Keywords
Amino Acids; Diabetes Mellitus; Pancreatic Elastase; Pancreatitis, Chronic
Abbreviations
PITC: phenyl isothiocyanate
INTRODUCTION
Protein energy malnutrition has been reported in chronic pancreatitis [1]. Malabsorption and systemic inflammation have been the mechanisms postulated. Conversely, protein malnutrition can influence pancreatic enzymatic secretion [2]. Alcohol abuse has profound adverse effects on protein status; the etiopathogenesis of tropical pancreatitis has been attributed to protein malnutrition [3].
Protein-energy malnutrition could affect pancreatic function and structure. Previous reports have documented reduction in zymogen granules [4] and pancreatic head size [5] as well as the development of pancreatic fibrosis [6] in patients with protein energy malnutrition. Sandhyamani et al. [7] reported that feeding protein-deficient and carbohydrate-rich meals could induce pancreatic damage in experimental bonnet monkeys. Histological findings of the pancreas in these animals were similar to changes in tropical chronic pancreatitis.
However, there is a lack of literature on amino acid status in chronic pancreatitis. A recent paper [8] reported the changes in plasma amino acid levels in a small series of chronic pancreatitis and pancreatic cancer patients. These authors explained that the changes observed might presumably be due to intestinal malabsorption and systemic inflammation. The profile of individual amino acids in chronic pancreatitis has also not received as much attention as in other diseases where elevated amino acids and their products (e.g. ammonia, homocysteine) have been implicated in the pathogenesis.
We estimated the plasma free amino acid profile in patients with chronic pancreatitis and compared it to the healthy controls. An attempt was made to identify any particular limiting amino acid(s) or amino acid subgroup(s).
METHODS
A total of 175 consecutive adult patients with chronic pancreatitis were recruited for the study from the Pancreas Clinic of our hospital. Diagnosis was based on pancreatic calcification and/or parenchymal or ductal changes on imaging (US/CT). Chronic pancreatitis patients included 84 patients with alcoholic chronic pancreatitis and 91 with tropical chronic pancreatitis. Patients having chronic pancreatitis with alcohol consumption equal to, or greater than, 80 g/day for at least 5 years were considered to have alcoholic chronic pancreatitis while tropical chronic pancreatitis was defined using previously reported criteria [9]. Patients with pancreatic cancer, those who had undergone pancreatic surgery and those with complications, such as a pseudocyst or common bile duct obstruction, and those consuming protein supplements were excluded. Furthermore, 113 apparently healthy adult hospital visitors were recruited as controls.
History of illness, including presenting complaints, duration of illness, pain and diabetes mellitus and risk factors, such as alcohol and smoking, were recorded. Demographic parameters and anthropometric measurements were elicited and a detailed physical examination was carried out. BMI was calculated by the formula weight/height2 (kg/m2). A detailed dietary history was recorded.
Characteristics of Study Subjects
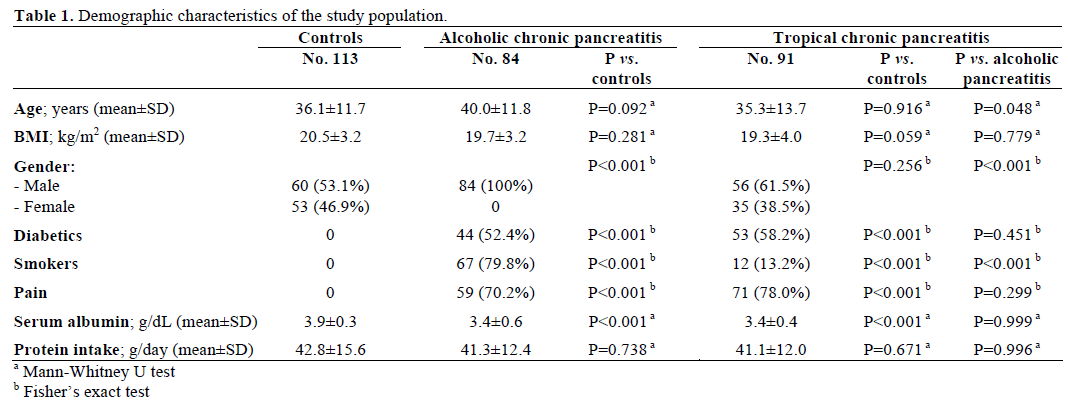
The demographic characteristics of the study population are given in Table 1. Of the 175 patients, there were 84 patietns with alcoholic chronic pancreatitis and 91 with tropical chronic pancreatitis. The mean age of the chronic pancreatitis patients was comparable with the age of controls; however, the mean age of tropical chronic patients was significantly lower than those with alcoholic chronic pancreatitis. The mean body mass index (BMI) was comparable in all three groups. Alcoholic and tropical chronic pancreatitis patients had significantly lower serum albumin levels as compared to the controls. The protein intake in alcoholic and tropical chronic pancreatitis patients and controls was comparable; however, the protein intake of the patients and controls was less than the recommended daily allowance in this population.
