Keywords
Immunoglobulin G; Pancreatitis; Retroperitoneal Fibrosis
Abbreviations
AIP autoimmune pancreatitis; CP chronic pancreatitis; IDCP idiopathic duct-centric pancreatitis; NOS not otherwise specified
INTRODUCTION
An inflammatory pancreatitis was described for the first time by Henri Sarles in 1961[1], but it was only in 1995 when the terminology of autoimmune pancreatitis (AIP) was used [2] and in 2003 when the concept of IgG4 related disease was widely accepted [3]. Later on, a second type of AIP was described, which received the name of type 2 or Idiopathic Duct-Centric Pancreatitis (IDCP), [4, 5, 6, 7, 8]. While different in several aspects, this type of disease also responds to steroid treatment. It is rare in Asia [9], somewhat more frequent in USA [4, 6].
Autoimmune factors play an important role even in the widely accepted TIGAR-O [10] classification system, where the “A” refers to “autoimmune” etiology. However, it seems to be quite different entity and unrelated to IgG4. For example, chronic pancreatitis (CP) was described in relation to systemic lupus erythematosus [11], but pancreatitis was rarely found in patients with autoimmune diseases [4]. AIP has a characteristic clinical course, radiologic findings, histology and prognosis. However, CP can be the late result of AIP and AIP continues to be accepted as a class of CP.
A lot of papers have been published on this disease from Asia, Europe and United States. However, from Latin America, major experiences were reported only from Mexico [12], and there are some case reports from Argentina [13], Peru [14, 15, 16], Brazil [17, 18] and Colombia [19]. We published our initial experience with 10 patients in 2010 [20]. In this paper we compare our experience to the observations published from other regions of the world, and evaluate difficulties in the diagnosis and classification of AIP in the daily clinical practice. The regular follow-up of our patients permits to evaluate the late outcome of this disease and its relation to the classic CP.
PATIENTS AND METHODS
We reviewed clinical files of patients treated between 1999 and 2017 with diagnosis of AIP in two tertiary hospitals with regular follow up by pancreatologists. The initial diagnosis was revised according to the International Consensus Diagnostic Criteria [21] at the moment of this analysis, and they were classified as type 1 and type 2 AIP. If the diagnosis of AIP was established but no definitive classification was possible, they were considered as Not Otherwise Specified - NOS [22]. The patient was later on reclassified if new data made it possible (e.g. posterior appearance of inflammatory bowel disease or other IgG4 related disease). Demographic characteristics, clinical findings, laboratory tests, imaging studies and other organ involvements were registered. IgG4 serum level was not measured in 14 patients, which occurred mainly in the initial period. Later on, IgG4 was routinely checked at the moment of diagnosis and during the follow-up using an upper cut-off limit of 135 mg/dl [23].
Histology was obtained from surgical specimens of resected pancreas (n=7), fine needle aspiration (FNA) by endosonography (n = 5), endoscopic biopsy from the papilla of Vater (n=8) and histology of other involved organs such as lymph nodes (n=2) and stomach biopsy (n=1).
Patients were treated with oral prednisone in a dose of 0.5-0.6 mg/kg body weight per day and controlled at the 3rd week to confirm the initial response to the treatment. After the 4th week, the prednisone dose was tapered by 5 mg every 2 weeks and suspended after 4-6 months. Morphological recovery of the pancreas was confirmed by magnetic resonance (MR).
The patients were regularly followed by pancreatologists in the outpatient center of both institutions and contacted by phone at the time of the conducting this study. The follow-up period was 4.1 ± 4.17 years (range 1 to 18 years, 10 of them for more than 10 years). They were monitored clinically, and with laboratory tests. MR was made on suspicion of recurrence of the disease, even if the IgG4 related disease recurred in other organ. In these cases oral steroid therapy was repeated and 1-1.5 mg/kg/day Azathioprine was added and continued for several years. Rituximab has not been used yet in our group.
Ethics: The retrospective analysis of the clinical files and the project was approved by Committee of Ethics in both institutions.
Statistical Analysis
Basic descriptive statistics were obtained including mean, median and standard deviation (SD) for continuous variables.
RESULTS
Data were collected from 83 patients diagnosed with AIP between 1999 and August 2017. Nine of them were excluded from this analysis for incomplete data (n=1) or lost for follow-up (n=8). Finally, 74 patients were included, of which 48 were men and 26 women, mean age 45.4 ± 17 years. All patients had characteristic imaging features, responded quickly to steroid treatment. According to the ICDC, 44 patients were categorized as type 1 AIP, 10 patients as type 2 and 20 patients as AIP- NOS (Figure 1).
Figure 1: Flow-chart of the patients analyzed. For demographic and other clinical details see Table 1.
Classification as type 1 AIP was confirmed by increased IgG4 serum level (n=24), by histological findings in the resected pancreas (n=7), or involvement of other organs (n=29). All patients classified as type 2 AIP had ulcerative colitis, at the time of the AIP diagnosis or later (n=10). The remaining patients were classified as NOS (Table 1). AIP was increasingly diagnosed after 2010 (Figure 2). Type 2 and NOS patients had normal IgG4 serum levels and fulfilled the other criteria of AIP, but pancreatic biopsy was not done. Cytology of involved pancreatic tissue was obtained in some cases (n=4) by FNA.
Figure 2: Diagnosis of AIP in different 5 years periods. Only some cases of type 1. disease were recognized in the first period, followed by a marked increase in time, by the appearance of type 2. and NOS patients. The proportion of NOS is the highest in the recently observed cases, several of them probably will be determined during the follow-up as type 1 or 2.
