Keywords
Adult attachment; Abuse history; Relationship trauma; High-risk; Psychopathology; Personality disorders
Introduction
Considerable research has addressed relationship trauma and psychopathology within an attachment theory approach. In Attachment Theory, Bowlby [1-3] proposed that early child-parent attachment has life-long implications for an adult’s representational structure of relationships, personality development, and potential psychopathology. In this theory, a consistent and sensitive caregiving environment leads to thoughts and feelings that the world is a safe place and others can be called upon when it is not. However, a history of relationship trauma including loss and/or abuse predisposes someone to a variety of mental health and personality problems, as well as negative representations of the self as unworthy of protection or others unlikely to provide it when needed. Adult attachment representations have therefore been examined in many different kinds of clinical and high-risk populations, with the findings being that all tend to have higher rates of insecure relationship strategies, including those that are disorganized due to unresolved relationship trauma [4,5].
Developmental representational measures of adult attachment address thoughts and feelings about relationships, the impact of childhood attachment relationships on those thought patterns, and defense processes used to cope with relationship threat [6]. George and West [7] designed the Adult Attachment Projective Picture System (AAP) to directly assess attachment under threating conditions, and defensive processes that may be used to cope with these threats and anxiety-provoking evaluations of the self. They claim that the AAP is a trauma-sensitive measure, and it too has shown attachment insecurity is elevated in various clinical groups [5]. A less-common approach is to examine trauma history and indicators of psychopathology in high-risk samples. The goal of the current study is therefore to examine attachment representations using the AAP in a small sample of very high-risk mothers, many of which have histories of maltreatment of their own young children, and then relate these classifications to childhood trauma history, psychopathology, and personality disorders.
Adult Attachment and Psychopathology
There are many descriptions of how defensive processes underlie adult attachment representations and emotional regulatory strategies [8,9] based on Bowlby’s [3] original propositions. Defensive processes could either minimize relationship threat and involve avoidance of the emotional content of situations, which is a deactivating style typical of dismissing (Ds) attachment representations, maximize the threat and exaggerate emotional responses, which is the hyperactivating style typical of preoccupied (E) strategies, or defenses may fail altogether due to attachment threats being so overwhelming that emotions and thoughts become contradictory and lose their organized structure, which is typical of people whose relationship trauma history remains unresolved (U). When relationship threats can be quickly addressed by either seeking assistance from either others or an internalized attachment figure, the threat is quickly resolved and emotional response ultimately positive, which is typical of secure (F) attachment representations.
The Adult Attachment Interview (AAI) [10] is the most widely used measure of mental representations of attachment, in which someone is asked to describe their relationships with parents as well as other childhood attachment-related events. Transcribed interviews are then scored on scales related to past experiences with parents, current state of mind with respect to attachment, and whether these experiences are described in a coherent way. Ultimately a person is assigned to one of three attachment patterns of secure/autonomous, dismissing/ avoidant, preoccupied/enmeshed, or a fourth category in which attachment issues are unresolved/disorganized. The first three of these categories represent organized approaches to relationship threat, but the last category does not. Bakermans-Kranenburg and van IJzendoorn [4] completed a large scale meta-analysis of adult attachment distributions in many AAI studies of clinical and non-clinical groups, and found that the distribution of non-clinical classifications was 16% dismissing, 56% secure, 9% preoccupied, and 18% unresolved. However, they also examined high-risk and clinical samples, and found these distributions shifted with significantly lower rates of security and higher rates of insecurity, and unresolved classifications in particular. The highest rates of unresolved attachment were seen in studies of people with internalizing problems defined as suicidal ideation or Borderline Personality Disorder (BPD), as well as studies where there was some kind of abuse within the family or PTSD for some other kind of trauma. Other research has focused on preoccupied states of mind, and found preoccupied but not dismissing attachment is associated with a history of childhood abuse and neglect as well as non-suicidal self-injurious behavior [11,12] the latter being a diagnostic criteria of BPD [13].
Whereas clinical studies often examine one particular diagnostic group, potential comorbidity with other problems has been acknowledged, but rarely are Axis I and Axis II disorders considered at the same time [8]. In addition, relationship trauma may also be comorbid with mental health diagnoses, for example, over 90% of patients with BPD report a history of abuse and neglect [14]. There are other forms of combined risk, for example, low socioeconomic status (SES), child abuse history, and current violence in the family may co-occur, and thus compound unresolved relationship trauma and amplify the probability of insecure attachment classifications, psychopathology, personality disorders, and further family violence in adulthood [15-17]. For example, Chiesa, Cirasola, Williams, Nassisi and Fonagy [18] compared people formally diagnosed with an Axis II personality disorder to non-psychiatric controls. People with a personality disorder were far more likely to have experienced abuse and loss, and on the AAI, be unresolved for these experiences. They suggest that while attachment status is related to personality disorder, there is less predictive power of specific attachment categories with specific personality disorders, potentially due to their comorbidity and common underlying processes as a spectrum disorder [13].
The AAI addresses unresolved loss or trauma, but George and West [6] have argued that this is limited and not necessarily pursued during the interview. They point out that the representational nature of adult attachment should affect narrative structure, particularly when the attachment system is activated. They thus developed the AAP [19,7] as an alternative way of assessing adult attachment representations, which is a structured task in which adults are asked to create stories in response to a series of pictures that reflect attachment-related themes of separation, loss, and aloneness. George and West [7] describe how internal representations of attachment to provide safety and protection allows the needs, feelings, and perspectives of both self and other be integrated into a goal-corrected partnership and contribute to secure base behavior within stories generated. Secure individuals do not need defensive processes as they feel others can be called on in times of distress. However, when representations of attachment do not provide safety and security due to relationship trauma, then activation of the attachment system is threatening and behavioral strategies and defenses are used cope with anxieties and fears, or alternatively, overwhelm a person due to a history with caregivers and attachment figures of failed protection and abandonment. The narrative structures of stories are coded for these kinds of themes, and attachment is ultimately classified into the same four adult attachment AAI categories. George and West [7] report 90% concordance of the AAP with the AAI across four attachment categories in a diverse sample which included clinical and non-clinical groups of many ages, a finding replicated in a German sample [20]. However, another study [21] failed to find convergence in a fairly homogeneous 20-year-old college sample skewed towards high SES and over-represented by minority students. They concluded that this does not invalidate the AAP, but rather, the AAP and AAI may reflect different sets of experiences and states of mind with respect to attachment experiences.
