Keywords
Morbidity; Pancreas; Pancreatectomy
INTRODUCTION
Distal pancreatectomy is a technically complex procedure usually performed on an older population with significant comorbidities, with a perioperative mortality rate inferior to 5% in high volume centers [1], but with a high morbidity rate, ranging from 22.7% to 57% [2, 3]. How is it possible to justify this wide range? Are there really important differences between the different centers or does a common method for evaluating surgical outcome not exist? In fact, while mortality is an easily quantifiable outcome parameter, overall morbidity and its severity are only poorly defined and this has hampered comparison among the different centers and within the same institution over time. It should be pointed out that the definition and severity of the most common complications after pancreatic resection are widely accepted to be postoperative pancreatic fistula [4], postpancreatectomy hemorrhage [5] and delayed gastric emptying [6], but there is no internationally accepted grading system of all types of complications which allows a proper interpretation of the surgical outcome. In 1992, a novel approach was presented for ranking complications by severity based on the therapy used to treat the complications but it did not gain widespread acceptance [7]. The same authors revised this grading system in 2004, introducing a new five-scale classification system with the aim of presenting an objective, simple, reliable and reproducible way of reporting all complications after surgery [8]. From January 2004 to March 2009, Clavien et al. [9] reported 214 citations of this classification system, 49 of them from the hepato-pancreatico-biliary field. Nevertheless, to our knowledge, there is no study which has tested the Clavien-Dindo classification after distal pancreatectomy. Thus, the aim of our study was to test the usefulness of the Clavien-Dindo classification in patients undergoing distal pancreatectomy in clinical practice by considering the length of the hospital stay as the principal outcome indicator.
METHODS
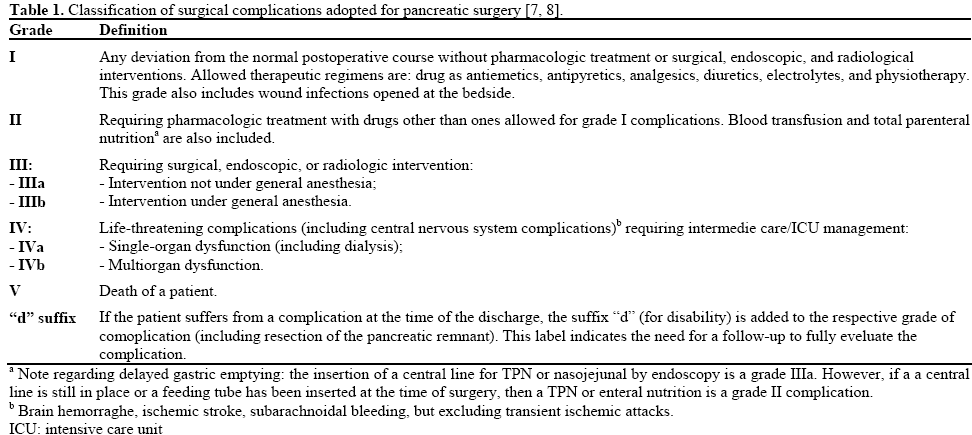
A prospective study of 61 consecutive patients who underwent distal pancreatectomy in the First Surgical Clinic of the University of Bologna, S.Orsola-Malpighi Hospital, from January 2006 to June 2010, was conducted. Demographic data (age and sex), preoperative factors (presence and number of comorbidities), operative parameters (type of distal pancreatectomy, treatment of the pancreatic stump, extension of resection), and pathological diagnosis (benign or malignant disease) were reported. The clinical course was documented for each patient and the complications were classified according to the criteria of Clavien and Dindo [7, 8] (Table 1).
Briefly, distal pancreatectomy was performed for pancreatic diseases of the body-tail, always with a standard lymphadenectomy, frequently with a splenectomy (44, 72.1%), rarely spleen-preserving (17, 27.9%). A left pancreatectomy consisted in a pancreatic resection to the left of the portal mesenteric vein; in a subtotal pancreatectomy, instead, the pancreatic resection was to the right of the portal mesenteric vein. Manual or stapler closure of the pancreatic stump was performed.