Plasma Amino Acid Levels
Seventeen amino acids were estimated in all the chronic pancreatitis patients and controls. The results were expressed as mean±SEM (μmol/L). Overnight fasting venous blood was collected in EDTA vials and centrifuged immediately at 1,500 g for 15 min at 4°C. The plasma was separated and stored at -20°C and a biochemical assay was performed within 2 weeks. Plasma amino acids were derivatized with phenyl isothiocyanate (PITC), and separated and quantified by reverse-phase high-pressure liquid chromatography (HPLC) using EconosphereTM column (Alltech, Deerfield, IL, USA; 150x4.6 mm, internal diameter 3 μm) [10]. One hundred microliters of plasma were mixed with 100 μL of internal standard (norleucine) and centrifuged. Coupling buffer (methanol/water/ triethylamine, 2:1:1) and PITC derivatization solution (ethanol/water/triethylamine/PITC, 7:1:1:1) were applied and vacuum dried. Finally, the residue was mixed with 500 μL of sodium acetate-acetonitrile buffer, and 20 μL were injected into HPLC.
No significant differences in plasma amino-acid concentrations were observed in repeat samples obtained from any given patient. The overall reproducibility of the results was consistent within ±5%.
The following subgroups were calculated:
1. essential amino acids: total plasma concentrations of phenylalanine, valine, threonine, isoleucine, methionine, histidine, leucine and lysine were estimated and included as essential amino acids;
2. non-essential amino acids: total amino acid concentrations of aspartate, glutamate, serine, glycine, arginine, alanine, proline, tyrosine and cystine were estimated and included as non-essential amino acids;
3. the branched chain amino acid (BCAA) to aromatic amino acid (AAA) ratio (Fischer ratio) was calculated using the formula: Fisher ratio = (leucine + isoleucine + valine) / (phenylalanine + tyrosine);
4. phenylalanine:tyrosine ratio (indicator of catabolic state) [11];
5. glycine:BCAA ratio (indicator of protein intake) [11];
6. glycine:valine ratio (index of protein malnutrition) [11].
Biochemical Evaluations
Stool samples were collected from chronic pancreatitis patients and stored at -4°C. Pancreatic fecal elastase-1 was measured using a polyclonal antibody-based ELISA kit (Bioserv, Rostock, Germany) as a measurement of pancreatic exocrine insufficiency; fecal elastase-1 ranging 100-200 μg/g stool was considered as moderate while fecal elastase-1 less than 100 μg/g stool was considered as severe exocrine insufficiency.
Plasma total protein [12], albumin [13] and blood hemoglobin [14] concentrations were also estimated using spectrophotometry.
Serum fasting and postprandial glucose levels were recorded to estimate endocrine insufficiency (fasting blood glucose level >110 mg/dL and random blood glucose level >200 mg/dL on more than one occasion). Insulin requirement was used for assessment of the severity of diabetes.
ETHICS
Institutional ethics committee clearance was obtained. Written informed consent was taken from all subjects who participated in the study. The study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004. The study was approved by the ethical review committee of our institution.
STATISTICS
Statistical analysis was conducted by using SPSS, version 11 (SPSS Inc, Rostock, IL, USA). The Mann- Whitney U test was used to compare continuous data between two groups. The Spearman correlation was used for bivariate correlations and the Fisher’s exact test was used in order to analyze 2x2 tables. Multivariate logistic regression analysis was performed to identify amino acids independently associated with diabetes and low elastase-1. Plasma amino acid levels were reported as mean±SE.
