Keywords
Pancreas; Endoscopic Ultrasound-Guided Fine Needle
Aspiration
Introduction
The role of pancreatic endoscopic ultrasoundguided
fine needle aspiration (EUS-FNA) cytology in
diagnosis and management of pancreatic lesions is wellestablished.
The Papanicolaou Society of Cytopathology
recently proposed a standardized terminology scheme
for pancreatobiliary specimens that correlate cytological
diagnosis with biological behavior and increasingly
conservative patient management of surveillance only
[1]. The proposed terminology scheme recommends a sixtiered
system which includes an ‘atypical’ interpretation
category. ‘Atypical’ diagnoses are rendered in cases where
qualitative cytologic features fall short of malignancy
and overlap with those seen in benign processes. Low
cellularity and premalignant changes (dysplasia) may
also be included within this category. Additionally, in
many instances, gastrointestinal tract contamination is not easily distinguished from a mucinous neoplasm of the
pancreas. The presence of atypical cells in a background of
benign pancreatic tissue, where a neoplasm or malignancy
cannot be confidently excluded, is also well-placed within
this interpretation category [2]. The risk of malignancy of
‘atypical’ diagnoses has been shown to range from 25%
to 100% [1, 3, 4, 5]. Alston et al. reported the risk of a
pancreatic neoplasm ranges from 6% to 93%, a reflection
of the range of benign to malignant/neoplastic lesions
represented by this diagnosis [6].
The existing literature reports a mean ‘atypical’
reporting rate for EUS-FNA ranging from 1% to 14% (mean
5.3%) [4]. However, these studies do not comment on the
experience of the reporting pathologists in interpreting
these challenging cytologic specimens. We conducted a
retrospective study to determine the frequency of use of
‘atypical’ in pancreatic EUS-FNA within our institution
and to determine the interobserver agreement on a
uniform test set of EUS-FNA smear samples in a group
of pathologists with variable experience in pancreatic
cytopathology smear interpretation.
Materials and Methods
Following Institutional Review Board approval, cases
of EUS-FNA procedures performed from January 2007
to December 2012 were extracted from the pathology
database. Other recorded clinical data included: age, sex, initial and follow-up radiological findings (either from CT
scans, MRI scans or ERCP findings), EUS-FNA diagnoses
and follow-up biopsy/resection information, where
available. Fluid chemistry levels (for example, CEA and
amylase) were not available at the time of the study.
EUS-FNA procedures were performed under conscious
sedation using 22 gauge needles with a cytotechnologist
present for on-site evaluation of adequacy. For on-site
adequacy, only DiffQuik (Baxter, McGraw Park, IL) staining
was used. Final pathology diagnosis was performed
with additional Papanicolaou-stained slides as well as
hematoxylin and eosin stained cell blocks where available.
Five hundred and ninety-eight EUS-FNA cases were
reported during this time period as ‘benign’, ‘malignant’ or
‘atypical’. ‘Benign’ cases included those with normal tissue
like pancreatic acinar (grape-like) and ductal (monolayered
sheet with well-spaced nuclei), inflammation and
reactive processes with no significant cytologic atypia.
‘Malignant’ cases included specimens with unequivocal
diagnostic features of malignancy including crowded sheets
and clusters of cells with significant cytoarchitectural
and nuclear atypia, discohesive single abnormal cells,
mitoses and necrosis. ‘Atypical’ cases displayed features as
described earlier (Figure 1). From the 598 EUS-FNA cases,
twenty-eight were selected for review within this study,
including 18 cases with ‘atypical’, 5 cases with ‘benign’ and
5 cases with ‘malignant’ diagnoses. Cases reported as ‘nondiagnostic’
or ‘suspicious’ were excluded from the initial selection. Eight participating pathologists with variable
experience in evaluating cytology specimens (3 to 20
years) blindly reviewed these cases using standard terms
in reporting categories used within our institution: ‘nondiagnostic’
(unsatisfactory/inadequate), ‘benign’, ‘atypical’,
‘suspicious’ (suspicious for neoplasm) and ‘malignant’
(positive for neoplasm). The free-marginal kappa (Kfree) [7]
was calculated to determine the interobserver agreement.