The AAP has been used in a number of clinical studies. For example, in case studies of people with intellectual disabilities [22], unresolved classifications were assigned to both a man diagnosed with dysthymia and a woman with a history of physical and emotional abuse within her family, complex PTSD, and BPD. Other studies have used more common group comparison methods. For example, West and George [23] identified women that fit the diagnostic criteria for dysthymia, and found that rates of secure attachment were quite low and preoccupied attachment very high. Dysthymia was not related to elevations in unresolved classifications, but it is noted that the sample had experienced little trauma in the past. In contrast, a comparison of depressed inpatients to non-inpatient controls did not find differences in AAP distributions between the two groups [24]. The largest clinical group comparison study [5] using the AAP in 218 adults included those with psychiatric diagnoses of PTSD, BPD, depression, addiction, and schizophrenia, as well as controls. Rates of security were 54% for controls vs. 4% for psychiatric patients, with the latter rates uniformally low across all five clinical groups. Unresolved classification rates were 83% for PTSD and 76% for BPD, with most of the others being preoccupied in these two groups. Unresolved classifications were more moderate in depression and addiction groups and lowest in schizophrenia. Another German study [20] of multiple psychiatric groups and controls found low rates of security and high rates of unresolved classifications in patients with anxiety disorders and BPD compared to controls.
Taken together, these results are consistent with findings [4] using the AAI that clinical groups have higher than normal rates of adult attachment insecurity, but the specific nature of that insecurity varies between groups. The comorbidity problem also remains when only the primary diagnosis is used to form groups [5] and in the case of PTSD, this does not provide information on whether the trauma was related to relationship history or some other form of trauma such as medical traumas and accidents [25,26]. Whereas BPD and antisocial personality disorders are significant Axis II disorders and associated with history of childhood abuse [8,14] there is little information on the relations between attachment classifications, other forms of personality disorders, and trauma specific to relationships.
Attachment, Relationship Trauma and Abuse
There is considerable interest in relationship traumatization, life-long mental health problems, and attachment representations [27]. For example, an epidemiological study [28] showed childhood relationship traumas of loss of a parent and adverse parenting practices predicted a variety of anxiety, mood, and substance-use disorders in adulthood, and these effects were greater when the loss was at a younger than older childhood age. Another study [29] found that a history of childhood trauma and particularly emotional and sexual abuse was higher for those adults with social anxiety compared to psychiatric and healthy controls. Kaehler and Freyd [16] examined physical abuse history and found that this kind of significant relationship betrayal predicted BPD features in women, and mothers with diagnosed BPD were more likely to have preoccupied/unresolved attachment status but not more likely to be dismissive [30]. In a study of people presenting at a psychiatric outpatient clinic [31], physical and emotional child abuse history was positively correlated with elevated scores on the MMPI-2 in a number of different dimensions including psychopathic deviate, paranoia, psychasthenia, and schizophrenia. They also point out that this symptom complexity may be accounted for by underlying processes such as emotion regulation difficulties, and others have similarly suggested that childhood trauma is associated with these deficits [15,11,32].
A small number of studies have integrated attachment representations with childhood abuse history and mental health outcomes. For example, in a study using the AAP to assess attachment representations [33], adolescents with maltreatment histories were found to have high rates of unresolved classifications, 18% Ds, 24% F, 16% E, and 42% U, and a majority of unresolved teens had a history of some form of abuse. Maltreatment history is not only related to lower security and higher unresolved attachment in adulthood [4,8], but similar effects are found in child-parent attachment when disorganized attachment is synonymous with the unresolved category. For example, in a meta-analysis of studies examining child attachment classifications in various risk conditions [34], those in high- compared to low-risk conditions displayed less secure and more disorganized attachment classifications and these effects were highest for those with maltreatment histories.
A small number of studies have specifically related childhood trauma with adult attachment assessed using the AAI. For example, Bailey, Moran, and Pederson [35] examined teenage mothers as an at-risk sample and related AAI classifications to interview and self-report measures of childhood abuse history. On interview data, 55% of those reporting physical and 71% who reported sexual abuse histories were classified as unresolved, and the general self-report measure of abuse was also related to an unresolved classification. In another example [36], the AAI was used to show that adolescents with a sexual abuse history were more likely to be classified as unresolved than either those depressed or non-clinical controls.
Other approaches have been used to examine these issues with respect to family violence. Murphy et al. [37] examined community and clinical samples of mothers in which the latter were mothers referred from pediatric or child protection services due to concerns about parenting ability to meet child needs.
Their goal was to relate adverse childhood experiences to AAI classifications, with the former including variables addressing physical and sexual abuse, neglect variables, and household dysfunction; variables which can be reframed as emotional abuse or neglect (i.e., witnessing domestic violence, substance abuse by a parent). Not surprisingly, clinical samples reported many more adverse childhood experiences than controls. Percentages for secure and unresolved classifications for community and clinical samples, respectively, were 50% secure and 20% unresolved for the community group and 5% and 76%, respectively, for the clinical group. Further, when a metric of degree of childhood adversity was created, those with the highest scores had the highest level of unresolved classifications, with witnessing their mother being treated violently during childhood being the most salient predictor. Similarly [15], adult women seeking services for interpersonal violence have been examined to show that those who were unresolved were more likely to have witnessed family violence in childhood and experienced multiple forms of other childhood trauma. AAI data thus point to child abuse history as a correlate of unresolved attachment in adulthood, but no such data exist for the AAP.