RESULTS
Plasma Amino Acid Levels
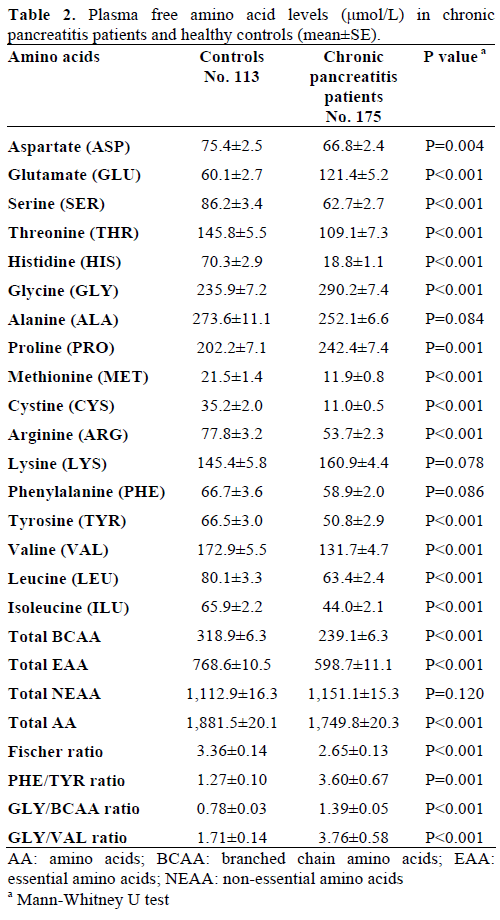
In all, 17 amino acids were detected and identified. The distribution pattern of these amino acids is given in Table 2. As compared to the healthy controls, the chronic pancreatitis patients had lower concentrations of aspartate, serine, histidine, arginine, threonine, tyrosine, valine, methionine, cystine, isoleucine and leucine while alanine and phenylalanine did not reach statistical significance. Plasma glutamate, glycine, and proline were significantly increased while lysine did not reach statistical significance. Asignificant positive correlation was obtained between serum albumin and the essential amino acid levels (rs=0.312; P<0.001) as well as with the total amino acid level (rs=0.412; P<0.001).
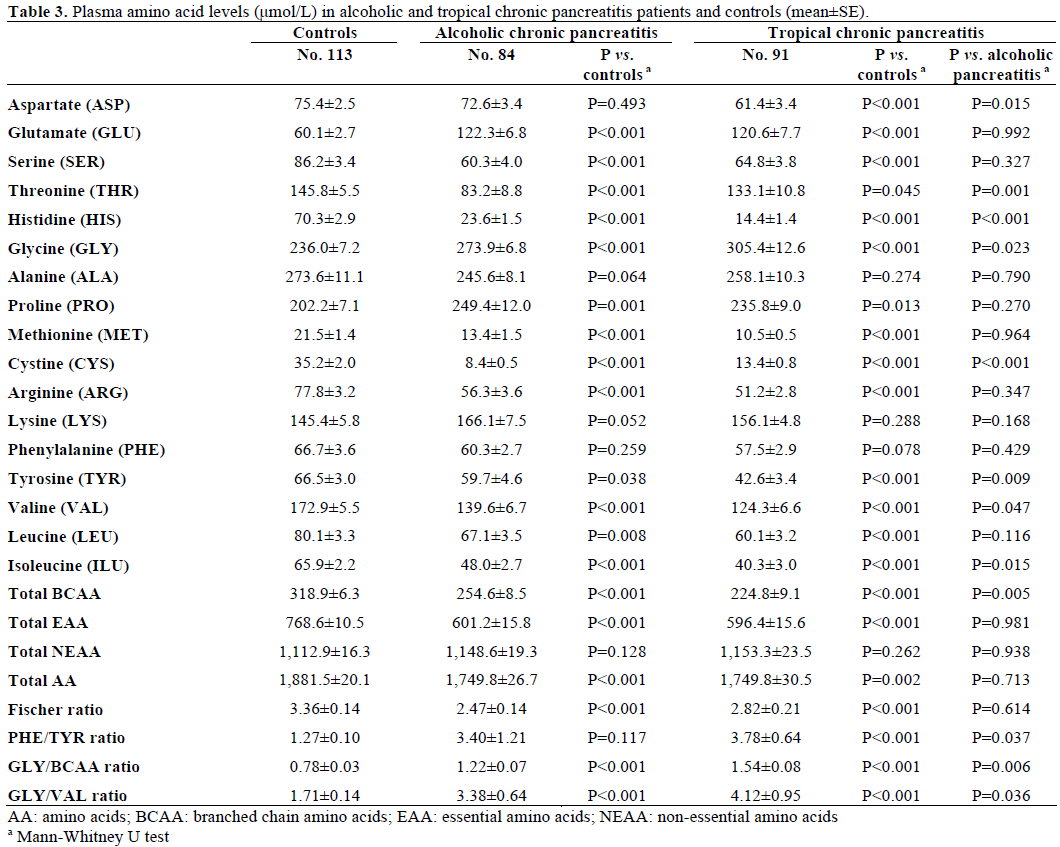
The plasma free amino acid levels in alcoholic chronic pancreatitis patients and tropical chronic pancreatitis patients are shown in Table 3. In alcoholic chronic pancreatitispatients, as well as in tropical chronic pancreatitis patients, the plasma levels of serine, threonine, histidine, arginine, tyrosine, valine, methionine, cystine, isoleucine, and leucine were significantly decreased while the levels of glutamate, glycine, and proline were elevated in comparison to the control patients. Aspartate was significantly decreased vs. control subjects in tropical chronic pancreatitis patients only. Aspartate, histidine, tyrosine, valine and isoleucine were significantly decreased in tropical chronic pancreatitis patients while threonine, glycine, and cystine were significantly elevated when compared to alcoholic chronic pancreatitis patients. A significant decrease in total branched chain amino acid levels was found in tropical chronic pancreatitis as compared to alcoholic chronic pancreatitis patients.
