Keywords
Amylases; Creatine Kinase; macroamylase
INTRODUCTION
A distinctive characteristic of macroenzymes is a molecular mass higher than that of the corresponding enzymes normally found in serum under physiological or pathophysiological conditions [1]. The prevalence of macroenzymes is not wellestablished but it is generally considered to be a rare event, occurring in 1.5-2.5% of the general population [2, 3, 4]. The group of serum macroenzymes includes macroamylase, macro-creatine kinase, macro-lactic dehydrogenase, macro-alkaline phosphatase, macroaspartate aminotransferase, and macrogamma- glutamyltransferase [5]. By causing falsely increased total serum enzyme levels, the occurrence of one of the above-listed macroenzymes is frequently responsible for diagnostic confusion leading to additional unnecessary, costly and often invasive procedures in clinical practice. In particular, macroamylasemia and macro-creatine kinasemia may generate diagnostic confusion in the differential diagnosis between acute pancreatitis and myocardial infarction, respectively. Until now, the association of macroamylase and macro-creatine kinase in the same patient has never been described. This article reports such association for the first time.
CASE REPORT
A 68-year-old female was admitted because of distal edema and mild dyspnea. The most important anamnestic findings were a previous diagnosis of arterial hypertension with secondary cardiac involvement (left ventricular hypertrophy with an ejection fraction within the reference range) and a previous cholecystectomy (15 years before, for gallstones). The patient took furosemide and ramipril as her principal home treatment
Laboratory investigation showed increased serum levels of creatine kinase and amylase (40 and 4 times the reference upper value, respectively) some days before hospitalization. At admission to the Emergency Department, the patient complained of non-specific symptoms such as weakness and tiredness. Even if physical examination showed only mild bilateral ankle edema, without major features of congestive heart failure or ischemic disease, or abdominal complaints/pathologic findings, the confirmed high levels of total creatine kinase and amylase (Table 1) led to an extensive diagnostic work-up searching for cardiac or pancreatic illnesses. The patient underwent seriate electrocardiograms, a chest roentgenogram, echocardiography, Doppler ultrasonography of the legs, abdominal ultrasound, and chest and abdomen contrastenhanced computed tomography. After this, the patient was transferred to our Unit where the diagnostic program was supplemented with assays of serum pancreatic isoamylase, serum lipase, 24 h amylasuria, amylase/creatinine clearance ratio (Table 1), and serum creatine kinase isoenzymes assay and electrophoresis (Figure 1). The patient was then discharged with a final diagnosis of mild arterial hypertension (WHO stage II, with compensated secondary cardiac involvement) and macroenzyme syndrome (association of macroamylase and macrocreatine kinase).
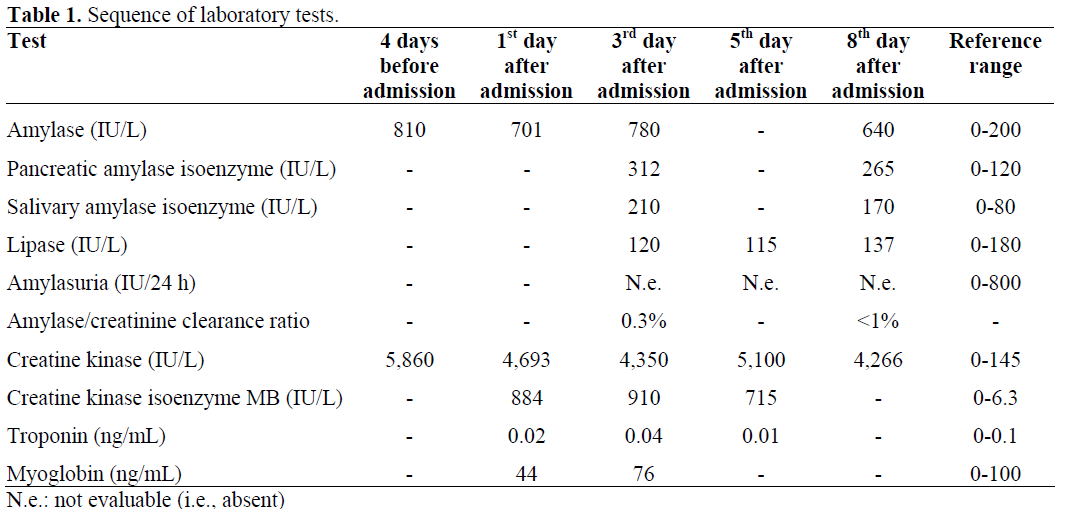
Figure 1. Agarose gel electrophoresis of serum
creatine kinase.