The Present Study
In the present study, the AAP was used to assess adult attachment. A small sample of very high-risk mothers of young children was examined, most of which had active maltreatment histories of their own children defined as contact with child protection services. Given the nature of high-risk, it was hypothesized that high rates of adult insecurity would be found, including unresolved attachment. In addition, mothers completed a childhood relationship trauma questionnaire, a measure of both Axis I psychopathology and Axis II personality disorder, and of depression. High rates of psychopathology related to anxiety, depression, and personality disorder were expected, particularly for preoccupied and unresolved mothers, and more specifically, high rates of other Cluster B personality disorders that involve impulsive, dramatic, emotional, and erratic behavior that could reflect relationship trauma. In the current study, data are not represented as scores, but categorically as scores above or below multiple clinical cutoffs for the respective measures, which is how these measures are used in clinical practice. Differences in relationship trauma, psychopathology, personality, and depression between attachment categories were examined in this way. It was originally expected that secure and dismissive mothers would report the fewest problems in these areas and unresolved and preoccupied mothers the most. As it turned out, none of the mothers were classified as secure, so distinctions between the three insecure categories became the focus.
Method
Participants
Participants consisted of 18 women ranging in age from 20 to 40 years, M=31.1, SD=5.77, in a rural area of East Coast Canada. Each woman had at least one child 2 to 8 years of age, and the total number of children living in the home ranged from 1 to 5, M=3.0. This was a high psychosocial risk sample, and risk indicators were failure to complete high school, n=4, 22%, single-parent, n=9, 50%, teenage parent, n=2, 11%, living below the national poverty line for a particular family size, n=16, 89%, lived away from their parent(s) as a child, n=5, 28%, and maltreatment concerns in current family defined by formal contact with child protection services, n=14, 78%. Ethnicity of all the women was White. Four children (22%) had biological fathers either of African-Canadian or African-Caribbean ethnicity, with the other 14 being White. All were recruited through the Kids Action Program, which provides a variety of family support services to high psychosocial risk families, many of which have formal child protection concerns and self-reported stress and mental health needs.
Measures
The Adult Attachment Projective Picture System (AAP) [7] was used to assess adult attachment representations. It consists of drawings of one neutral scene and seven scenes designed to activate the attachment system by depicting potential separation, loss, aloneness, and harm. While the attachment context is clear from the drawings, there are no facial expressions, actions, or postures that make it obvious what is happening. Participants are then asked to create a story for each picture, with structured prompts to address details of the story if they are omitted such as what led up to and follows from the scene, as well as thoughts and feelings of characters. These stories are then audiotaped, transcribed, and then coded for adult attachment status. The AAP takes about 30 minutes to complete.
Coding of the transcripts is highly structured and complex [7] and includes story content, how the character copes with the situation in the picture, whether characters receive care from others or seek to repair relationships and make connections with others, and three forms of defensive processes used to cope with the material. In deactivation, attention is shifted away from the attachment-caregiving context of the story to something else like social rules, sexual activity, achievement, or exploration, all central to dismissing attachment (Ds). In cognitive disconnection, elements of attachment are disconnected from their source, and thus stories are uncertain with multiple possible story-lines, events, or feelings; a focus on emotions related to problems rather than the problems themselves; and, personal experiences may intrude into stories, all of which are indicative of preoccupied attachment (E). Sometimes the attachment theme shown in the picture is so threatening that thought, behavior, and feelings become disorganized and chaotic in the story, and reflect a traumatic response to threatening and even frightening material. Stories may convey fear, helplessness, being uncontrolled, unprotected, or abandoned, and may even reflect dissociative symptoms. These kinds of responses are referred to as segregated systems, and what is important is whether these kinds of responses are contained and reorganized, in other words, go through “resolution” so the story can return to an agency of self or functional assistance from others. This resolution does not happen in unresolved attachment (U). In addition, people classified as U receive an alternate code from resolved categories to reflect what their attachment style is when they are organized in their responses, in other words, what their predominant defense strategy is when their stories do not break down. In secure attachment (F), participants relay stories in which characters can contain threatening material, but they reach out to others for assistance and comfort, and thus can use others as a secure base. Stories may still reflect defensive processes, but these are used to integrate attachment feelings and not exclude them nor transform them into something else.
Coding decision rules have been detailed [7] and the AAP validation study of community and college recruits reports the breakdown of categories to be 17% secure, 26% dismissing, 21% preoccupied, and 36% unresolved. The four-group classification on the AAP has also been shown to have convergent validity with the AAI, κ=0.79, and 12-week test-retest reliability, κ=0.78, by the test authors [21]. In the current study, stories were coded blindly and independently by an accredited coder (C.S.) and a second one (M.W.) blindly coded 10 of these transcripts. There was 80% agreement on their AAP codes. It should be noted that the two disagreements were a U/E vs. E and U/Ds vs. Ds, so in fact there was 100% agreement on the primary defensive process if the alternate code is taken into consideration. The two coders conferred to achieve consensus on what the final category should be for these two protocols. In addition to study participants, two women completed the AAP but later withdrew from the study and did not complete other measures, so they are excluded.