Plasma concentrations of aspartate, phenylalanine, valine and leucine were significantly lower in diabetics as compared to non-diabetic chronic pancreatitis patients (Table 4).
Plasma Molar Amino Acid Ratios
Mean Fisher ratio was significantly lower both in alcoholic and tropical chronic pancreatitis patients (Table 3) when compared to the controls (P<0.001).
The phenylalanine to tyrosine ratio, an indicator of catabolic state, was significantly elevated in overall chronic pancreatitis patients (Table 2), tropical chronic pancreatitis patients (Table 3) and both diabetic and non-diabetic chronic pancreatitis patients (Table 4) when compared to the controls.

The glycine to total branched chain amino acid ratio, an indicator of reduced protein intake, was significantly elevated in overall chronic pancreatitis patients (Table 2), alcoholic and tropical chronic pancreatitis patients (Table 3), as well as in diabetic and non-diabetic chronic pancreatitis patients (Table 4) in comparison with the controls. In addition, the glycine to branched chain amino acid ratio was significantly elevated in tropical chronic pancreatitis patients when compared to alcoholic chronic pancreatitis patients (Table 3) as well as in diabetic vs. non-diabetic chronic pancreatitis patients (Table4).
The glycine to valine ratio, an indicator of protein malnutrition, was significantly increased in overall chronic pancreatitis patients (Table 2), both alcoholic and tropical chronic pancreatitis patients (Table 3), and diabetic and non-diabetic (Table 4) chronic pancreatitis patients in comparison with the controls. In addition, tropical chronic pancreatitis patients had a significant increase in the glycine to valine ratio when compared to alcoholic chronic pancreatitis patients (Table 3) as did diabetic vs. non diabetic patients (Table 4).