A postoperative pancreatic fistula was defined as a drain output of any measurable volume of fluid on or after the third postoperative day, with amylase content greater than three times the serum amylase activity. The grading system for a postoperative pancreatic fistula which was used in the present study was that proposed by the International Study Group of Pancreatic Fistula (ISGPF: grades A, B, and C) [4]. Postpancreatectomy hemorrhage was defined as intraabdominal or intestinal bleeding according to the criteria of the International Study Group of Pancreatic Surgery (ISGPS). The definition of postpancreatectomy hemorrhage is based on three parameters: onset (early: less than, or equal to, 24 hours; late: more than 24 hours), location (intraluminal or extraluminal) and severity (mild or severe). Three different grades of postpancreatectomy hemorrhage (grades A, B, and C) were recognized and, in general, postpancreatectomy hemorrhage grade A has no major clinical impact, postpancreatectomy hemorrhage grade B requires adjustment of a given clinical pathway, including additional diagnostic examinations and intervention and, finally, postpancreatectomy hemorrhage grade C should always be considered potentially life threatening [5]. Postoperative mortality was defined as all deaths within 30 days after surgery; postoperative morbidity included all complications following surgery up to the day of discharge. The length of the postoperative period was defined as the interval from the day of surgery to discharge. Reoperation was defined as any surgical procedure performed in the first 30 postoperative days or before discharge from the hospital.
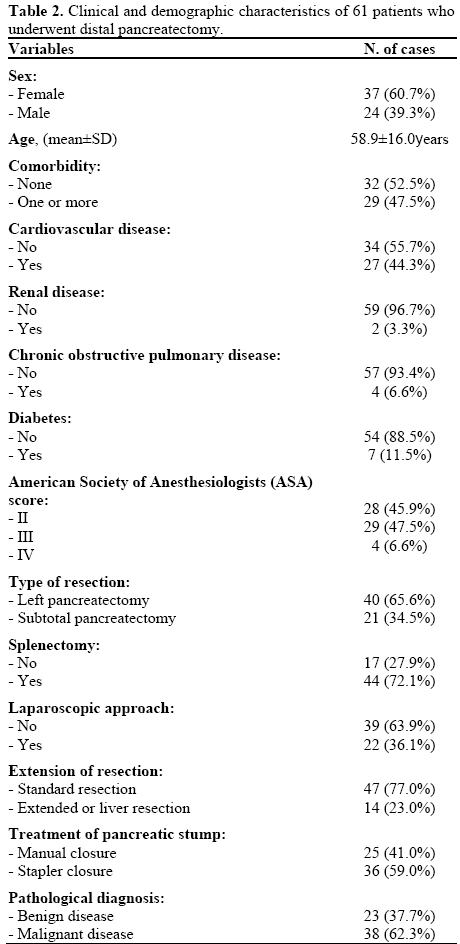
The characteristics of the 61 patients are summarized in Table 2. There were 24 (39.3%) males and 37 (60.7%) females, having a mean age of 58.9±16.0 years. Co-morbidities were present in 29 patients (47.5%) and, among them, the most frequent were cardiovascular diseases (44.3%). The majority of patients had an American Society of Anesthesiologists (ASA) score of II and III (45.9% and 47.5%, respectively) whereas a score of IV was present in only a few patients (6.6%). The type of distal pancreatectomy included 40 (65.6%) left pancreatectomies and 21 (34.5%) subtotal pancreatectomies. Standard resections were routinely performed (47, 77.0%); extended resections (14, 23.0%) included 5 liver resections and 9 resections of neighboring structures (stomach, kidney, etc.). The majority of the patients had malignant disease (38, 62.3%), while 23 patients (37.7%) had various benign pancreatic diseases.
