Keywords
Alcohol Drinking; Mortality; Pancreatitis; Russia
INTRODUCTION
Pancreatitis is a major public health problem with high associated economic costs [1]. The incidence of pancreatitis has increased in many European countries in recent decades [2, 3]. Increase of acute pancreatitis over time were greater in the younger age group which probably represent an increase in alcoholic pancreatitis, as acute pancreatitis among young people is more commonly alcohol related [4, 5]. The incidence of acute pancreatitis varies considerably throughout the region and tended to be highest in Scandinavia and Eastern Europe [2]. The reasons for geographic differences in incidence of pancreatitis are still poorly understood and most likely are because of differences in the risk factors, including alcohol consumption [6]. Since an association between alcohol abuse and pancreatitis was reported by Friedreich in 1878 [7], many studies have confirmed that excessive alcohol consumption is a major risk factor for both acute and chronic pancreatitis [1, 8-10]. The strong support for a close link between alcohol and pancreatitis come from individual level studies [11, 12]. Using data on 17905 men and women who participated in the Copenhagen City Heart Study Kristiansen et al. reported that a high alcohol intake is associated with a high risk of pancreatitis [13]. A recent systematic review and metaanalysis of epidemiologic studies on alcohol consumption and pancreatitis published between 1980 and 2008 found a monotonic and approximately exponential doseresponse relationship between average volume of alcohol consumption and the risk of pancreatitis [14]. Collectively, these findings suggest that the total amount of alcohol consumed is a critical factor in producing chronic alcoholinduced pancreatic damage.
There is, however, evidence that pattern of drinking may have modifying influence on pancreatitis risk independently of the amount of alcohol consumed. A follow-up study from Sweden revealed a dose-response association between the amount of spirits consumed on a single occasion and the risk of acute pancreatitis [15]. After multivariate adjustments, there was a 52% increased risk of acute pancreatitis for every increment of five standard drinks of spirits consumed on a single occasion [15]. There is also empirical evidence suggesting that the holidays binge drinking may influence on the incidence of acute pancreatitis. In particular, Roberts et al. reported an increased admission rate for alcoholic acute pancreatitis during the Christmas and New Year period, when there is a peak in the consumption of alcohol [11].
Although the association between alcohol and pancreatitis has been well documented, the precise magnitude of the impact of alcohol remains poorly quantified. At the individual level, the proportion of cases of pancreatitis attributed to alcohol varies widely among countries and range from 50 to 90% [8, 10]. With respect to population drinking and mortality from pancreatitis, the evidence is fairly limited. The only prior study applying the ARIMA time-series analysis found a positive relationship between alcohol consumption measured by alcohol sales and pancreatitis mortality in 14 western European countries [6]. According the poled estimates for northern, midand southern Europe, the strongest effect was found in northern Europe. The results from this study suggest that an increase in per capita alcohol consumption of 1 litre is followed by an increase in pancreatitis mortality of 5-15% in most countries, but by a 30-40% in Sweden and Norway. In most countries, the proportions of alcohol- attributable mortality from pancreatitis fall within the range between 40 and 80% [6]. It appears that the effect of alcohol on pancreatitis mortality rate was stronger in the northern European spirits countries characterized by a binge drinking pattern, than in the southern European wine countries with a high average consumption, which is more evenly distributed throughout the week.
In Russia, rates of alcohol consumption and pancreatitis mortality are among the highest in the world [16-19]. The distinctive trait of Russian drinking culture is a high overall level of alcohol consumption and the heavy episodic (binge) drinking pattern of strong spirits [20-22]. This is a good reason to expect positive association between alcohol consumption and pancreatitis mortality at the aggregate level in Russia. In present study we will test the hypothesis of the close aggregate level link between alcohol and pancreatitis mortality in Russia using data on overall alcohol consumption and sex-specific pancreatitis mortality rate between 1970 and 2005.