Plasma Amino Acids and Pancreatic Stool Elastase-1
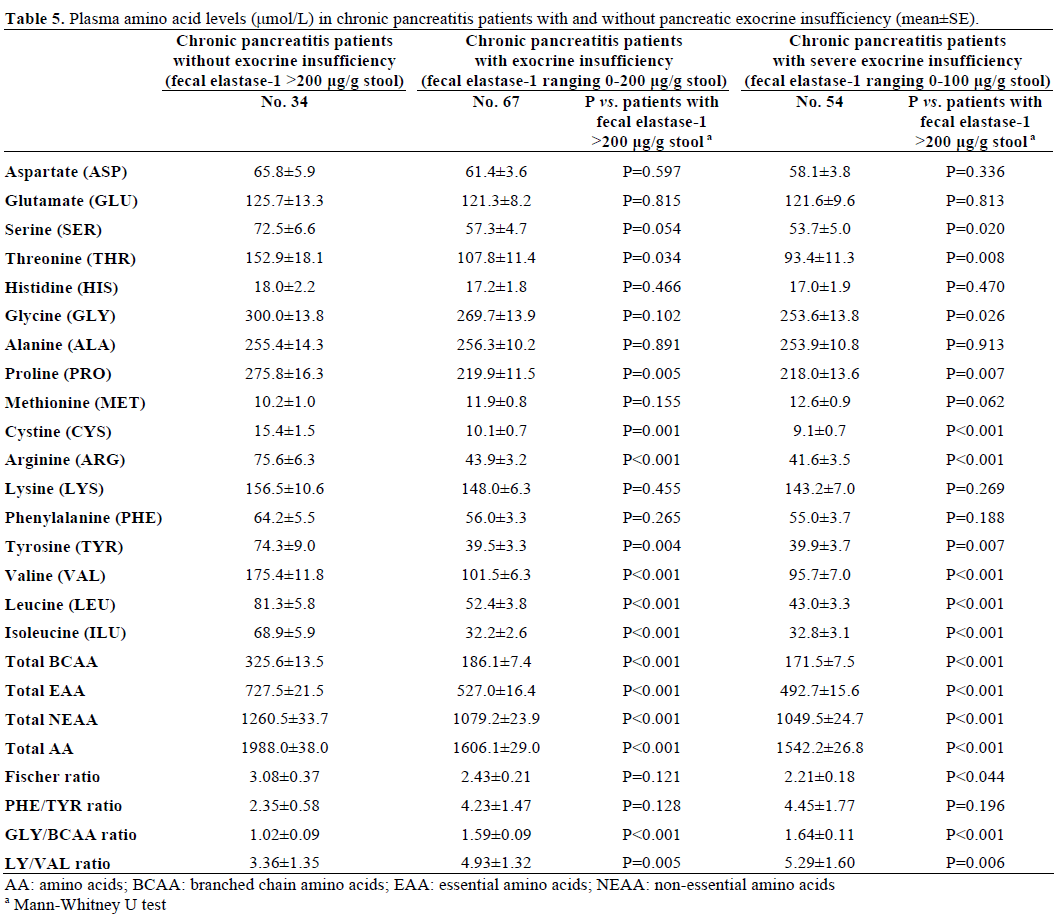
Pancreatic stool elastase-1 was measured in 101 consecutive chronic pancreatitis patients. Elastase-1 was low (0-200 μg/g stool) in 67 (66.3%) chronic pancreatitis patients. Among these, moderate (100-200 μg/g stool) and severe (less than 100 μg/g stool) insufficiency was seen in 13 (12.9%) and 54 (53.5%) patients, respectively. A significant decrease in arginine, threonine, proline, tyrosine, cystine, isoleucine, valine and leucine levels was noted in chronic pancreatitis patients with low fecal elastase-1 (0-200 μg/g stool) when compared to chronic pancreatitis patients with normal fecal elastase-1 level (>200 μg/g stool) (Table 5). In patients with severe exocrine insufficiency (fecal elastase-1 less than 100 μg/g stool), plasma levels of serine, glycine, arginine, threonine, proline, tyrosine, cystine, isoleucine, leucine, and valine were significantly decreased when compared to patients who had pancreatic fecal elastase- 1 >200 μg/g stool (Table 5).
Total branched chain amino acids showed significant positive correlation with fecal elastase-1 (rs=0.724; P<0.001).