The Childhood Trauma Questionnaire (CTQ) [38] contains 28-Items that assess childhood maltreatment that generate subscale scores for emotional abuse, physical abuse, sexual abuse, and two neglect subscales. Items are rated on a five-point scale from never to very often true. In addition, there are three items that address Minimization/Denial of problems within the family and may indicate an under-reporting of maltreatment experiences. Adequate internal consistency for subscales has been reported across a number of clinical and medical populations, testretest reliability has been reported over a 3 or 4 month period (rs>0.79), there has been concurrent validation with other clinical measures and therapist ratings of maltreatment history. Total scores within each subscale can then be assigned to one of four ranges of scores indicating None or Minimal, Low to Moderate, Medium to Severe, and Severe to Extreme. These ranges have been cross-validated against interview ratings after an in-depth trauma interview. For the purposes of this study, only emotional, physical, and sexual abuse scales used. A total abuse score was created by assigning one point for every category of abuse in the Medium to Severe range and two points for categories in in the Severe to Extreme range.
The Millon Clinical Multiaxial Inventory, 3rd Edition (MCMI-III) [39] was used to assess personality disorders and psychopathology. The MCMI-III was normed on various psychiatric and clinical populations, and thus very useful at distinguishing forms of psychopathology based on DSM-V criteria [13]. It consists of 175 self-report questions in true/ false format and contains 14 Clinical Personality Pattern Subscales, 10 Clinical Syndrome Scales, and three Modifying Indices. Raw scores for each subscale are converted to base rate scores according to normative information provided for clinical samples of females, and these are then adjusted for modifying indices of Disclosure, Social Desirability, and Debasement. Base rate scores between 75 and 85 indicate the presence of trait or syndrome and scores 85 and above indicate prominence, with the latter representing higher severity.
In the current study, the 10 Axis-II personality disorders from DSM-V were addressed using the corresponding MCMI-III subscales which are organized into three Clusters: Paranoid, Schizoid, and Schizotypal (Cluster A); Antisocial, Borderline, Histrionic, and Narcissistic (Cluster B); and, Avoidant, Dependent, and Obsessive-Compulsive (Cluster C). Cluster A involves odd, eccentric, and socially withdrawn behavior, Cluster B involves impulsive, dramatic, emotional, and erratic behavior, and Cluster C involves anxious and fearful behavior. It is acknowledged that the nature of personality disorders are being intensely debated [40] with attention on the profile of current or future categories, dimensional reorganization of symptoms, clinical spectrum approaches, and integration with general personality function. In the current study, total personality disorder score was calculated by giving participants one point for every category in the presence range and two points if in the prominence range.
In addition, all 10 of Millon’s Axis I Clinical Syndrome Scales were examined: Anxiety, Somatoform, Bipolar, Dysthymia, Alcohol Dependence, Drug Dependence, PTSD, Thought Disorder, Major Depression, and Delusional Disorder. These subscale scores are related, so the highest two subscale scores are the most important, and a score above a cutoff considered alone does not constitute a formal clinical diagnosis. Again, base rate scores indicate presence and prominence of a disorder, and in the current study, total psychopathology score was calculated by giving participants one point for every category in the presence range and two points if in the prominence range.
The MCMI-III and its earlier versions have been very widely used with various clinical and high- risk samples, and subscales have been shown to have good internal consistency (αs>0.66), test-retest reliability across 1 to 2 weeks (rs>0.81), and concurrent validity with other clinical and normative measures of personality and aspects of mental health.
The Beck Depression Inventory, 2nd Edition (BDI-II) [41] is a widely used 21-item self-report measures addresses cognitive, affective, and somatic symptoms of depression. Each item contains four descriptive statements over the past two weeks scored on a 0 to 3 scale. A total raw score is derived by summing items, and this total score can be assigned to a range of scores indicating Minimal, Mild, Moderate, and Severe Depression. Cut-off scores for these ranges were derived by cross-validating BDI scores against clinical groups with known degrees of diagnosed depression [41]. The scale has excellent internal consistency (α ≥ 0.90), test-retest reliability at one week (r=0.93), and good concurrent validity with self-report and clinician diagnoses of depression.
Procedure
Women were recruited through a local organization that provides a variety of services to families at extreme psychosocial disadvantage, some of which have had contact with child protection services. All woman provided written informed consent before they participated, and this project was approved by the Research Ethics Board of Acadia University, which follows Canada’s Tri-Council Policy Statement: Ethical Conduct for Research Involving Humans. During a visit to research space, the AAP was administered, questionnaires were completed, and participants were engaged in other activities not related to this study. Participants with poor reading ability had items read aloud to them or received other assistance as needed. Women attended the lab visit with their young child, but completed the above activities while their child was engaged in adjacent room in tasks unrelated to this study.
Results
The breakdown of AAP classifications was preoccupied, n=5 (28%), dismissing, n=4 (22%), and unresolved, n=9 (50%). None of the participants were classified as secure. Chi-Square Goodness of Fit Tests were used to compare the current observed distribution of AAP classifications to that expected from AAP norms [7]. The current distribution of scores did not significantly differ from that expected either when all four categories were used, χ2(3)=4.53, p=0.21, or categories were collapsed into resolved vs. unresolved classifications, χ2(1)=1.53, p=0.22. Of the 9 participants classified as unresolved, one (11%) received an alternate code of dismissive and 8 (88%) received an alternate code of preoccupied.
The results of this study can be found in Figure 1, with further details in Appendix 1. In Figure 1, abuse history broken down by adult attachment classification was seen as present if people reported one form of abuse in the medium to severe or severe to extreme ranges. Overall, 12 (66%) of the women reported at least one clinically-significant level of abuse history, with nine of these reporting at least one form of abuse history in the severe to extreme ranges. In addition, three of the women met criteria for minimization of possible maltreatment history, and two of these were classified as unresolved and one dismissive. Only three women either reported no abuse or did not minimize their reports, and two of these were dismissive. Only one of four dismissive women reported a significant history of abuse. However, all five of the preoccupied women reported this history, with four in the severe to extreme range, and 6 of the 9 unresolved women reported abuse history, with 4 in the severe range.