METHODS
Data
The data on age-adjusted sex-specific pancreatitis mortality rates per 1 000 000 of the population are taken from the Russian State Statistical Committee (Rosstat). The Rosstat's cause of death classification has undergone several changes in recent decades. Until 1988 the cause of death classification was based upon the Soviet nomenclature which had a limited number of causes of death in comparison with the International Classification of Diseases (ICD) system. From 1989-1998 Rosstat used a coding scheme that was based on ICD-9. From 1999 a new coding system based on ICD-10 was introduced. Rosstat issued a table of correspondence between its classification system and ICD-9 and ICD-10 and it has been claimed that the Russian system of coding is compatible with ICD codes [23]. Thus, Rosstat’s codes corresponds with ICD-9 codes 577.0 (acute pancreatitis) and 577.1 (chronic pancreatitis) and with ICD-10 codes K 85 (acute pancreatitis) and K 86.0/86.1 (chronic pancreatitis). Furthermore, a group of researchers has gained access to the Soviet mortality data and has been able to recalculate the Russian data according to the detailed list of ICD-9 codes [24]. These reclassified data have been used in the present study.
Realizing the difficulties associated with measuring alcohol consumption at the population level in Russia, we employed an alternative measure of overall alcohol consumption relative to Nemtsov’s estimates [16]. Estimation of alcohol consumption per capita was based on a set of indicator of alcohol-related harm which was adjusted for the effect of recorded alcohol consumption employing ARIMA (autoregressive integrated moving average) model [25]. More specifically, we calculated the level of unrecorded alcohol consumption as the difference between observed changes in the harm indicator and changes that would be expected on the bases of alcohol sales. The harm indicator series used was alcohol psychoses incidence rate because this indicator depends almost entirely on alcohol consumption [26]. We specified the number of persons, witches were admitted for the first time for the treatment as incidence of alcohol psychoses: (ICD-10: F 10). The data on alcohol psychoses incidence rate (per 100.000 of the population) are taken from the Russian State Statistical Committee (Rosstat). The alcohol series used was the volume of alcohol sales in liters of pure alcohol per capita.
STATISTICS
To examine the relation between changes in the alcohol consumption and pancreatitis mortality across the study period a time-series analysis was performed using the statistical package "Statistica". The dependent variables were the annual pancreatitis mortality and the independent variable was aggregate overall alcohol consumption. Bivariate correlations between the raw data from two time-series can often be spurious due to common sources in the trends and due to autocorrelation [27]. One way to reduce the risk of obtaining a spurious relation between two variables that have common trends is to remove these trends by means of a ‘differencing’ procedure, as expressed in formula:
∇xt = xt - xt-1
This means that the annual changes ‘∇’ in variable ‘X’ are analyzed rather than raw data. The process whereby systematic variation within a time series is eliminated before the examination of potential causal relationships is referred to as ‘prewhitening’. This is subsequently followed an inspection of the cross-correlation function in order to estimate the association between the two prewhitened time series. It was Box and Jenkins [28] who first proposed this particular method for undertaking a time series analysis and it is commonly referred to as ARIMA modeling. We used this model specification to estimate the relationship between the time series pancreatitis mortality and alcohol consumption rates in this paper. In line with previous aggregate studies [27, 29, 30] we estimated semi-logarithmic models with logged output. The following model was estimated:
∇LnM = a + β∇A + ∇Nt
where ∇ means that the series is differenced, M is pancreatitis mortality rates, a indicates the possible trend in pancreatitis mortality due to other factors than those included in the model, A is the alcohol consumption, β is the estimated regression parameter, and N is the noise term. The percentage increase in pancreatitis mortality rate rates associated with a 1-litre increase in alcohol consumption is given by the expression: (exp(β1)-1)*100. The temporal structure of the error term was estimated by using autoregressive (AR) or moving average (MA) parameters in the model. A diagnostic test for residual correlation is given by the Box-Ljung Q-test, which indicates whether the model has been adequately fitted.
A change in aggregate level drinking is expected to have an immediate effect on acute forms of alcohol-related problems (such as fatal alcohol poisoning), as well as a long-term effect on chronic problems (liver cirrhosis) [31]. As pancreatitis is attributed to the chronic rather from acute alcohol-related problems, we should expect that the pancreatitis mortality response to changes in aggregate level alcohol consumption will be distributed over several years [27]. In order to deal with the time-lag problem we inspected the cross-correlations between two time series at different lags.