Association of Plasma Amino Acid Concentration with Diabetes and Low Elastase-1
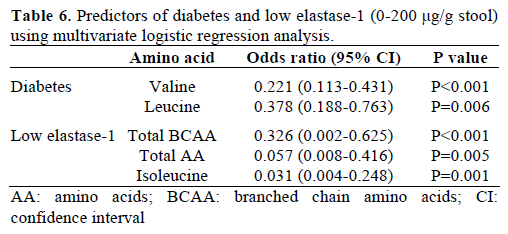
Stepwise multivariate logistic regression analysis was carried out to evaluate the possible association between different plasma amino acid levels and the presence of both diabetes mellitus and low elastase-1 (0-200 μg/g stool). Decreased valine and leucine levels were independent predictors of diabetes. Decreased total branched chain amino acids, total amino acids, and isoleucine were independent predictors of low stool elastase-1 (0-200 μg/g stool) (Table 6).
DISCUSSION
The pancreas is one of the organs with an extremely high protein turnover [15, 16]. Apart from being a constituent of proteins, amino acids have an important role in the physiological functioning of the pancreas [17]. Alterations in the amino acid metabolism in alcoholic chronic pancreatitis patients are probably related to chronic alcoholism since alcoholism is known to affect the normal absorption of amino acids [18]. Although, Zuidema [19] initially reported protein malnutrition in tropical chronic pancreatitis patients about four decades ago, there is limited literature on the role of any limiting amino acids, the effects of amino acid imbalance and the exact role of individual amino acids in the normal physiology and also pathological conditions of the pancreas.
In this study we found a significant decrease in the majority of amino acids in chronic pancreatitis patients. In addition, we observed a decrease in the levels of total essential amino acids in both alcoholic chronic pancreatitis and tropical chronic pancreatitis patients as compared to the controls. However, levels of essential amino acids were comparable among alcoholic chronic pancreatitis and tropical chronic pancreatitis patients. Adrych et al. [20] have recently reported that essential amino acids and aromatic amino acids were decreased in chronic pancreatitis patients, possibly due to decreased exocrine function. In our study, the majority of plasma amino acid levels were lower in chronic pancreatitis patients with pancreatic exocrine insufficiency as evidenced by low pancreatic stool elastase-1.
A key finding in this study was a significant decrease in total branched chain amino acid levels in tropical chronic pancreatitis compared to alcoholic chronic pancreatitis patients. Tissue utilization of branched chain amino acids is increased in the case of depressed ketogenesis [21]. It is worthwhile to note that tropical chronic pancreatitis is frequently associated with low ketosis [22]. Increased utilization of branched chain amino acids in tropical chronic pancreatitis patients due to the decreased availability of ketone bodies could possibly be one of the reasons for lower branched chain amino acid levels in tropical as compared to alcoholic chronic pancreatitis patients. Branched chain amino acids, especially leucine, have been found to have a stimulatory effect on protein assimilation in pancreatic acinar cells via an mTOR pathway [23]. Furthermore, branched chain amino acid transferase, an enzyme responsible for catabolism of branched chain amino acids, is strongly expressed in acinar cells of the exocrine pancreas. Sweatt et al. [24] argued that high concentrations of mitochondrial branched chain amino acid transferase in pancreatic acinar cells could be that of providing ketoisocaproate (transamination product of leucine) as a signaling molecule to the islet to stimulate insulin secretion. Although the importance of high branched chain amino acid transferase, especially in the exocrine pancreas, remains to be established, it seems likely that branched chain amino acids may play an important role in the normal functioning of pancreatic acinar cells.
Nakamura et al. [25] have reported that plasma amino acids in patients with pancreatic diabetes due to chronic pancreatitis were higher as compared to those with primary diabetes of similar glycemic control. Elevated levels of plasma amino acids were related to decreased tissue uptake of amino acids, lower levels of insulin as well as decreased gluconeogenensis due to low glucagon. In the current study, we observed decreased plasma levels of the majority of amino acids in diabetics with chronic pancreatitis as compared to healthy subjects. However, pancreatic diabetes is associated with a decreased risk of ketosis; insulin resistance is also usually not a feature. It is possible that exocrine insufficiency may impact amino acid levels in a manner different from that of endocrine insufficiency.