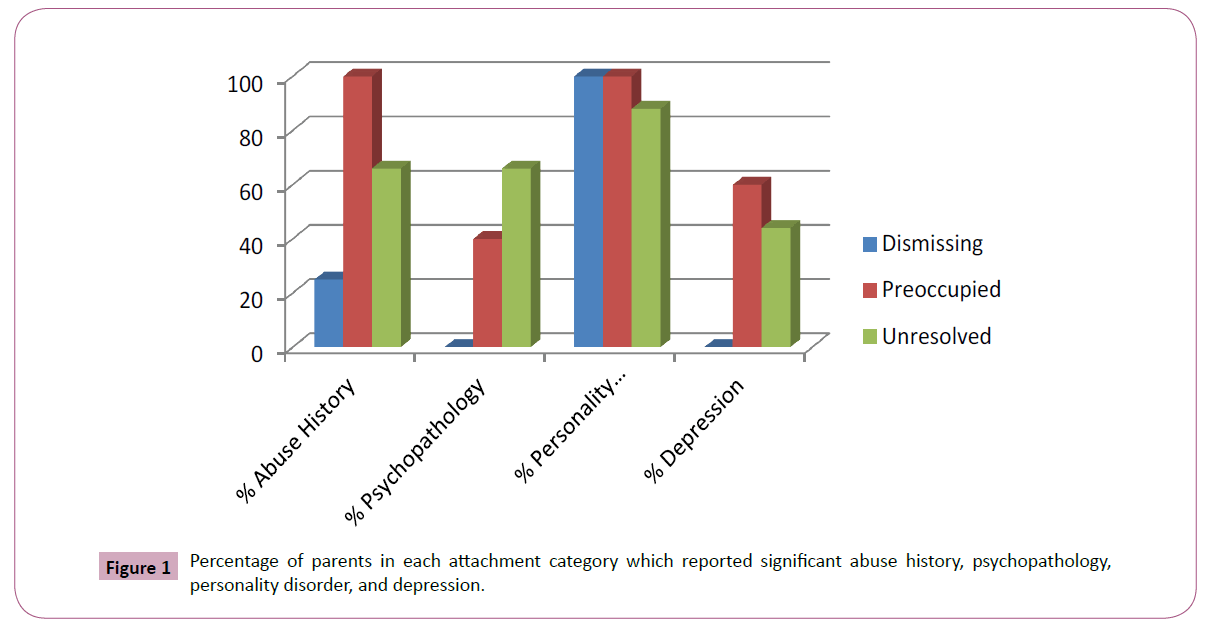
Figure 1: Percentage of parents in each attachment category which reported significant abuse history, psychopathology, personality disorder, and depression.
The data analytic plan was to conduct Kruskall-Wallis tests on total scores to compare adult attachment categories using an alpha of 0.10 because of the small sample size. When this was done on total abuse scores, significant differences in abuse history were found between adult attachment categories, H(2)=5.45, p=0.07. Dismissing women had the lowest scores, preoccupied the highest, and unresolved were intermediate. Appendix 1 provides person-by-person details of the nature of abuse history. The significant kinds of abuse are written in plain text when in the medium to severe range, and the severe to extreme range if noted in bold.
The primary defense strategy can also be examined by reassigning unresolved women into their alternate code classifications, which results in 5(28%) women with a primary defense strategy as dismissing and 13(72%) as preoccupied. Reclassified in this way, rates of a reported abuse history were 2 in 5(40%) for dismissing and 10 in 13(77%) for preoccupied.
Figure 1 also displays the percentage of women within each attachment category that scored in at least one MCMI-III category for the presence or prominence clinical ranges of personality disorders and psychopathology. The details of specific subscales are found in Appendix 1, in which mental health problems indicate the presence of the disorder, unless noted in bold, which indicates the more severe prominence of the disorder. Multiple disorders are possible as participants could be above base rate cutoffs on more than one problem, and so the disorders are organized within each column in the order of severity for a person within both the Axis II personality disorder and Axis I psychopathology sections. Overall, 17 (94%) of the women met criteria for at least one personality disorder, with seven of these falling into the more severe prominence category. The most common of these were the Cluster B personality disorders of Histrionic, n=8, Narcissistic, n=6, BPD, n=5, and Antisocial, n=1, in fact, 14 (78%) women reported at least one Cluster B disorder, some more than one, and there were similar rates across all three categories. Less common were Cluster A and C personality disorders. There were no differences in total personality disorders between AAP classifications, H(2)=0.48, p=0.79.
In addition, Millon et al. [39] identified three personality disorders that are more severe than others: Schizoid, BPD, and Paranoid. Of the 5 participants who met criteria for BPD, 3 were classified as Preoccupied and the other 2 were Unresolved, with a secondary classification of Preoccupied. Of the five participants who met criteria for Paranoid, on the other hand, all three insecure attachment classifications were represented.
In terms of psychopathology, 8(44%) of the women reported an Axis I problem on clinical syndrome subscales, with half of these scoring in the more severe range. Two people met criteria for Somatoform Disorder and one each for PTSD, drug dependency, and delusional disorder. Seven of the 8 reported some combination of Anxiety and Depression. These results were corroborated by BDI-II scores, which for all but one of these eight women were in the Moderate or Severe ranges. Of the 11 women who reported Minimal or Mild Depression on the BDI-II, only one (9%) reported an Axis I clinical syndrome. There were significant differences in total psychopathology between attachment classifications, H(2)=4.75, p=0.09. Figure 1 shows that none of the dismissive mothers reported psychopathology, whereas 2 of 5 (40%) preoccupied mothers and 6 of 9 (66%) unresolved mothers did. The women with maltreatment concerns in their current family accounted for all the clinical syndrome reports and BDI-II scores in the moderate or severe ranges. Women without these concerns reported neither kind of problem. If the alternate defense strategy is taken into consideration, 7 of the 8 mothers reporting a clinical syndrome were classified as either preoccupied or unresolved with an alternate code of preoccupied.