In addition to the estimated effect parameter, the alcohol effect will also be expressed in terms of alcohol-attributable fraction (AAF), which can be calculated from the estimates obtained in ARIMA models according to following formula: AAF = 1-exp(-bX), where X is alcohol consumption for the whole study period and b is the estimated effect parameter [32] .
RESULTS
According to official statistics, the male pancreatitis mortality rate increased 5.6 times (from 21.4 to 120.1 per 1,000,000 of population) and female mortality rate increased 3.8 times (from 11.2 to 42.9 per 1,000,000 of population) in Russia from 1970 to 2005. Across the whole period the male pancreatitis mortality rate was 2.2 times higher than the female rate (56.3 vs. 25.6 per 1 000 000) with a rate ratio of 1.9 in 1970 increasing to 2.8 by the 2005. The trends in the age-adjusted, sex-specific pancreatitis mortality rates are displayed in Figures 1 and 2. For both sexes the time series pancreatitis mortality rates fluctuated greatly over the period: decreased markedly between 1984 and 1988, than started on an upward trend from 1988 to 1989, before increasing substantially during 1992 to 1994 (by 72.3% and 29.6% for men and women, respectively). From 1995 to 1998 there was a fall in the rates before they again jumping dramatically between 1998 and 2005 (by 84.3% and 46.4% for men and women respectively). Although the trends in pancreatitis mortality rates are rather similar over time series for both sexes, the male pancreatitis mortality rate tends to fluctuated across time series to a much greater extent than the female rate.
Figure 1. Trends in male pancreatitis mortality rate and alcohol consumption per capita in Russia between 1970 and 2005. We reported 1,000,000 in the
right y-axis too.
Figure 2. Trends in female pancreatitis mortality rate and alcohol consumption per capita in Russia between 1970 and 2005.
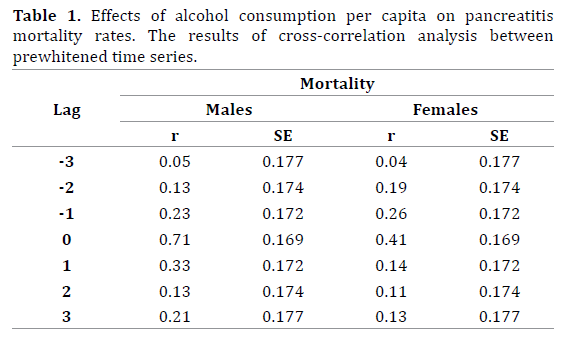
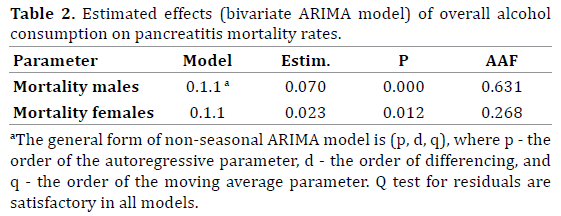
The graphical evidence suggests that the trends in both alcohol consumption per capita and pancreatitis mortality for males and females seem to follow each other across the time-series (Figures 1 and 2). As can be seen, there were sharp trends in the time series data across the study period. These trends were removed by means of a firstorder differencing procedure. After prewhitening the cross-correlations between alcohol consumption and the pancreatitis mortality time series were inspected. This indicated that there was a statistically significant crosscorrelation between alcohol consumption and pancreatitis mortality for males and females at lag zero (Table 1). The specification of the bivariate ARIMA model and outcome of the analyses are presented in Table 2. According to the results, alcohol consumption is a statistically significant associated with both male and female pancreatitis mortality rates, implying that a 1-litre increase in per capita consumption is associated with an increase in male mortality of 7.0% and female mortality of 2.3%. Table 2 also shows the relative proportion of alcohol-attributable deaths to all pancreatitis deaths by gender. The results of the analysis suggest that 63.1% of all male deaths and 26.8% female deaths from pancreatitis in Russia could be attributed to alcohol.