The ranges of agreement are as follows: -1.0: perfect
agreement, 0.0: agreement equal to chance, 0.01-0.2: slight
agreement, 0.21-0.4: fair agreement, 0.41-0.6 moderate
agreement, 0.61-0.8: substantial agreement and 0.81-1.0:
almost perfect agreement.
Figure 1. (a, b). ‘Atypical’ cells on cytology, and inflammation on final histology. (DiffQuik, magnification 20x; Papanicolaou stain, magnification 10x). (c,
d). ‘Atypical’ cells on cytology and adenocarcinoma with mucinous and papillary features on final histology (DiffQuik, magnification 40x; Papanicolaou
stain, magnification 20x).
The ‘atypical’ reporting rate for each pathologist over
the 6 year time period was also calculated by dividing the
number of ‘atypical’ diagnoses made by the individual
pathologist over the total number of cases reported for the
year.
Results
Five hundred and ninety-eight pancreatic EUS-FNA
cases were screened during the study period of 6 years
(2007 to 2012), of which 29 (4.9%) were reported as
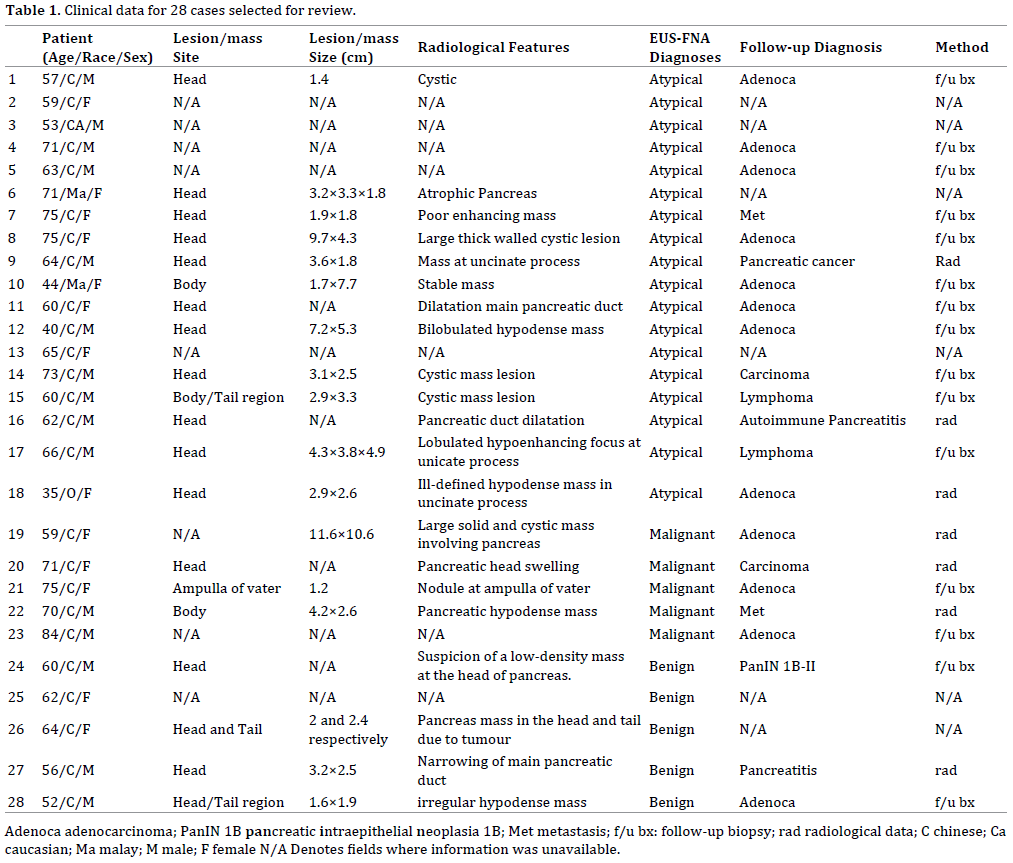
atypical. Twenty-eight cases were selected for blinded
review. These patients included 15 males and 13 females
with a mean age of 62 years (range: 35-84). Radiological
information was available for twenty cases: 16 with a head
of pancreas mass, 1 with an ampulla of Vater mass and 3 pancreas body/tail masses by imaging studies. All, except
one, were described as solid hypodense masses (Table 1).
