Keywords
Diabetes Complications; Diabetes Mellitus, Type 2; Interleukin-6
Abbreviations
CRP C-reactive protein; T2DM type 2 diabetes mellitus
INTRODUCTION
The frequency of diabetes has been rapidly mounting worldwide. It is an assembly of metabolic syndrome characterized by hyperglycemia due to defective secretion of insulin. It has been divided into three main groups on the bases of its etiology and the pathophysiology; Type 1 diabetes mellitus (T1DM), results from the failure of insulin production by body due to destruction of pancreatic beta cells either through an autoimmune phenomenon of unknown reason [1, 2, 3]. Type 2 diabetes mellitus (T2DM) is due to decreased secretion and sensitivity of insulin. Type 3 diabetes mellitus is caused whichever by typical genetic mutation or linked with other various pathogenic conditions. Metabolism of sugar is divided into normal, intermediate and diabetic phase. Moreover, diabetic phase is further divided into non-insulin dependent, insulin dependent for glycemic management. The T2DM is probable to affect 20 million Americans which is dramatically growing in incidence and is linked with an augmented hazard for microvascular disease, particularly among females [3]. As of the resultant of various cardiovascular diseases typical related to T2DM, the monetary and practical burdens are maximum during late adulthood.Compounding such problems, more than one third of persons with T2DM are undiagnosed. About 30% have diabetic post complications including retinopathy, nephropathy or substantiation of micro and macro vasculopathies at clinical presentation [4]. Even though the most important physiological abnormalitiesare resistance and lack of insulin secretion [5, 6, 7]. The particular underlying causes of these metabolic abnormalities remain doubtful. A series of evidences suggeststhat inflammation may haveintermediaryrole in diabetic pathogenesis, thus concerning T2DM with many coexisting conditions deliberation to invent through inflammatory mechanisms. Regarding substantial experimental facts and more currentcross sectional studies recommend that IL-6 and CRP are two important susceptible physiological inflammatory markers which belong to subclinical systemic inflammation associatedwith high level of glucose, resistance of insulin and explicit T2DM [8, 9, 10, 11, 12, 13, 14, 15]. Certainly, it lately has been observed that T2DM may signify a syndrome of the inborn immune system [16] a suggestion of exacting interest as of CRP and IL-6 are inflammatory biomarkers involve to predict the progression of various vasculardiseases in or else healthy populations [17, 18, 19, 20].
The higher the hazard of T2DM in the obese people can moderately be explained by alters the functions of adipose tissue [21, 22, 23]. In the last few years, anassumption was anticipated to link thepathogenesis of T2DM with a condition of subclinical persistent inflammation [24, 25]. Epidemiological data have revealed that elevated plasma levels of CRP and IL-6 in patients of uncontrolled T2DM commonly observed [26]. Persistentlyhigh levels of these both bio-inflammatory markers promote onset of T2DM and as well as increase the hazard of its complications by functioning of endothelial [27] adipose and other tissues [28]. It remains imprecise whether the experiential alterations in plasma inflammatory parameters in T2DM are because of excess adipositiesor directly linked with the state of diabetes mellitus [29, 30]. We conjecture that altered plasma CRP and IL-6 inflammatory markers levels are associated to the obese situation and are not common in non-obese non-diabetic individuals. The current study compares the plasma CRP and IL-6 inflammatorymarkers between non-obese and non-diabetic normoglycemic controls versus obese T2DM patients [31]. In spite of these annotations, to our information, there are no available eventual data revealing the association between CRP and IL-6 concentrations showed correlation with the severity, extent, and progression of T2DM and therefore the current study conducted to find prognostic significance of those associations linked with both CRP and IL-6 are not simply being a markers of disease however additionally contributory to its pathological process. Thisidea can favor the employment of novel medicine that specifically block these inflammatory markers binding and its unhealthy effects in vivo among T2DM patients.
MATERIAL AND METHODS
A total of 200 subjects with almost five years duration of T2DM recruited from outpatient clinic of endocrinology and diabetes unit of Aziz Fatima trust hospital, Faisalabad were included in the current studies. Among these, 150 were of T2DM (BMI>30, waist>40 cm=Group-I), while 50 were healthy nondiabetic (BMI≤25, waist≤35 cm=Group-II). The average age of both groups ranged from 40-65 years (mean 52.5) and gender ratio was 1:1.
Ethical approval of research planincluding patient data collection sheet written both in English and Urdu (national language), was obtained and the data thus generated was submitted to the Institutional Ethics Committee. The privacy of all patients and confidentiality of personal information was ensuredand their informed consents were obtained prior to analysis.