ETHICS
No approval of institutional review committee was needed because the data of the present study were collected in the course common clinical practice and, accordingly, the signed informed consent was obtained from each patient for any surgical and clinical procedure. The study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004.
STATISTICS
Means, standard deviations, ranges, and frequencies were used to describe the data. Box and whiskers plot showed the interquartile ranges, the medians and the extreme values. The logarithmic transformation of the hospital stay was applied before analysis because these data were not normally distributed at the Kolmogorov- Smirnov test and showed a positive skewness. Data were analyzed by means of the one-way ANOVA; the linear trend and the simple contrast were applied. The linear by linear chi squared test was applied to discrete variables. All statistical analyses were made by running SPSS for Windows (version 13.0) on a personal computer. Two-tailed P values less than 0.05 were considered statistically significant.
RESULTS
Using the Clavien-Dindo classification, 30 out of 61 (49.2%) patients had no complications and 31 (50.8%) had at least one complication. The postoperative mortality rate (grade V) was 0%. The 31 complicated patients had the following grades: 9 patients (14.5%) had grade I, 15 (24.6%) had grade II, 6 (9.8%) had grade III and 1 (1.6%) had grade IV. The absence of major complications, as well as postoperative pancreatic fistula and postpancreatectomy hemorrhage, was reported in 4 out of 9 (44.4%) patients with grade I and in 7 out of 15 (46.7%) with grade II. Major complications were always present in grades III and IV. All patients with grade III required radiologic intervention not under general anesthesia (grade IIIa) and the patient with grade IV, who required the intensive care unit (ICU), underwent surgery under general anesthesia.
The mean length of the postoperative stay was 12.7 days (range 7-118 days.) The length of the postoperative stay, according to the grades of the Clavien-Dindo classification, is reported in Table 3 and Figure 1. The length of hospital stay progressively increased (P<0.001) from non-complicated patients to grade IV patients. The patient with grade IV was excluded from the analysis. It should be pointed out that the length of the postoperative stay was not significantly different between non-complicated patients and patients with grade I (P=0.303) while it was significantly shorter in non-complicated patients with respect to patients having grades II or III (P=0.008 and P<0.001, respectively).
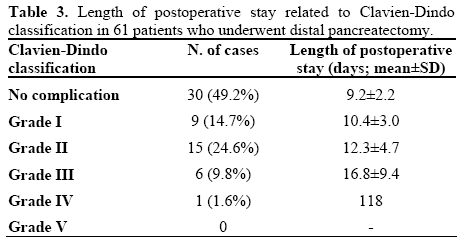
Figure 1. Box and whiskers plot showing the relationship between
the length of the postoperative stay and the Clavien-Dindo
classification. The boxes represent the interquartile ranges and the
lines within the boxes show the median values. The whiskers
represent the extreme values. The comparison between noncomplicated
patients and complicated patients demonstrates a
significantly shorter length of hospital stay (P<0.001) in noncomplicated
patients (grade IV was excluded due to the small
sample: No. 1).