Finally, Figure 1 shows the percentage of women scoring in Moderate or Severe ranges of depression on the BDI. Although none of women in the dismissing category reported these levels of depression, there were no significant differences in BDI scores across attachment classifications, H(2)=1.39, p=0.50.
Discussion
This study examined adult attachment representations, childhood abuse history, and indicators of psychopathology and personality disorders in a small sample of very high-risk mothers. The AAP was used as it has been argued to be clinically-oriented, sensitive to a history of relationship trauma, and examines defenses used in a story-telling task when the attachment system is activated [6,7]. Differences in abuse history and psychopathology were examined between attachment classifications using cutoff scores as these scores are commonly used in clinical practice. In the current study, none of the women were classified as secure, 28% preoccupied, 22% dismissing, and 50% unresolved. This AAP distribution of classifications was comparable to the norms [7] and those for clinical groups [5]. While there were a number of risk factors in this sample that could contribute to adult insecurity, the two most common were poverty and formal contact with child protection services due to concerns about maltreatment of their own children.
All of the women had multiple problems reflected in terms of some combination of their own history of childhood abuse and indices of psychopathology. The current data are therefore consistent with research using the AAI that has shown that a history of child maltreatment and other relationship trauma is associated with low rates of adult security and high rates of unresolved attachment classifications [4,15,35]. There is little longitudinal data using the AAP, but in one exception [42] in low-risk teens, little overall continuity from infant attachment classifications to adult attachment was found. But when negative life and relationships events were taken into account, AAP attachment representations were predicted, largely due to secure children becoming unresolved teens when they had a negative relationship history. In the current study, many women reported a childhood abuse history and this would certainly constitute the kind of relationship trauma that can contribute to insecure adult attachment representations regardless of their attachment classification in childhood. In addition, many of the mothers had active involvement with community services for maltreating their own children, almost all of these mothers reported an abuse history, and they accounted for all the major mental health problems [37]. In contrast, of the four women with no child protection involvement, only two reported an abuse history and none reported major mental health problems. This supports clinical impressions that women with maltreatment concerns in their current family often have many challenges including abuse within their own history, maladaptive strategies within their current approach to relationships, and mental health problems.
The least amount of difficulty appeared to be with the four women classified as dismissive as none reported significant psychopathology, only one a severe personality disorder, and only one an abuse history, and there were significant group differences in total abuse history and total psychopathology. The unresolved and preoccupied women therefore reported most of the abuse history, most of the personality disorders, and all of the psychopathology. In fact, high rates of the unresolved women received a secondary classification of preoccupied when the defenses were intact, which has been found before with woman with dysthymia [23].
The primary defense strategy associated with mental health problems was cognitive disconnection, in which there is overattention to details of attachment experiences and own personal relationship history, as well as a focus on emotions related to problems rather than the problems themselves and potential solutions. Five of the women maintained this defensive strategy throughout the AAP and were preoccupied, and for nine, the history of trauma caused a collapse of this strategy that resulted in disorganization of thought and feeling from which they could not recover, and thus an unresolved classification [7]. Cognitive disconnection is similar to descriptions of the attachment system being hyperactivated to threat and attachment-related events [9]. A high proportion of the mental health problems revolved around anxiety and depression, so it should not be surprising that a preoccupied defense strategy was used by these women given the association of anxiety, preoccupied classifications, and emotional regulation problems [8,11].
It has been suggested that a history of child abuse leads to emotional regulation difficulties and these underlie later psychopathology [15,31,32]. In the current data, not only did most of the clinical syndrome data revolve around anxiety and depression, but the Axis II personality disorder data most commonly included Cluster B Disorders. Cluster B personality disorders involve impulsive, dramatic, emotional, and erratic behavior that could arise from relationship trauma and reflect emotional regulation problems, with Histrionic being most common but BPD the most serious. While the current data did not suggest these were more common in unresolved than preoccupied classification as has been found elsewhere [4,5,20], they were more common in women with a primary defense strategy of cognitive disconnection than deactivation (i.e., dismissing). It is interesting that in the new dimensional model of Personality Disorders [13], BPD remains but Histrionic has been removed. However, one of the underlying trait domains for personality disorders is negative affectivity versus emotional stability, which would reflect the ability to regulate emotions [40]. George and West [7] have reviewed how emotional regulation difficulties not only underlies adult attachment classifications, but also has a biological basis in brain function in response to attachment-activating stimuli which may be at a low threshold and lead to hyperactivation [9,43].
There are a number of limitations to this study. Most obviously, the sample size is small so the data are simply descriptive of patterns of co-classifications. Statistical tests could only be of total scores and not individual categories or problem areas. On the other hand, the data are very rich and permit an examination of all kinds of relationships between the constructs at hand using commonly used assessment measures. Second, there were no secure attachment representations, so no comparisons could be drawn to comorbid patterns in secure high-risk mothers. Third, it is possible that there was a recruiting bias towards relatively more challenged parents. For example, it is possible that child protection services are able to effectively deal with parents who come to their attention for maltreatment concerns and do not have as many complicating problems as this sample. Only when these services fail to provide help is there a referral to the outside agency used in the current study, in other words, this sample may not be representative of the general population of parents involved with child protection services. Further, as the data was collected in a rural area, it is possible that risk factors may be compounded by things like isolated living situations and severe poverty.
