81.
- Boeck S, Ankerst DP, Heinemann V. The role of adjuvant chemotherapy for patients with resected pancreatic cancer: systematic review of randomized controlled trials and meta-analysis. Oncology. 2007;72(5-6):314-21. Epub 2008 Jan 14.
- Kalser MH, et al. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg. 1985 Aug; 120(8):899-903.
- Klinkenbijl JH, et al. Adjuvant radiotherapy and 5-fluorouracil after curative resection of cancer of the pancreas and periampullary region: phase III trial of the EORTC gastrointestinal tract cancer cooperative group. Ann Surg 1999 Dec;230(6):776-82.
- Regine WF, Winter KA, Abrams RA, Safran H, Hoffman JP, Konski A, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA. 2008 Mar 5;299(9):1019-26. Erratum in: JAMA. 2008 Apr 23/30;299(16):1902.
- Hsu CC, Herman JM, Corsini MM, Winter JM, Callister MD, Haddock MG, et al. Adjuvant chemoradiation for pancreatic adenocarcinoma: the Johns Hopkins Hospital-Mayo Clinic collaborative study. Ann Surg Oncol. 2010 Apr;17(4):981-90. Epub2010 Jan 20.
- Corsini MM, Miller RC, Haddock MG, Donohue JH, Farnell MB, Nagorney DM, et al. Adjuvant radiotherapy and chemotherapy for pancreatic carcinoma: the Mayo Clinic experience (1975-2005). J Clin Oncol. 2008 Jul 20;26(21):3511-6.
- Hazard L, Tward JD, Szabo A, Shrieve DC. Radiation therapy is
associated with improved survival in patients with pancreatic adenocarcinoma: results of a study from the Surveillance, Epidemiology, and End Results (SEER) registry data. Cancer. 2007 Nov 15;110(10):2191-201.
- Artinyan A, Hellan M, Mojica-Manosa P, Chen YJ, Pezner R, Ellenhorn JD, Kim J. Improved survival with adjuvant external-beam radiation therapy in lymph node-negative pancreatic cancer: a United States population-based assessment. Cancer. 2008 Jan 1;112(1):34-42.
- Stocken DD, Büchler MW, Dervenis C, Bassi C, Jeekel H, Klinkenbijl JH, et al. Meta-analysis of randomised adjuvant therapy trials for pancreatic cancer. Br. J Cancer. 2005 Apr 25;92(8):1372- 81.
- Butturini G, Stocken DD, Wente MN, Jeekel H, Klinkenbijl JH, Bakkevold KE, et al. Influence of resection margins and treatment on survival in patients with pancreatic cancer: meta-analysis of randomized controlled trials. Arch Surg. 2008 Jan;143(1):75-83; discussion 83.
- Biankin et al. Expression of S100A2 calcium-binding protein predicts response to pancreatectomy for pancreatic cancer. Gastroenterology. 2009 Aug;137(2):558-68, 568.e1-11
- Ohuchida K et al. Over-expression of S100A2 in pancreatic cancer correlates with progression and poor prognosis. J Pathol. 2007 Nov;213(3):275-82.
- Fujita H et al. Gene expression levels as predictive markers of outcome in pancreatic cancer after gemcitabine-based adjuvant chemotherapy. Neoplasia. 2010 Oct;12(10):807-17.
- Drudi F. Adjuavnt treatments in pancreatic cancer: Preliminary data of a pooled analysis. J Clin Onclol 2011; 29(Suppl.):4042
- Fensterer H et al. Multicenter phase II trial to investigate safety and efficacy of an adjuvant therapy with gemcitabine and cetuximab in patients with R0 or R1 resected pancreatic cancer. J Clin Onclol 2011; 29(Suppl.):4039.
- Kwon JH et al. Phase II trial of postoperative adjuvant gemcitabine and cisplatin chemotherapy followed by chemoradiation with gemcitabine in patients with resected pancreatic cancer. J Clin Onclol 2011; 29(Suppl.):4094.
- Pisa A, et al. The effect of time to adjuvant chemotherapy on survival in nonmetastatic resectable pancreatic adenocarcinoma: A retrospective analysis. J Clin Onclol 2011; 29(Suppl.):e14519.
- Tempero MA, et al. S100A2 as a prognostic marker in patients receiving adjuvant therapy for pancreatic cancer (PC): A secondary analysis of RTOG 9704. J Clin Onclol 2011; 29(Suppl.):4118.
- Maréchal R et al. Prediction of gemcitabine benefit after curative-intent resection of pancreatic adenocarcinoma using HENT1 and dCK protein expression. J Clin Onclol 2011; 29(Suppl.):4024.