All patients included the studies were subjected to complete clinical history and clinical examination.
The biochemical parameters were determined by using respective kits (Roche Diagnostics) following manufacturer’s protocols.
Fasting and random blood sugar by clinical chemistry analyzer cobas c 311 4th generation of routine chemistry Absorbance was noted at 350 nm and results were expressed as mg/dL glucose.
Glycated hemoglobin (HbA1c): Samples were homogenised and 20 uL of standard and well-mixed whole blood was pipetted into the properly labelled vials. Hemolysis reagent (1.0 mL) was added to each vial and vortex. The samples were incubated for 30 minutes at 37°C and loaded onto the Diastat for glycosylated hemoglobin estimation (%).
Lipid profile by clinical chemistry analyzer cobas c 311 4th generation of routine chemistry Absorbance was noted at 500 nm (cholesterol), 600 nm (HDL-C), 550 nm (LDL-C) and 500 nm (TG)appropriate wavelength for each parameter and results were expressed as mg/dL.
C-reactive protein (CRP) by clinical chemistry analyzer cobas c 311 5th generation of routine chemistry Absorbance was noted at 340nm and results were expressed as mg/dL CRP. Normal level of CRP is 1-3 mg/dL.
Interleukin-6 (IL-6) by (ELISA) Kits (Medgenix Diagnostics SA, B-6220 Fleurus, Belgium). The normal range for IL-6 values [32]: 0.08-5.0 pg/mL.
Exclusion Criteria
Patients with smoking habit, acute inflammations, acute infections and chronic liver diseases were excluded from our study.
Statistical Analysis
Statistical analysis was performed using SPSS 16.0 for windows software. The statistical significance of differences in CRP, IL-6 and other variables between the Group1 and Group 2 was estimated by Independent T test used. A multiple regression used fordetermine relation between CRP and IL-6 to onset of T2DM indiabetic patients. The p- values smaller than 0.05 were accepted a significant.
RESULTS
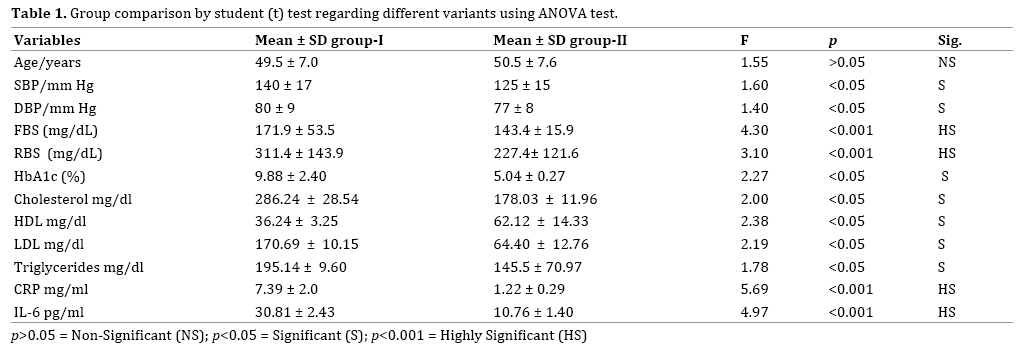
On comparing the diabetics group-I with the control group-II, a highly statistical significant difference (p<0.005) was recorded as regard CRP (7.39±2.0 vs. 1.22±0.29 mg/ dL) and IL-6 (30.81±2.43 vs. 10.76±1.40 pg/mL), fasting blood sugar (171.9±53.5 vs. 143.4±15.9 mg/dl), random blood sugar (311.4±143.9 vs. 227.4±121.6 mg/dl). There were also statistical significant differences (p<0.05) as HbA1c% (9.88±2.40 vs. 5.04±0.27). There were significant relation (p<0.05) noted of serum triglycerides (195.14± 9.60 vs. 145.5±70.97 mg/dl), Cholesterol (286.24±28.54 vs. 178.03±11.96). LDL-C (170.69±10.15 vs. 64.40±12.76) and HDL-C (36.24±3.25 vs. 62.12±14.33) between diabetic and control group respectively. Thus in agreement of Sattar et al. [33] a positive correlation exists between HbA1C CRP, IL-6 and lipid profile in diabetic subjects (Figures 1, 2, 3). Previous studies discovered that sufficient levels of various antioxidants for example vitamin D play crucial role to normalize the various metabolic parameters including cholesterol, HDL, LDL and triglycerides in T2DM patients. Comparison between Group 1 and Group 2 showed that CRP and IL-6 had a higher concentration in T2DM patients than normal control respectively (5.39±2.0 vs. 1.22±0.29; 30.81±2.43 vs. 10.76±1.40) (Table 1). We found in our study a positive significant correlation between CRP and IL-6 (r = 0.728, p<0.001) in diabetic patients (Figure 1).