It is useful to consider just how complicated people’s lives are when attachment representations, childhood trauma history, and mental health problems are seen in combination as they are in clinical work. The data presentation strategy in this study was clinically-oriented in that scores were presented using clinically significant cutoffs. This allowed patterns of comorbidity and the magnitude of problems to be more readily apparent in a descriptive fashion, although these data do not reflect clinical diagnoses, and elevations on multiple scales may simply reflect a primary problem that is correlated with lesser elevations on other scales. Regardless, the AAP is a relatively new measure, and the current data support claims it is particularly sensitive to relationship trauma and mental health problems. The AAP has not been used with parents primarily involved with child protection services, so the absence of secure classifications is striking. Although it appeared 14 years ago [19], it has recently become more formalized [7], and studies using it have only appeared relatively recently. In sum, the current study contributes to the growing research base that examines adult attachment representations in various at-risk and clinical groups, which supplements what we have already learned from AAI studies [4]. These studies contribute to the development of Bowlby’s [3] original emphases on attachment’s representational structure that contains defensive processes, as well as how relationship trauma and psychopathology may be related to these processes.
Author Contribution
This research was supported by grants from the Social Sciences and Humanities Research Council of Canada, the Nova Scotia Research Foundation and IWK-Grace Health Centre. C. George, M. West, and C. Sundheim are thanked for AAP training, coding, and comments. K. Smith, A. Webster, K. Wilson, and J. Meisner are thanked for data scoring and management and the Kids Action Program is thanked for facilitating participation.
References
- Bowlby J (1969/1982) Attachment and loss, Vol. 1: Attachment. New York: Basic Books.
- Bowlby J (1973) Attachment and loss, Vol. 2: Separation. New York: Basic Books.
- Bowlby J (1980) Attachment and loss, Vol. 3: Sadness and Depression. New York: Basic Books.
- Bakermans-Kranenburg MJ, van IJzendoorn MH (2009) The first 10,000 adult attachment interviews: distributions of adult attachment representations in clinical and non-clinical groups. Attach Hum Dev 11: 223-263.
- Juen F, Arnold L, Meissner D, Nolte T, Buchheim A (2013) Attachment disorganization in different clinical groups: What underpins unresolved attachment? Psihologua 46: 127-141.
- George C, West ML (2011) The adult attachment projective picture system: integrating attachment into clinical assessment. J Pers Assess 93: 207-416.
- George C, West ML (2012) The adult attachment projective picture system. New York: The Guilford Press.
- Dozier M, Stovall-McClough KC, Albus K (2008) Attachment and psychopathology in adulthood. In: Cassidy J, Shaver PR, Handbook of attachment: theory, research, and clinical applications, 2nd Edn, New York: Guilford, pp: 718-744.
- Mikulincer M, Shaver PR (2008) Adult attachment and affect regulation. In: Cassidy J, Shaver PR eds. Handbook of attachment: theory, research, and clinical applications, 2nd Edn, New York: Guilford, pp: 503-531.
- Main M, Kaplan N, Cassidy J (1985) Security in infancy, childhood, and adulthood: A move to the representational level. In: Bretherton I, Waters E, Growing points of attachment theory and research. Monogr Soc Res Child Dev 50: 66-104.
- Martin J, Raby KL, Labella MH, Roisman GI (2017) Childhood abuse and neglect, attachment states of mind, and non-suicidal self-injury. Attach Hum Dev 5: 425-446.
- Raby KL, Labella MH, Martin J, Egeland B, Roisman GI (2017) Adverse caregiving experiences during childhood predict insecure attachment states of mind in adulthood: Prospective longitudinal evidence from a high-risk sample. Dev Psychopathol 29: 347-363.
- APA (2013) Diagnostic and statistical manual of mental disorders, 5th Edn. Washington, D.C: APA.
- Zanari MC (2000) Childhood experiences associated with the development of borderline personality disorder. Psychiatr Clin North Am 23: 89-101.
- Alexander PC (2009) Childhood trauma, attachment, and abuse by multiple partners. Psychol Trauma 1: 78-88.
- Kaeler LA, Freyd JJ (2012) Betrayal trauma and borderline personality characteristics: gender differences. Psychol Trauma 4: 379-385.
- Milner JS (2010) Do trauma symptoms mediate the relationship between childhood physical abuse and adult child abuse risk? Child Abuse Negl 34: 332-344.
- Chiesa M, Cirascola A, Williams R, Nassisi V, Fonagy P (2017) Categorical and dimensional approaches in the evaluation of the relationship between attachment and personality disorders: an empirical study. Attach Hum Dev 19: 151-169.
- George C, West M (2001) The development and preliminary validation of a new measure of adult attachment: the adult attachment projective. Attach Hum Dev 3: 30-61.
- Buchheim A, George C (2011) Attachment disorganization in borderline personality disorder and anxiety disorder. In Solomon J, George C Edn: disorganized attachment and caregiving. New York: Guilford, pp: 343-382.
- Jones-Mason K, Allen IE, Hamilton S, Weiss SJ (2015) Comparative validity of the adult attachment interview and the adult attachment projective. Attach Hum Dev 17: 429-447.
- Gallichan DJ, George C (2014) Assessing attachment status in adults with intellectual disabilities: the potential of the adult attachment projective picture system. Adv Ment Health Intellect Disabil 8: 103-119.
- West M, George C (2002) Attachment and dysthymia: The contributions of preoccupied attachment and agency of self to depression in women. Attach Hum Dev 4: 278-293.
- Fizke E, Buchheim A, Juen F (2013) Activation of the attachment system and mentalization in depressive and healthy individuals – an experimental control study. Psihologua 46: 161–176.
- Benoit M, Bouthillier D, Moss A, Rousseau C, Brunet A (2010) Emotion regulation strategies as mediators of the association between level of attachment security and PTSD following trauma in adulthood. Anxiety Stress Coping 23: 101-118.
- Juen F, Rattensberger V, Buchheim A (2014) Attachment and posttraumatic symptomatology following physical injury accidents. Psihologua 47: 81-92.