Of the 28 cases reviewed, 18 were originally diagnosed
as ‘atypical’ on cytology. Thirteen (72%) of these cases
were malignant on histologic follow-up, 1 was benign
and 4 did not have follow-up tissue diagnoses. Following
blinded review by 8 pathologists with variable experience
in interpreting such smears, the free-marginal kappa (Kfree)
was calculated for the ‘overall’ 28 cases, 18 ‘atypical’, 5
‘benign’ and 5 ‘malignant’ cases. Slight agreement (Kfree 0.15
and 0.07, respectively) was observed with the ‘overall’ and
‘atypical’ categories and fair agreement (Kfree 0.34 and 0.22,
respectively) was observed with the ‘benign’ and ‘malignant’
categories (Table 2). As ‘suspicious’ and ‘malignant’
diagnoses were used almost interchangeably among the pathologists, the two interpretations were combined and the
Kfree calculated comparing the following diagnostic categories:
‘non-diagnostic’, ‘benign’, ‘atypical’ and ‘suspicious/
malignant’. The Kfree increased to 0.50 (moderate agreement)
for a ‘suspicous/malignant’ diagnosis (Table 3).


Five hundred and ninety-eight EUS-FNA cases were
reported between January 2007 and December 2012. The
yearly atypical reporting rate fluctuated between 1.6% to
7.0% with an average of 5.1% (standard deviation: 1.83)
(Table 4). Figure 2 shows the percentage distribution
of pancreatic EUS-FNA cases reported by each of the 8
pathologists involved in the current study, as well as other
pathologists within the department who did not report any
atypical cases during the study period. The 8 pathologists
individually reported between 3 (1%) and 140 (24%) EUS-FNA cases within the study period. The mean ‘atypical’
reporting rate was 5.9% (standard deviation: 5, range:
12.2-0.7%); two pathologists who reported less than 20
EUS-FNA cases were excluded (Figure 3).
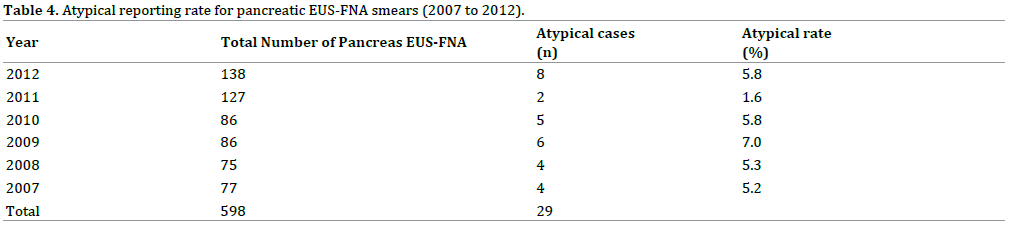
Figure 2. Percentage distribution of pancreatic EUS-FNA cases reported
by each pathologist, ‘A’ to ‘H’ (‘Others’ refer to pathologists that did not
report any atypical cases from 2007 to 2012).
Figure 3. Atypical reporting rate of eight pathologists, ‘A’ to ‘H’
(pathologists ‘D’ and ‘E’ were excluded as they reported less than 20
pancreatic EUS-FNA cases from 2007-2012).