Figure 1. Graphic presentation of correlation between HbA1c and CRP in diabetic patients (Group-I).
Figure 2. Graphic presentation of correlation between HbA1c and IL-6 in diabetic patients (Group-I).
Figure 3. Graphic presentation of correlation between IL-6 and CRP in diabetic patients (Group-I).
DISCUSSION
Type 2 diabetes mellitus is a multifaceted disorder that may be developed due to the interface between environmental or acquired and genetic factors.In our study we tend to found that diabetic patients showed considerably higher levels of C-reactive protein and IL-6 than did the controls (p<0.001). Inflammation is considered to play an important role in progression of T2DM; though, clinical figures addressing this problem are limited. CRP is an inflammatory biomarker formed and released from liver by the prompt of cytokines interleukins 1 and 6 [34]. In this district, various studies have confirmed that high levels of IL-6 and CRP among individuals found clinically unconcealed T2DM [35]. In the current study, it is attempted to assess the relationship of CRP and IL-6, the mainly frequent bio-inflammatory marker, with T2DM. Our results discovered that subjects with T2DM had considerable elevated levels of CRP and IL-6 with no association with gender, age and duration of having T2DM [36] present study also revealed that the level of bio inflammatory markers such as IL-6 and CRP were considerably elevated in T2DM patients than to normal control. Our study show that levels of CRP and IL-6 of T2DM patients is 2 fold higher than control group. In spite of that, we observed that CRP also associated with resistance of insulin in these subjects. Consequently, it also confirmed that CRP is a precise forecaster for the resistance of insulin in T2DM patients.
In agreement of previous studies both systolic and diastolic pressures, FBS, RBS, HbA1c, cholesterol and LDL was higher in T2DM subjects with positive correlation of CRP and IL-6. According to previous studies that high blood pressure was strong predictor of T2DM occurrence [37, 38, 39]. Even though our data hold up etiological relationship [40, 41, 42], at this time unambiguous mechanisms stay tentative and need further study. Our epidemiological interpretation, coupled with emerging investigational confirmation, support a probable role for inflammation in pathogenesis of T2DM [43]. One of the confines of present study must be considered; the small sample size of recruited subjects with limited associations of biochemical parameters, need further concise analytical statement of link between molecular and biochemical parameters in same type of studied subjects.
CONCLUSION
We report a positive independent association between elevated CRP levels and diabetes.As the progress in identification of above bio-inflammatory markers predisposing to T2DM in local population has been limited, therefore, future research is needed with the aim to examine association of these inflammatory markers and their candidate genes in Pakistani T2DM patients.
Conflict of Interest
The authors declare no conflict of interest.
References
- Harris M. Diabetes in America: Diabetes Data Compiled. 1995. Group NDD, ed. Bethesda, Md: National Institutes of Health, Dept of Health and Human Services.1995:1-13. Publication (PHS) 95-1468.
- Harris MI, Flegal KM, Cowie CC, Eberhardt MS, Goldstein DE, Little RR, et al. Prevalence of diabetes, impaired fasting glucose, and impaired glucosetolerance in U.S. adults: the Third National Health and Nutrition Examination Survey, 1988-1994. Diabetes Care 1998; 21:518-524. [PMID: 9571335]
- Manson J. Risk modification in the diabetic patient. In: Manson J, Ridker P, Gaziano J, Hennekens C, eds. Prevention of Myocardial Infarction. New York, NY: Oxford University Press, 1996:241-273.