a Position of isoenzyme MM migration
b Peak of type I-macro creatine kinase
c Position of isoenzyme MB migration
DISCUSSION
Macroamylase is a complex composed of an immunoglobulin (IgG or more frequently IgA) bound to an amylase molecule, the salivary or pancreatic isoenzymes, or both [5]. This macrocomplex does not pass the renal filter and, as a consequence, its renal clearance is low. Another form of macroamylase (characteristically transient) is an enzyme-substrate complex of amylase and intravenously infused high molecular mass glycoprotein or polysaccharide (e.g., hydroxyethyl starch) [1]. Immunoglobulinbound macroamylase is indistinguishable from normal amylase in a quantitative amylase assay and causes a false increase of total serum enzyme activity. Identification of serum macroamylase is difficult on agarose gel electrophoresis because it appears as a smeared band which may overlap the normal position of the salivary or pancreatic isoenzyme [1, 6]. Polyethylene glycol precipitation associated with fast protein liquid chromatography was suggested as the most reliable method for identifying the macromolecular complex [7], but this assay is quite complex and, currently, it is rarely utilized in the majority of laboratories. For these reasons, an increased value of total serum amylase with a normal value for lipase together with normal/decreased amylase in the urine or a decreased amylase-creatinine clearance ratio (less than 1%) are usually used for the identification of macroamylase in clinical practice [4, 5]. Typically macroamylasemia represents a biochemical abnormality in which an elevated serum amylase level is present in asymptomatic subjects without any kind of pathology. However, in the presence of symptoms, especially of abdominal origin, it is important that this condition be identified accurately in order to avoid unnecessary diagnostic examinations or treatment for pancreatitis or other related diseases. More rarely, macroamylasemia has been found to occur in a variety of diseases including celiac disease, monoclonal gammopathy, HIV infection, ulcerative colitis, and rheumatoid arthritis [5, 6]. Only in celiac disease there are data indicating that the presence of macroamylasemia is not merely an incidental finding, but it is in some way linked to the pathogenetic mechanism of the disease [8]. In this respect, macroamylasemia disappeared after various patients followed a gluten-free diet [9, 10].
Macro-creatine kinase in serum occurs in two major forms. Type I macro-creatine kinase is a complex constituted of an immunoglobulin (usually IgG or IgA) bound to two creatine kinase isoenzymes (creatine kinase-MB and, more frequently, creatine kinase-BB) [3]. It is detectable in 2% of the population, most commonly affects elderly women, frequently persists for months or years, and is usually not associated with specific diseases [1]. More rarely, type I macro-creatine kinase has been described in patients with irritable bowel syndrome, bronchopulmonary chronic illness, and immunological disorders [3]. The real clinical significance of such an association is unclear. Type II macro-creatine kinase is oligomeric mitochondrial creatine kinase, released as a result of tissue necrosis; it is usually a transient finding and is most frequently found in the serum of patients who have widespread tissue destruction or who are terminally ill [2]. Macro-creatine kinase is indistinguishable from normal creatine kinase in a quantitative total enzymatic assay and may give a false overestimation of total creatine kinase activity. Electrophoresis identifies macro-creatine kinase (Figure 1), as it usually migrates between the MM or MB isoenzyme positions. Misleading higher values may cause confusing laboratory results and can lead to additional pointless investigation. In fact, many disorders may present an abnormally high value of creatine kinase, i.e., muscle, neurological, pulmonary and neoplastic diseases whereas, concerning possible confusion in laboratory work-ups for ischemic heart disease, the utilization of the troponin serum assay has cleared up any diagnostic doubt.
To the best of our knowledge, the present case represents, within the group of patients presenting macroenzymes, the first one in which the association of macroamylasemia and macro-creatine kinasemia is reported in the English literature
Conflict of interest
The authors have no potential conflicts of interest
References
- Mifflin TE, Bruns DE, Wrotnoski U, MacMillan
RH, Stallings RG, Felder RA, Herold DA. University
of Virginia case conference. Macroamylase, macro
creatine kinase, and other macroenzymes. Clin Chem
1985; 31:1743-8. [PMID 2412731]
- Sturk A, Sanders GT. Macro enzymes: prevalence,
composition, detection and clinical relevance. J Clin
Chem Clin Biochem 1990; 28:65-81. [PMID 2184194]
- Lee KN, Csako G, Bernhardt P, Elin RJ.
Relevance of macro creatine kinase type 1 and type 2
isoenzymes to laboratory and clinical data. Clin Chem
1994; 40:1278-83. [PMID 8013099]
- Steinberg W, Tenner S. Acute pancreatitis. N Engl
J Med 1994; 330:1198-210. [PMID 7811319]
- Galasso PJ, Litin SC, O'Brien JF. The
macroenzymes: a clinical review. Mayo Clin Proc
1993; 68:349-54. [PMID 7681133]
- Forsman RW. Macroamylase: prevalence,
distribution of age, sex, amylase activity, and
electrophoretic mobility. Clin Biochem 1986; 19:250-
3. [PMID 2428542]
- Lawson GJ. Prevalence of macroamylasaemia
using polyethylene glycol precipitation as a screening
method. Ann Clin Biochem 2001; 38:37-45. [PMID
11270840]
- Sanders DS. Macroamylasemia in celiac disease: a
novel observation, but what does it mean? Am J
Gastroenterol 2002; 97:1068. [PMID 12003397]
- Deprettere AJ, Eykens A, Van Hoof V.
Disappearance of macroamylasemia in a celiac patient
after treatment with a gluten-free diet. J Pediatr
Gastroenterol Nutr 2001; 33:346-8. [PMID 11593136]
- Rabsztyn A, Green PH, Berti I, Fasano A, Perman
JA, Horvath K. Macroamylasemia in patients with
celiac disease. Am J Gastroenterol 2001; 96:1096-100.
[PMID 11316153]