Discussion
In their review of EUS-FNA samples reported within
their institution, Saieg et al. applied the newly proposed
standardized terminology scheme to 155 cases reported
over a 12-month period. Twenty-nine (18.7%) ‘atypical’
diagnoses were re-interpreted as ‘neoplastic-other’ as
these cases were of cystic neoplasms with no features of
high grade dysplasia [8]. This reiterates the importance
of knowledge of radiological findings when interpreting
such specimens. Cyst fluid CEA and amylase levels are also
helpful to the cytopathologist in rendering an accurate
diagnosis [9, 10]. This additional information would no
doubt have improved the interobserver agreement in this
study. However, the clinico-radiological findings were not
made available to the reviewing pathologists in this study
in order to assess interpretation differences based solely on
the cytomorphologic findings. In the case of cystic lesions,
fluid CEA and amylase levels were not recorded as those
tests were not available within our institution at the time
of the study. Additionally, the interpretation categories
were kept at 5 tiers as they are the standard reporting
terms the pathologists used in our institution before
the introduction of the fairly new 6-tier system. For the
purposes of our study, which was to assess differences in
the ‘atypical’ interpretation, the exclusion of a ‘Neoplasticbenign/
other’ category was deemed acceptable.
The inter-observer agreement level for benign
and malignant control cases was ‘fair’ (0.34 and 0.22,
respectively). This was lower than expected and could be
attributed to the wide range of interpretive experience (3
to 20 years) and confidence level among the participating
pathologists. The ‘atypical’ reporting rates recorded in
the literature range from 1% to 14% (mean, 5.3%) [4].
The mean ‘atypical’ reporting rate of 5.9% within our
institution for the 6 year study period falls well within this
range. The differences in individual ‘atypical’ reporting
rates amongst cytopathologists were remarkably different,
although the number of cases reported by each pathologist
also varied widely (Figure 3), reiterating the fact that
likely contributing factors for these differences include
frequency of interpreting such cases, the varying years of practice experience, confidence level and expertise in
pancreatic cytopathology smear interpretation, excluding
the limitations due to the inherent nature of the lesion or
material itself [11]. This was similarly shown by Schneider
et al. who reported improved rates of sensitivity and
negative predictive value of EUS-FNA performed at a
specialized cytology institute compared to a standard
pathology service [12].
In our study, the overall inter-observer agreement for
the 28 pancreas EUS-FNA smears after review was poor,
especially for the 18 atypical smears. It improved after
combining the ‘suspicious’ and ‘malignant’ categories
together, especially for the 5 malignant cases, which
suggests that, as expected, the pathologists had stronger
threshold levels for a ‘malignant’ diagnosis. The interobserver
agreement level for the 18 atypical cases was
the lowest compared to the other diagnostic groups
reviewed (5 benign and 5 malignant cases). There are
many well-documented reasons why cytological smears
are interpreted as atypical, including low specimen
cellularity, gastro-intestinal tract contaminants, poor cell
preservation and under-diagnosis [9]. The variability in
both the atypical reporting rates and overall poor interobserver
agreement amongst reviewing pathologists has
implications for practice as well as education. In low-volume
centers, cytopathologists and cytopathology trainees who
have limited exposure to pancreatic EUS-FNA’s or a limited
range of benign to malignant/neoplastic lesions which
are sampled need to be cautious in interpretation until
adequate experience is gained, and with the hindsight of
histologic correlation. Where available, the addition of cell
blocks can be useful to provide additional information in
rendering a diagnosis. However, these are ever dependent
on adequate sampling. We performed a cell block utility
study using paired smears and cell blocks resulting in
63 (83%), 9 (11%) and 2 (3%) of 73 cases confidently
diagnosed as malignant, benign and non-diagnostic,
respectively, with the addition of cell block material and
only 2 (3%) cases remained as ‘atypical’ (data not shown).
This is a single center study that has evaluated the
difficult area of the ‘atypical’ diagnostic category in
pancreatic EUS-FNA. We have established our rates and
compared them against the published literature and
studied interobserver variations in the reporting of this
category. Additionally, quality criteria and thresholds in
non-gynecological cytology are not well-established in
such specimens. Our results may provide the basis for
developing atypical rates as a measure of quality both as a
service as a whole as well as for tracking in routine practice
as an additional measure of quality assurance.