- Harris MI, Klein R, Welborn TA, KnuimanMW. Onset of NIDDM occurs at least 4-7 yr before clinical diagnosis. Diabetes Care 1992; 15:815-819. [PMID: 1516497]
- Reaven GM. Banting lecture 1988: role of insulin resistance in human disease. Diabetes 1988; 37:1595- 1607. [PMID: 3056758]
- DeFronzo RA. Lilly lecture 1987: the triumvirate: beta-cell, muscle, liver: a collusion responsible for NIDDM. Diabetes 1988; 37:667-687. [PMID: 3289989]
- Bergman RN. Lilly lecture 1989: toward physiological understanding of glucose tolerance: minimalmodel approach. Diabetes 1989; 38:1512-1527. [PMID: 2684710]
- Sandler S, Bendtzen K, Eizirik DL, Welsh M. Interleukin- 6 affects insulin secretion and glucose metabolism of rat pancreatic islets in vitro. Endocrinology 1990; 126:1288-1294. [PMID: 2404746]
- Kanemaki T, Kitade H, Kaibori M, Sakitani K, Hiramatsu Y, Kamiyama Y, et al. Interleukin 1 beta and interleukin 6, but not tumor necrosis factor alpha, inhibit insulin-stimulated glycogen synthesis in rat hepatocytes. Hepatology 1998; 27:1296- 1303. [PMID: 9581683]
- Tsigos C, Papanicolaou DA, Kyrou I, Defensor R, Mitsiadis CS, Chrousos GP. Dose-dependent effects of recombinant human interleukin-6 on glucose regulation. J Clin Endocrinol Metab 1997; 82:4167-4170. [PMID: 9398733]
- Pickup JC, Mattock MB, Chusney GD, Burt D. NIDDM as a disease of the innate immune system: association of acute-phase reactants and interleukin-6 with metabolic syndrome X. Diabetologia 1997; 40: 1286-1292. [PMID: 9389420]
- Grau AJ, Buggle F, Becher H, Werle E, Hacke W. The association of leukocyte count, fibrinogen and Creactive protein with vascular risk factors and ischemic vascular diseases. Thromb Res 1996; 82:245-255. [PMID: 8732628]
- Ford ES. Body mass index, diabetes, and Creactive protein among U.S. adults. Diabetes Care. 1999; 22:1971-1977. [PMID: 10587828]
- Festa A, D’Agostino R Jr, Howard G, Mykkanen L, Tracy RP, Haffner SM. Chronic subclinical inflammation as part of the insulin resistance syndrome: the Insulin Resistance Atherosclerosis Study (IRAS). Circulation 2000; 102:42-47. [PMID: 10880413]
- Frohlich M, Imhof A, Berg G, Hutchinson WL, Pepys MB, Boeing H, et al. Association between C-reactive protein and features of the metabolic syndrome: a population-based study. Diabetes Care 2000; 23:1835-1839. [PMID: 11128362]
- Pickup JC, Crook MA. Is type II diabetes mellitus a disease of the innate immune system? Diabetologia 1998; 41:1241-1248. [PMID: 9794114]
- Ridker PM, Cushman M, Stampfer MJ, Tracy RP, Hennekens CH. Inflammation, aspirin, and the risk of cardiovascular disease in apparently healthy men. N Engl J Med 1997; 336:973-979. [PMID: 9077376]
- Koenig W, Sund M, Frohlich M, Fischer HG, Löwel H, Döring A, et al. Reactive protein, a sensitive marker of inflammation,predicts future risk of coronary heart disease in initially healthy middle-aged men: results from the MONICA (Monitoring Trends and Determinants in CardiovascularDisease) Augsburg Cohort Study, 1984 to1992. Circulation 1999; 99:237-242. [PMID: 9892589]
- Ridker PM, Hennekens CH, Buring JE, Rifai N. Creactive protein and other markers of inflammation in the prediction of cardiovascular disease in women. N Engl J Med 2000; 342:836-843. [PMID: 10733371]
- Ridker PM, Rifai N, Stampfer MJ, Hennekens CH. Plasma concentration of interleukin-6 and the risk of future myocardial infarction among apparently healthy men. Circulation 2000; 101:1767-1772. [PMID: 10769275]
- Jensen MD. Role of body fat distribution and the metabolic complications of obesity. J Clin Endocrinol Metab 2008, 93:S57–S63. [PMID: 18987271]
- Bastard JP, Maachi M, Lagathu C, Kim MJ, Caron M, Vidal H, et al. Recent advances in the relationship between obesity, inflammation, and insulin resistance. Eur Cytokine Netw 2006; 17:4–12. [PMID: 16613757]
- Rasouli N, Kern PA. Adipocytokines and the metabolic complications of obesity. J Clin Endocrinol Metab 2008; 93:S64–S73. [PMID: 18987272]