aProgressive increase: linear trend ANOVA
bComparison of each grade with non complicated patients: ANOVA
with simple contrast
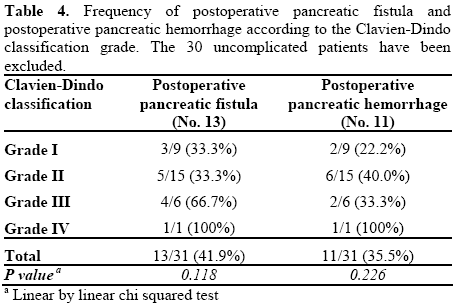
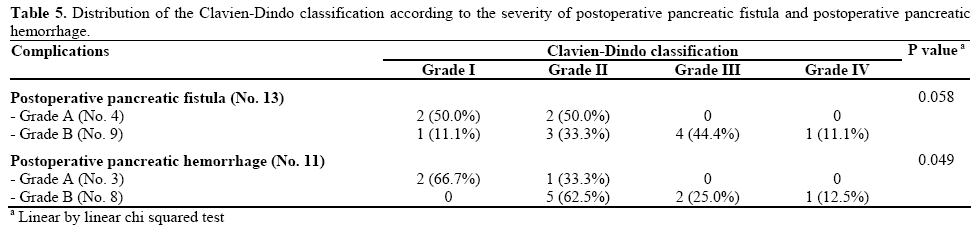
The most important complications following distal pancreatectomy were postoperative pancreatic fistula (14 patients, 23.0%) and postpancreatectomy hemorrhage (11 patients, 18.0%). One case of postoperative pancreatic fistula A was not considered to be a complicated patient in the Clavien-Dindo classification because it did not change the normal postoperative course as well as di not require any additional treatment The frequency of the most important complications following pancreatic resection is reported according to the grade of the Clavien-Dindo classification in Table 4. Postoperative pancreatic fistula and postpancreatectomy hemorrhage rates did not significantly increase from Clavien-Dindo grade I to grade IV (P=0.118, and P=0.226, respectively). Regarding the severity of the major complications, postoperative pancreatic fistula and postpancreatectomy hemorrhage were positively related (P=0.046 and P=0.023, respectively) with the grade of the Clavien-Dindo classification (Table 5). Postpancreatectomy hemorrhage showed a significant value (P=0.049) while postoperative pancreatic fistula was near the significant level (P=0.058); in particular, postoperative pancreatic fistulas and postpancreatectomy hemorrhages of grade A were present in Clavien-Dindo grades I and II only.
DISCUSSION
To our knowledge, this is the first prospective study evaluating the usefulness of the Clavien-Dindo classification, a grading system designed to classify postoperative course after distal pancreatectomy according to the treatment used for complications. In this classification, grades I and II include only a minor deviation from the normal postoperative course which can be treated with drugs, blood transfusions, physiotherapy and nutrition, while grades III and IV require surgical, endoscopic or radiologic intervention, and intermediate care or ICU management [7, 8, 9].
This grading system was objective and simple because the data recorded in our database were easily converted into this new classification. First, we noted that using this system, the rate of patients with any deviation from the normal postoperative course was very high (50.8%); only 49.2% of the patients had an uneventful postoperative course. In the literature, the lack of a stratified grading system for complications after surgery has not allowed proper evaluation of the surgical outcome. Probably, for this reason, the overall postoperative morbidity rate after a distal pancreatectomy was reported as lower and had a wide range [1, 2, 3]. Some authors have recently reported an overall morbidity rate after distal pancreatectomy using the Clavien-Dindo classification [3, 10]; Yoshioka et al. [3] recognized an overall morbidity rate of 65% of which 61% were grades I-II whereas only 4% were grades III-IV; Seeliger et al. [10] had an overall morbidity rate of 56.4% of which 32.7% were grades III and 18.2% were grades III-IV.
In the present study, the complicated patients were also more frequently in grades I and II, constituting about two-thirds of the complicated patients requiring only pharmacological treatment, whereas one-third of the complicated patients required management in the ICU or interventional treatment.
Patients with a normal postoperative course (i.e. those with no complications) had a significantly shorter hospital stay than patients defined as complicated in the Clavien-Dindo grading system. Thus, in our opinion, this grading system seems to be useful in recognizing a normal postoperative course from a complicated one; nevertheless, patients with no complications and patients with grade I are similar because grade I did not include particular pharmacologic treatment but only wound infections which opened at bedside. The length of the hospital stay significantly increased for grades II-III, demonstrating that the Clavien-Dindo classification is a useful tool for distinguishing among the increased grade of severity of the complications. Moreover, this result suggests that patients undergoing interventional treatment had a greater clinical impact on the length of hospital stay than patients who needed only medical treatment.