DISCUSSION
According to the results of time-series analysis there was a positive and statistically significant effect of per capita alcohol consumption on pancreatitis mortality in Russia at lag zero. These findings clearly indicate that population drinking and pancreatitis mortality are positively related phenomena in Russia. The results of present study are important because despite the growing literature on alcohol and mortality in Russia there has been no prior time-series analysis of alcohol and pancreatitis mortality in the country. The positive and significant contemporaneous association between alcohol and pancreatitis mortality in present analysis replicates the recent findings from a time-series studies highlighted close temporal association between alcohol and ischemic heart disease mortality in Russia [30].
It should be emphasis that the results suggest a fairly quick response of pancreatitis mortality rates to changes in population drinking. The instantaneous response in mortality rates from chronic alcohol-related diseases seem quite surprising when considering the long latency period at the individual level. There are several reasonable explanations for this seeming inconsistency. It is well recognized, that pancreatitis mortality is the classical indicator of harmful effect of chronic heavy drinking (chronic pancreatitis) and also associated with episodic heavy drinking (acute pancreatitis), thus reflecting the acute and chronic consequences of heavy drinking [8]. Therefore, the contemporaneous association between the two variables may support the point that binge drinking is an important determinant of pancreatitis mortality in Russia. Further, Norström and Skog [27] argue that in a population there exists a reservoir of heavy drinkers who are near the critical threshold-value for a dying from chronic alcohol-related consequences. In case when these high risk individuals increase alcohol consumption during a given year, they will exceed the threshold value and die from alcohol-related diseases. This is the reason why the immediate impact on chronic alcohol related mortality can be registered from marked changes in aggregate consumption.
It is important to point out, that the size of the bivariate association between alcohol and pancreatitis mortality for men is substantially greater than for women. The harmful drinking might be responsible for the gender differences in alcohol attributable deaths. The population surveys from Russia show consistently higher rates of binge drinking among men than women. Indeed, the results of study carried out in Archangelsk suggest that 61.9% of male and 25.7% of female industrial workers had a consumption pattern that was hazardous according to the AUDIT definition [33].
Understanding the reasons the substantial fluctuations in pancreatitis mortality rate in Russia over recent decades is very important from a public health perspective. There is evidence that the pancreatitis mortality trends in Russia influenced by the three major factors: Gorbachev’s antialcohol campaign 1985-88; severe socioeconomic crisis imposed by rapid societal transformation in the early 1990s; financial crisis and worsening economic situation in 1998. A fairly close match between trends in alcohol consumption and pancreatitis mortality during the Gorbachev’s anti-alcohol campaigns may be use as evidence for the hypothesis suggesting that alcohol is responsible for a substantial number of pancreatitis deaths in Russia. This empirical evidence also indicates that a restrictive alcohol policy can be considered as an effective measure of pancreatitis mortality prevention.
It seems plausible that alcohol is a key variable in explaining the increase in the pancreatitis mortality rate in the early-1990s. An increase of alcohol consumption in this period was to a great extent due to increase of alcohol availability following the repeal of the state alcohol monopoly in January 1992 [18]. There are several potential factors behind the decrease in alcohol consumption and pancreatitis mortality rate between 1994 and 1998. They include better regulation of the alcohol market that may have resulted in a relative increase in prices for vodka compared to those for food products [16]. Another possible factor in the decrease in alcohol consumption was impoverishment and decrease in the purchasing capacity of the population due to unpaid or delayed salaries [17]. The subsequent rise in alcohol consumption and pancreatitis mortality rates from 1998 may be associated with the financial crisis which resulted in hyperinflation, increasing poverty, political and economic uncertainty [34].
Before concluding, several potential limitations of this study must be mentioned. In particular, there was the risk of omitted variable bias in this work. It should be acknowledged that other risk factors such as diet and smoking also affect the mortality rate from pancreatitis [9]. However, there is no compelling epidemiological evidence of rapid changes in the dietary and smoking patterns among Russian men and women that could have translated into substantial fluctuations in pancreatitis mortality rate in the last decades. Therefore, the controlling for the impact of these risk factors would not have modified our results.