Conclusion
The overall poor agreement level amongst participating
pathologists indicates that occasional interpretation of
pancreatic cytology should be discouraged. In order to be
a reliable and responsible interpreter of pancreatic EUSFNA
cytology samples, regular and frequent exposure to
such specimens is essential. The results also emphasize the limitations of evaluating EUS-FNA samples solely
based on cytomorphology. Adjunct imaging, fluid chemistry
and clinical information are essential to increase diagnostic
accuracy. Proper training guidelines and aspects on workload
should be established in the development of a high-quality
pancreatic EUS service. In addition, development of quality
control based on aggregated and individualized reporting
rates for the ‘atypical’ may serve as a simple tool for improving
and monitoring of a routine EUS service.
Ethics Statement
Subjects have given their informed consent. This study
protocol has been approved by the institute's committee
on human research and thus meets the standards of the
Declaration of Helsinki in its revised version of 1975
and its amendments of 1983, 1989, and 1996 [JAMA
1997;277:925-926].
Conflict of Interest
The authors have declared that no competing interests
exist.
References
- Pitman MB, Centeno BA, Ali SZ, Genevay M, Stelow E, Mino-Kenudson
M, et al. Standardized terminology and nomenclature for pancreatobiliary
cytology: The Papanicolaou Society of Cytopathology Guidelines.
Cytojournal 2014; 11:3. [PMID: 25191517]
- Bergeron JP, Perry KD, Houser PM, Yang J. Endoscopic ultrasoundguided
pancreatic fine-needle aspiration: potential pitfalls in one
institution's experience of 1212 procedures. Cancer Cytopathol 2015;
123:98-107. [PMID: 25410732]
- Bellizzi AM, Stelow EB. Pancreatic cytopathology: a practical
approach and review. Arch Pathol Lab Med 2009; 133:388-404. [PMID:
19260745]
- Abdelgawwad MS, Alston E, Eltoum IA. The frequency and cancer
risk associated with the atypical cytologic diagnostic category in
endoscopic ultrasound-guided fine-needle aspiration specimens of solid
pancreatic lesions: a meta-analysis and argument for a Bethesda System
for Reporting Cytopathology of the Pancreas. Cancer Cytopathol 2013;
121:620-8. [PMID: 23881871]
- Layfield LJ, Schmidt RL, Hirschowitz SL, Olson MT, Ali SZ, Dodd LL.
Significance of the diagnostic categories "atypical" and "suspicious for
malignancy" in the cytologic diagnosis of solid pancreatic masses. Diagn
Cytopathol 2014; 42:292-6. [PMID: 24578254]
- Alston E, Bae S, Eltoum IA. Atypical cytologic diagnostic category in
EUS-FNA of the pancreas: follow-up, outcomes, and predictive models.
Cancer Cytopathol 2014; 122:428-34. [PMID: 24436110]
- Brennan RL, Prediger, DJ. Coefficient Kappa: Some uses, misuses, and
alternatives. Educ Psychol Meas 1981; 41: 687-699.
- Saieg MA, Munson V, Colletti S, Nassar A. The impact of the new
proposed Papanicolaou Society of Cytopathology terminology for
pancreaticobiliary cytology in endoscopic US-FNA: A single-Institutional
experience. Cancer Cytopathol 2015; 123:488-94. [PMID: 25994860]
- Oppong KW, Dawwas MF, Charnley RM, Wadehra V, Elamin K, White
S, et al. EUS and EUS-FNA diagnosis of suspected pancreatic cystic
neoplasms: Is the sum of the parts greater than the CEA? Pancreatology
2015; 15:531-7. [PMID: 26375415]
- McKinley M, Newman M. Observations on the application of the
Papanicolaou Society of Cytopathology standardised terminology and
nomenclature for pancreaticobiliary cytology. Pathology 2016; 48:353-6.
[PMID: 27114371]
- Payne M, Staerkel G, Gong Y. Indeterminate diagnosis in fine-needle
aspiration of the pancreas: reasons and clinical implications. Diagn
Cytopathol 2009; 37:21-9. [PMID: 18973122]
- Schneider AR, Nerlich A, Topalidis T, Schepp W. Specialized clinical
cytology may improve the results of EUS (endoscopic ultrasound)-guided
fine-needle aspiration (FNA) from pancreatic tumors. Endosc Int Open
2015; 3:E134-7. [PMID: 26135655]