We have observed significant reduction in plasma sulphur containing amino acids, such as methionine and cystine, in our patients with chronic pancreatitis. Studies by Veghelyi et al. [26] have demonstrated atrophic changes in the pancreas in children which result from essential amino acid deficiency, including that of methionine. Depletion of S-adenosyl methionine (SAM) can cause development of pancreatitis in choline (methyl donor)-deficient, ethionine (antagonist of methionine)-supplemented young female mice. [27]. Methionine supplementation has been shown to prevent ethionine-induced pancreatitis in these experimental animals [28]. Studies using an acinar cell differentiation model indicate that methionine is required for acinar cell survival, growth and differentiation [17]. In a recent study, our group has shown lower plasma methionine levels and hyperhomocystinemia in chronic pancreatitis especially in chronic pancreatitis patients with low red cell folate levels [29].
Sandstrom et al. [30] have reported alterations in the amino acid spectrum during the course of acute pancreatitis; this could have possible implications for inflammatory processes. Serial estimations of amino acid levels could be helpful in assessing their role during the disease course in chronic pancreatitis.
In conclusion, our findings indicate selective amino acid deficiency along with varying levels of deficiency in the amino acid subgroups which seems to correlate with exocrine and endocrine insufficiency in chronic pancreatitis. We also observed significant derangements in the levels of branched chain amino acids. Our preliminary findings require additional study to explore the mechanistic role of selective amino acid deficiency in chronic pancreatitis.
Acknowledgment
The authors thank the Kerala State Council for Science Technology and Environment, Government of Kerala, Kerala state, India, for the financial support
Conflict of interest
The authors have no potential conflict of interest
References
- Pitchumoni CS. Pancreas in primary malnutrition disorders. Am J ClinNutr 1973; 26:374-9. [PMID 4632067]
- De Kolster CC, Kolster JG, Rached I, Estopiñán M, Azuaje M, Bordones G, et al. Serum cationic trypsinogen: marker of exocrine pancreatic dysfunction in children with protein-calorie malnutrition. G E N 1991; 45:92-7. [PMID 1843944]
- Balakrishnan V. Tropical Pancreatitis - Epidemiology, Athogenesis and Etiology. In: Balakrishnan V, Ed. Chronic Pancreatitis in India. Indian Society of Pancreatology, Trivandrum 1987; 79-85.
- Davies JN. The essential pathology of kwashiorkor. Lancet 1948; 251:317-20. [PMID 18905394]
- El-Hodhod MA, Nassar MF, Hetta OA, Gomaa SM. Pancreatic size in protein energy malnutrition: a predictor of nutritional recovery. Eur J ClinNutr 2005; 59:467-73. [PMID 15536474]
- Brooks SE, Golden MH. The exocrine pancreas in kwashiorkor and marasmus. Light and electron microscopy. West Indian Med J 1992; 41:56-60. [PMID 1523833]
- Sandhyamani S, Vijayakumari A, Balaraman Nair M. Bonnet monkey model for pancreatic changes in induced malnutrition. Pancreas 1999; 18:84-95. [PMID 9888664]
- Schrader H, Menge BA, Belyaev O, Uhl W, Schmidt WE, Meier JJ. Amino acid malnutrition in patients with chronic pancreatitis and pancreatic carcinoma. Pancreas 2009; 38:416-21. [PMID 19169171]
- Balakrishnan V, Unnikrishnan AG, Thomas V, Choudhuri G, Veeraraju P, Singh SP, et al. Chronic pancreatitis. A prospective nationwide study of 1,086 subjects from India. JOP. J Pancreas (Online) 2008; 9:593-600. [PMID 18762690]
- Hariharan M, Naga S, VanNoord T. Systematic approach to the development of plasma amino acid analysis by high-performance liquid chromatography with ultraviolet detection with precolumnderivatization using phenyl isothiocyanate. J Chromatogr 1993; 621:15-22. [PMID 8308083]
- Moyano D, Vilaseca MA, Artuch R, Lambruschini N. Plasma amino acids in anorexia nervosa. Eur J ClinNutr 1998; 52:684-9. [PMID 9756126]
- Lowry OH, Rosenbrough NJ, Farr A. Randall RJ. Protein measurement with the Folin phenol reagent. J BiolChem 1951; 193:265-75. [PMID 14907713]
- Burtis CA, Ashwood ER, Tietz NW (eds). Tietz Text Book of Clinical Chemistry. 1st Ed. W.B. Saunders, 1986; 589. [ISBN 978- 0721656106]
- Drabkins DL, Austin JH. Spectrophotometric studies: spectrophotometric constants for common hae- moglobin derivatives in human, dog and rabbit blood. J BiolChem 1932; 98:719-33.