Finally, estimating unrecorded consumption of alcohol in Russia is a challenge, because of the diversity of this fraction of alcohol consumption that ranges from “moonshine” (i.e., самогон - “samogon” - in Russian) through legal non-beverage alcohol (medical tincture) to counterfeit vodka produced from technical spirits [22]. We relied on estimated overall level of alcohol consumption across the period. However, the accuracy of assessment of actual alcohol consumption using indirect methods depends significantly on whether the level of alcohol consumption is the only factor influencing the index chosen as the indicator of alcohol-related problems. This represents an essential drawback of such methods, because many other factors influence the level of alcohol-related problems [35].
CONCLUSION
In conclusion, this is the first time-series analysis of overall level of alcohol consumption and pancreatitis mortality rate in Russia, which has shown that population drinking, is the strong predictor of pancreatitis mortality rate at the aggregate level. The outcomes of this study provide indirect support for the hypothesis that unfavorable mixture of higher overall level of alcohol consumption and binge drinking pattern is a major risk factor for pancreatitis mortality in Russia. The findings from the present study have important implications as regards alcohol-related mortality prevention indicating that a restrictive alcohol policy can be considered as an effective measure of prevention in countries where higher rate of alcohol consumption per capita.
Acknowledgements
The author would like to thank the anonymous reviewers for their valuable comments and suggestions on an earlier version of this paper.
Conflicts of Interest
Authors declare to have no conflict of interest.
References
- Banks PA. Epidemiology, natural history, and predictors of disease outcome in acute and chronic pancreatitis. GastrointEndosc. 2002; 56: 226-230. [PMID:12447272]
- Yadav D. Recent advances in the epidemiology of alcoholic pancreatitis. CurrGastroenterol Rep. 2011; 13: 157-65. [PMID:21243451]
- Yadav D, Lowenfels AB. Trends in the epidemiology of the first attack of acute pancreatitis: a systematic review. Pancreas 2006; 33: 323-30. [PMID:17079934]
- Roberts SE, Williams JG, Meddings D, Goldacre MJ. Incidence and case fatality for acute pancreatitis in England: geographical variation, social deprivation, alcohol consumption and etiology-a record linkage study. Aliment PharmacolTher. 2008; 28: 931-41. [PMID:18647283]
- Sand J, Välikoski A, Nordback I. Alcohol consumption in the country and hospitalizations for acute alcohol pancreatitis and liver cirrhosis during a 20-year period. Alcohol Alcohol 2009; 44: 321-25. [PMID:19144980]
- Ramstedt M. Alcohol and pancreatitis mortality at the population level: experiences from 14 western countries. Addiction 2004; 99(10): 1255-1261. [PMID:15369563]
- Friedreich N. Diseases of the pancreas. In: Cyclopedia of the Practice of Medicine. Ed. H. Ziemssen. London: Sampson Low. 1878; 8: 551.
- Herreson-Villanueva M, Hijona E, Banales JH, Cosme A, Bujanda L. Alcohol consumption on pancreatic diseases. World J Gastroenterol. 2013; 19: 638-647. [PMID:23429423]
- Cote GA, Yadav D, Slivka A, Anderson MA, Burton FR, Burton FR, et al. Alcohol and smoking as risk factors in an epidemiology study of patients with chronic pancreatitis. ClinGastroenterolHepatol. 2011; 9: 266-273. [PMID:21029787]
- Gullo L. Alcohol and chronic pancreatitis: leading or secondary etiopathogenic role? JOP. 2005; 6: 68-72. [PMID:15650289]
- Roberts SE, Akbari A, Thorne K, Atkinson M, Evans PA. The incidence of acute pancreatitis: impact of social deprivation, alcohol consumption, seasonal and demographic factors. Aliment PharmacolTher. 2013; DOI: 10.1111/apt. 12408. [PMID:23859492]
- Pelli H, Lappalainen-Lehto R, Piironen A, Sand J, Nordback I. Risk factors for recurrent acute alcohol-associated pancreatitis: a prospective analysis. Scand J Gastroenterol. 2008; 43: 614-21. [PMID:18415757]
- Kristiansen L, Grønbæk M, Becker U, Tolstrup JS. Risk of Pancreatitis According to Alcohol Drinking Habits: A Population-based Cohort Study. Am J Epidemiol 2008; 168: 932-937. [PMID:18779386]
- Irving HM, Samokhvalov AV, Rehm J. Alcohol as a risk factor for pancreatitis: a systematic review and meta-analysis. JOP. 2012; 10(4): 387-392. [PMID:19581740]
- Azodi OS, Orsini N, Andrén-Sandberg A. Effect of type of alcoholic beverage in causing acute pancreatitis. Brit J Surg. 2011; 98: 1609-1616. [PMID:21811997]
- Nemtsov AV. Estimates of total alcohol consumption in Russia, 1980- 1994. Drug Alcohol Depend. 2000; 58: 133-142. [PMID:10669064]
- Nemtsov AV, Davydov KE, Razvodovsky YE. Comparative analysis of the alcohol situation in Belarus and Russia. Narcologia 2009; 1: 52-60.