- Badawi A, Klip A, Haddad P, Cole D, Garcia Bailo B, El-Sohemy A, et al. Type 2 diabetes mellitus and inflammation: prospects for biomarkers of risk and nutritional intervention. Diabetes Metab Syndr Obes 2010; 3:173–186. [PMID: 21437087]
- Donath MY, Shoelson SE. Type 2 diabetes as an inflammatory disease. Nat Rev Immunol 2011; 11:98–107. [PMID: 21233852]
- Mirza S, Hossain M, Mathews C, Martinez P, Pino P, Gay JL, et al. Type 2-diabetes is associated with elevated levels of TNF-alpha, IL-6 and adiponectin and low levels of leptin in a population of Mexican Americans: a cross-sectional study. Cytokine 2012; 57:136–142. [PMID: 22035595]
- Calle MC, Fernandez ML. Inflammation and type 2 diabetes. Diabetes Metab 2012; 38:183–191. [PMID: 22252015]
- King GL. The role of inflammatory cytokines in diabetes and its complications. J Periodontol 2008; 79:1527–1534. [PMID: 18673007]
- Abdelgadir M, Elbagir M, Eltom M, Berne C, Ahrén B. Reduced leptin concentrations in subjects with type 2 diabetes mellitus in Sudan. Metabolism 2002; 51:304–306. [PMID: 11887164]
- Bahceci M, Gokalp D, Bahceci S, Tuzcu A, Atmaca S, Arikan S. The correlation between adiposity and adiponectin, tumor necrosis factor alpha, interleukin-6 and high-sensitivity c-reactive protein levels. Is adipocyte size associated with inflammation in adults? J Endocrinol Invest 2007; 30:210–214. [PMID: 17505154]
- Lilja M, Rolandsson O, Norberg M, Soderberg S. The impact of leptin and adiponectin on incident type 2 diabetes is modified by sex and insulin resistance. Metab Syndr Relat Disord 2012; 10:143–151. [PMID: 22283633]
- Di Cesare PE, Chang E, Preston CF, Liu CJ. Serum interleukin-6 as a marker of periprosthetic infection following total hip and knee arthroplasty. J Bone Joint Surg Am 2005; 87:1921-1927. [PMID: 16140805]
- Hansen D, Dendale P, Beelen M, Jonkers RA, Mullens A, Corluy L, et al, Plasma adipokine and inflammatory marker concentrations are altered in obese, as opposed to non-obese, type 2 diabetes patients. Eur J Appl Physiol 2010; 109:397-404. [PMID: 20131064]
- Fröhlich M, Imhof A, Berg G, Hutchinson WL, Pepys MB, Boeing H, et al. Association between C-reactive protein and features of the metabolic syndrome: a population-based study. Diabetes Care 2000; 23:1835-1839. [PMID: 11128362]
- Yeo ES, Hwang JY, Park JE, Choi YJ, Huh KB, Kim WY. Tumor necrosis factor (TNF-alpha) and C-reactive protein (CRP) arepositively associated with the risk of chronic kidney disease in patients with type 2 diabetes. Yonsei Med J 2010l; 51:519-25. [PMID: 20499416]
- Pickup JC, Crook MA. Is type II diabetes mellitus a disease of the innate immune system? Diabetologia 1998; 41:1241-1248. [PMID: 9794114]
- Gewurz H, Zhang XH, Lint TF. Structure and function of the pentraxins. Curr Opin Immunol 1995; 7:54-64. [PMID: 7772283]
- Fearon DT, Locksley RM. The instructive role of innate immunity in the acquired immune response. Science 1996; 272:50-53. [PMID: 8600536]
- Medzhitov R, Janeway CA, Jr. Innate immunity: impact on the adaptive immune response. Curr Opin Immunol 1997; 9:4-9. [PMID: 9039775]
- Steel DM, Whitehead AS. The major acute phase reactants: C-reactive protein, serum amyloid P component and serum amyloid A protein. Immunol Today 1994; 15:81-88. [PMID: 8155266]
- Mortensen R. Macrophages and acute-phase proteins. In: Zwilling B, Eisenstein T, eds. Macrophage-Pathogen Interactions. New York, NY: Marcel Deckker; 1994:143-158.
- Naila AS, Hussain F, Jamil A, Sarfraz A. Evaluation of biochemical parameters among type 2 diabetes mellitus patients in Pakistan. Oxidation Communications 2017; 40:220–225.
- Sheu WH, Wang WC, Wu KD, He CT, Hwu CM, Quertermous T, et al. CRP-level-associated polymorphism rs1205 within the CRP gene is associated with 2-hour glucose level: The SAPPHIRe study. Scientific Reports 2017; 7:7987. [PMID: 28801571]