- Bernstein RE, Freyd JJ (2014) Trauma at home: how betrayal trauma and attachment theories understand the human response to abuse by an attachment figure. Attachment 8: 18-41.
- Nickerson A, Bryant RA, Aderka IM, Hinton DE, Hofmann SG (2013) The impacts of parental loss and adverse parenting on mental health: findings from the national comorbidity survey - replication. Psychol Trauma 5: 119-127.
- Michail M, Birchwood M (2014) Social anxiety in first-episode psychosis: the role of childhood trauma and adult attachment. J Affect Disord 163: 102-109.
- MacFie J, Swan SA, Fitzpatrick KL, Watkins CD, Rivas EM (2014) Mothers with borderline personality and their young children: adult attachment interviews, mother-child interactions, and children’s narrative representations. Dev Psychopathol 26: 539-551.
- Choi JY, Choi YM, Gim MS, Park JH, Park SH (2014) The effects of childhood abuse on symptom complexity in a clinical sample: mediating effects of emotion regulation difficulties. Child Abuse Negl 38: 1313-1319.
- Young JC, Widon CS (2014) Long-term effects of child abuse and neglect on emotion processing in adulthood. Child Abuse Negl 38: 1369-1381.
- Webster L, Hackett RK, Joubert D (2009) The association of unresolved attachment status and cognitive processes in maltreated adolescents. Child Abuse Rev 18: 6-23.
- Cyr C, Euser EM, Bakermans-Kranenburg MJ, van IJzendoorn MI (2010) Attachment security and disorganization in maltreating and high-risk families: a series of meta-analyses. Dev Psychopathol 22: 87-108.
- Bailey HN, Moran G, Pederson DR (2007) Childhood maltreatment, complex trauma symptoms, and unresolved attachment in an at-risk sample of adolescent mothers. Attach Hum Dev 9: 139-161.
- van Hoof MJ, van Lang NDJ, Speekenbrink S, van IJzendoorn MH, Vermeiren R (2015) Adult attachment Interview differentiates adolescents with childhood sexual abuse from those with clinical depression and non-clinical controls. Attach Hum Dev 17: 354-375.
- Murphy A (2014) Adverse Childhood Experiences (ACEs) Questionnaire and Adult Attachment Interview (AAI): Implications for parent-child relationships. Child Abuse Negl 38: 224-238.
- Bernstein DP, Fink L (1997) Childhood trauma questionnaire: a retrospective self-report. Pearson Canada.
- Millon T, Davis R, Millon C (1997) Millon clinical multiaxial inventory –III (2nd Edn). Minneapolis: National Computer Systems Inc.
- Kruger RF, Markon KE (2014) The role of the DSM-5 personality trait model in moving toward a quantitative and empirically-based approach to classifying personality and psychopathology. Annu Rev Clin Psychol 10: 477-501.
- Beck AT, Steer RA, Brown GK (1996) Beck depression inventory manual, 2nd Edn. San Antonio, TX: Psychological Corporation.
- Aikens JW, Howes C, Hamilton C (2009) Attachment stability and the emergence of unresolved representations during adolescence. Attach Hum Dev 11: 491-512.
- Fonagy P, Luyten P, Strathe L (2011) Borderline personality disorder, mentalization, and the neurobiology of attachment. Infant Ment Health J 32: 47-69.
| # |
AAP |
Abuse |
Personality Disorders |
Psychopathology/ Clinical Syndromes |
BDI Range |
| 1 |
Ds |
Minimized |
Histrionic |
|
Mild |
| 2 |
Ds |
Emotional |
Histrionic, Narcissistic |
|
Mild |
| 3 |
Ds |
Sexual |
OCD, Narcissistic, Histrionic |
|
Mild |
| 4 |
Ds |
Emotional, Physical |
Paranoid |
|
Mild |
| 5 |
E |
Physical |
Histrionic, Borderline, Paranoid |
Anxiety |
Severe |
| 6 |
E |
Emotional, Physical |
Histrionic, Narcissistic, OCD |
|
Minimal |
| 7 |
E |
Physical |
Borderline |
|
Mild |
| 8 |
E |
Emotional, Physical |
Borderline |
Anxiety, Bipolar, Depression |
Severe |
| 9 |
E |
Emotional, Physical |
OCD |
|
Moderate |
| 10 |
U/E |
Physical |
Avoidant, Paranoid |
Somatoform, Anxiety, Depression |
Severe |
| 11 |
U/E |
Minimized |
Histrionic |
|
Minimal |
| 12 |
U/E |
|
Avoidant, Paranoid, Schizoid, Narcissistic |
|
Minimal |
| 13 |
U/E |
Sexual |
Histrionic |
Drug Dependence |
Minimal |
| 14 |
U/E |
Emotional, Physical |
Narcissistic, Anti-social, Borderline |
Bipolar |
Moderate |
| 15 |
U/E |
Emotional, Physical |
|
PTSD, Depression, Dysthymia, Somatoform, Anxiety |
Moderate |
| 16 |
U/E |
Minimized |
Narcissistic, Histrionic |
|
Minimal |
| 17 |
U/E |
Emotional |
Paranoid, Avoidant, Dependent, Borderline |
Delusional, Depression, Dysthymia, Anxiety |
Moderate |
| 18 |
U/Ds |
Emotional, Physical |
Narcissistic, OCD |
Anxiety |
Mild |
Notes: Problem areas are noted when above a clinical cutoff, and in bold when in a more severe range. AAP Codes, U = Unresolved; E = Preoccupied; and Ds = Dismissive; with alternate codes noted for U. OCD = Obsessive-Compulsive Disorder; PTSD = Post-Traumatic Stress Disorder; and BDI = Beck Depression Inventory.
Appendix I: Adult attachment projective (AAP) categories, childhood abuse history, and psychopathology indicators in 18 high risk mothers.