Regarding the relationship between the Clavien-Dindo classification and the most important complications after distal pancreatectomy, first of all, it should be pointed out that postoperative pancreatic fistulas A are sometimes not included in the complicated cases of the Clavien-Dindo grading system. This is probably due to the fact that, for the most part, postoperative pancreatic fistulas A do not have a clinical impact and they do not require any treatment. Moreover, patients with grades I or II did not have major complications in approximately 50% of the cases while, in grades III and IV, there were always major complications. Thus, the Clavien-Dindo classification appropriately selected those patients requiring additional surgical, radiologic or endoscopic intervention; in fact, the severity of both postoperative pancreatic fistula and postpancreatectomy hemorrhage was positively related with the severity of the Clavien-Dindo classification.
In conclusion, the Clavien-Dindo classification represents an objective and simple, way of reporting all complications in patients undergoing distal pancreatectomy. This classification system allows us to distinguish a normal postoperative course from any deviation and it satisfactorily distinguishes the severity of complications. Finally, according to our experience, this classification system seems to be of particular interest in comparing the various complications between different pancreatic surgical centers. However a definite statement on the clinical value is not yet possible due to the small case number, but the promising results should encourage further evaluation in larger cohort with the goal to possibly establish a standard classification.
Conflicts of interest
The authors have no potential conflicts of interest
References
- van Heek NT, Kuhlmann KF, Scholten RJ, de Castro SM, Busch OR, van Gulik TM, et al. Hospital volume and mortality after pancreatic resection: a systematic review and an evaluation of intervention in the Netherlands. Ann Surg 2005; 242:781-7. [PMID 16327488]
- Simons JP, Shah SA, Ng SC, Whalen GF, Tseng JF. National complication rates after pancreatectomy: beyond mere mortality. J Gastrointest Surg 2009; 13:1798-805. [PMID 19506975]
- Yoshioka R, Saiura A, Koga R, Seki M, Kishi Y, Morimura R, et al. Risk factors for clinical pancreatic fistula after distal pancreatectomy: analysis of consecutive 100 patients. World J Surg 2010; 34:121-5. [PMID 20020297]
- Bassi C, Dervenis C, Butturini G, Fingerhut A, Yeo C, Izbicki J, et al. Postoperative pancreatic fistula: an international study group (ISGPF) definition. Surgery 2005; 138:8-13. [PMID 16003309]
- Wente MN, Veit JA, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, et al. Postpancreatectomy hemorrhage (PPH): an International Study Group of Pancreatic Surgery (ISGPS) definition. Surgery 2007; 142:20-5. [PMID 17629996]
- Wente MN, Bassi C, Dervenis C, Fingerhut A, Gouma DJ, Izbicki JR, et al. Delayed gastric emptying (DGE) after pancreatic surgery: a suggested definition by the International Study Group of Pancreatic Surgery (ISGPS). Surgery 2007; 142:761-8. [PMID 17981197]
- Clavien PA, Sanabria JR, Strasberg SM. Proposed classification of complications of surgery with examples of utility in cholecystectomy. Surgery 1992; 111:518-26. [PMID 1598671]
- Dindo D, Demartines N, Clavien PA. Classification of surgical complications. A new proposal with evaluation in a cohort of 6336 patients and results of a survey. Ann Surg 2004; 240:205-13. [PMID 15273542]
- Clavien PA, Barkun J, de Oliveira ML, Vauthey JN, Dindo D, Schulick RD, et al. The Clavien-Dindo classification of surgical complications: five-year experience. Ann Surg 2009; 250:187-96. [PMID 19638912]
- Seeliger H, Christians S, Angele MK, Kleespies A, Eichhorn ME, Ischenko I, et al. Risk factors for surgical complications in distal pancreatectomy. Am J Surg 2010; 200:311-7. [PMID 20381788]