- Nemtsov AV, Razvodovsky YE. Alcohol situation in Russia, 1980-2005. Social and Clinical Psychiatry 2008; 2: 52-60.
- Khoziainov YA. The prevalence of digestive organ diseases and the organization of specialized care. Problems of Social Gygiene and Hystory of Medicine. 1997; 2: 9-11. [PMID:9254198]
- Leon D, Saburova L, Tomkins S, Andreev E, Kiryanov N, McKee M, &Shkolnikov V. Hazardous alcohol drinking and premature mortality in Russia: a population based case-control study. Lancet. 2007; 369: 2001- 2009. [PMID:17574092]
- Stickley A, Leinsalu M, Andreew E, Razvodovsky YE, Vagero D, McKee M. Alcohol poisoning in Russia and the countries in the European part of the former Soviet Union, 1970-2002. Eur J Pub Health. 2007; 17: 444-449. [PMID:17327281]
- Stickley A, Razvodovsky Y & McKee M. Alcohol and mortality in Russia: A historical perspective. Public Health. 2009; 123: 20-26. [PMID:19084882]
- Wasserman D, Varnik A. Reliability of statistics on violent death and suicide in the former USSR, 1970-1990. ActaPsychiatrScand Suppl. 1998; 394: 34-41. [PMID:9825016]
- Mesle F, Vallin J. Reconstruction long-term series of causes of death. Historical Methods 1996; 29: 72-87.
- Razvodovsky YE. Estimation of the level of alcohol consumption in Russia. ICAP Periodic Review on Drinking and Culture. Issue 8. 2013: 7-10.
- Babor TF, Caetano R, Casswell S, Edwards G, Giesbrecht N, Graham K, et al. Alcohol: No Ordinary Commodity: Research and Public Policy. London: Oxford University Press, 2010.
- Norström T, Skog OJ. Alcohol and mortality: methodological and analytical issue in aggregate analysis. Addiction 2001; 96: 5-17. [PMID:11228078]
- Box GEP, Jenkins GM. Time Series Analysis: forecasting and control. London: Holden-Day Inc. 1976.
- Razvodovsky YE. Estimation of alcohol attributable fraction of mortality in Russia. Adicciones 2012; 24(3): 1-7. [PMID:22868980]
- Razvodovsky YE. Alcohol-attributable fraction of ischemic heart disease mortality in Russia. ISRN Cardiol. 15; 2013:287869. [PMID:23956877]
- Norström T, Ramstedt M. Mortality and population drinking: a review of the literature. Drug Alcohol Rev. 2005; 24: 537-547. [PMID:16361210]
- Norström T. The use of aggregate data in alcohol epidemiology. Brit J Addict. 1989; 84: 969-977. [PMID:2624626]
- Nilssen O, Averina M, Brenn T, Drox J, Kalinin A, &Archipovski V. Alcohol consumption and its relation to risk factors for cardiovascular disease in the north-west of Russia: the Archangelsk study. Int J Epidemiol. 2005; 34: 781-788. [PMID:15833789]
- Cockerham WC, Hinote BP, Abbott P. Psychological distress, gender, and health lifestyles in Belarus, Kazakhstan, Russia, and Ukraine. SocSci Med. 2006; 63: 2381-2394. [PMID:16887246]
- Razvodovsky YE. Unrecorded alcohol consumption: quantitative methods of estimation. Alcoholism 2010; 46(1): 15-24.