- Wheeler JE, Lukens FD, Gyorgy P. Studies on the localization of tagged methionine within the pancreas. ProcSocExpBiol Med 1949; 70:187-9. [PMID 18109763]
- Hansson E. The formation of pancreatic juice proteins studies with labelled amino acids. ActaPhysiolScandSuppl 1959; 46:1-99. [PMID 13649369]
- Parsa I, Marsh WH, Fitzgerald PJ. Pancreas acinar cell differentiation. 3. Importance of methionine in differentiation of pancreas anlage in organ culture. Am J Pathol 1970; 59:1-22. [PMID 5441717]
- Israel Y, Salazar I, Rosenmann E. Inhibitory effects of alcohol on intestinal amino acid transport in vivo and in vitro. J Nutr 1968; 96:499-504. [PMID 5699991]
- ZuidemaPJ. Cirrhosis and disseminated calcification of the pancreas in patients with malnutrition. Trop Geogr Med 1959; 11:70- 4. [PMID 13659585]
- Adrych K, Smoczynski M, Stojek M, Sledzinski T, Slominska E, Goyke E, et al. Decreased serum essential and aromatic amino acids in patients with chronic pancreatitis. World J Gastroenterol 2010; 16:4422-7. [PMID 20845509]
- DudrickSJ, Kavic SM. Hepatobiliary nutrition: history and future. J HepatobiliaryPancreatSurg 2002; 9:459-68. [PMID 12483268]
- Balakrishnan V, Lakshmi R, Nandakumar R. Tropical pancreatitis - What Is Happening to It? In: Balakrishnan V, Kumar H, Sudhindran S, et al, eds Chronic pancreatitis and pancreatic diabetes in India. Cochin: The Indian Pancreatitis Study Group, 2006:25–53.
- Sans MD, Tashiro M, Vogel NL, Kimball SR, D'Alecy LG, Williams JA. Leucine activates pancreatic translational machinery in rats and mice through mTOR independently of CCK and insulin. J Nutr 2006; 136:1792-9. [PMID 16772439]
- SweattAJ, Wood M, Suryawan A, Wallin R, Willingham MC, Hutson SM. Branched-chain amino acid catabolism: unique segregation of pathway enzymes in organ systems and peripheral nerves. Am J PhysiolEndocrinolMetab 2004; 286:E64-76. [PMID 12965870]
- Nakamura T, Takebe K, Kudoh K, Ishii M, Imamura K, Kikuchi H, et al. Increased plasma gluconeogenic and system A amino acids in patients with pancreatic diabetes due to chronic pancreatitis in comparison with primary diabetes. Tohoku J Exp Med 1994; 173:413-20. [PMID 7825175]
- Veghelyi PV, KemenyTT, Pozsonyi J, Sós J. Dietary lesions of the pancreas. Am J Dis Child 1950; 79:658-65.
- Gilliland L, Steer ML. Effects of ethionine on digestive enzyme synthesis and discharge by mouse pancreas. Am J Physiol 1980; 239:G418-26. [PMID 6159794]
- Farber E, Popper H. Production of acute pancreatitis with ethionine and its prevention by methionine. ProcSocExpBiol Med 1950; 74:838-40. [PMID 14781196]
- GirishBN, Vaidyanathan K, Rao NA, Rajesh G, Reshmi S, Balakrishnan V. Chronic pancreatitis is associated with hyperhomocysteinemia and derangements in transsulfuration and transmethylation pathways. Pancreas 2010; 39:e11-6. [PMID 20050230]
- Sandstrom P, Trulsson L, Gasslander T, Sundqvist T, von Dobeln U, Svanvik J. Serum amino acid profile in patients with acute pancreatitis. Amino Acids 2008; 35:225-31. [PMID 17520324]