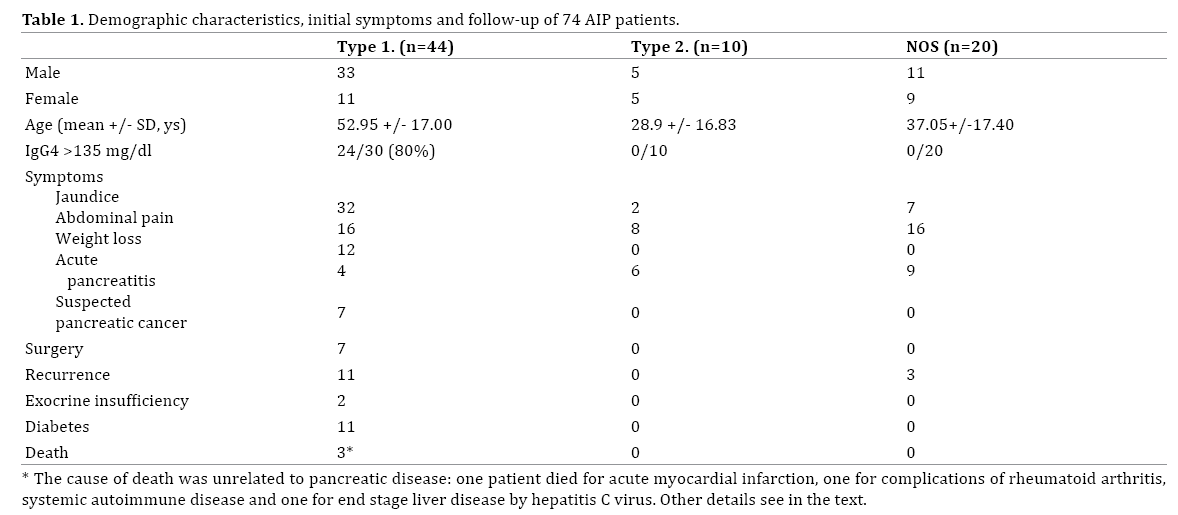
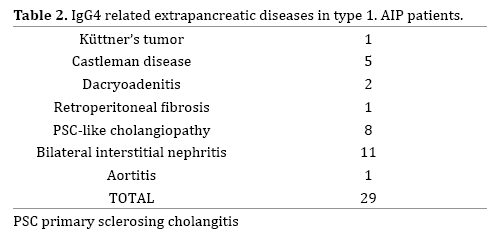
In type 1 AIP (n=44), the main initial symptom was jaundice (n=32), followed by abdominal pain (n=16), weight loss (n=12), and mild acute pancreatitis (n=4). In type 2 (n=10) and NOS (n=20) AIP, the leading symptom was abdominal pain in (n=8 and 16, respectively) followed by jaundice, also frequent in these groups (Table 2). Other organs were involved in 29 patients with type 1 AIP. The most frequent extrapancreatic IgG4 related manifestations were bilateral nephritis (n=11), sclerosing cholangitis-like cholangiopathy (n=8) and Castleman disease (n=5). Other, non IgG4 related autoimmune diseases were also found (n=8). All 10 patients with type 2 AIP had ulcerative colitis. In NOS AIP, one patient had hypothyroidism.
MR of pancreas was done in all patients and in most of them also CT scan was performed as first radiologic examination. The pancreatic involvement was diffuse in 27 of 44 type 1 patients, in 2 of 10 type 2 and in 4 of 20 NOS patients. Focal tumor-like lesion was found in 17 of type 1 AIP (11 head, 6 tail) and 2 of 10 type 2 AIP patients. In 16 of the NOS group, the disease affected only partially the pancreas (7 head, 9 body and tail), but the involvement of the affected segment was diffuse, without tumor-like lesion.
ERCP was performed in 12 patients, 10 of them for obstructive jaundice with stent placement. Pancreatic resection (6 head and 1 tail) was performed in 7 type 1 AIP patients, always for diagnostic doubts, 6 of these surgeries were carried out before 2010. No surgery was performed in type 2 and NOS group. Histology of surgical pancreatic tissue showed lymphoplasmacytic infiltrate, storiform fibrosis and venulitis, characteristic features of lymphoplasmacytic sclerosing pancreatitis (LPSP). Biopsies from the papilla of Vater showed nonspecific lymphoplasmocytic infiltrate, immunostaining for IgG4 was positive in 4 of 5 cases when it was applied. In 2 type 2 and 2 NOS patients, cytology was obtained by EUS guided FNA, showing only slight to moderate non-specific lymphoplasmocytic infiltration and no malignancy.
Treatment and Follow-Up
Four of the 40 patients with Type 1. AIP did not receive steroids, all of them had pancreatic resection. All but one surgical resection was performed only in the initial period, all patients had type 1. AIP. All the others had a complete recovery after receiving corticosteroid therapy, they responded quickly to steroids, independently of the subgroup. Post-treatment relapse observed in 11 of 44 patients with type 1 AIP which occurred after a symptom free period, and it was observed also in 3 of the 20 patients with NOS-AIP. There was no relapse in the type 2 AIP group. Of the patients who relapsed, 5 received prednisone associated with azathioprine, in the remaining 9 (6+3), a new course of prednisone alone was given. Recurrence occurred between 5 and 12 months after the suspension of first therapy. No recurrence occurred after pancreatic resection in this group. During followup, 11 patients developed diabetes, 6 of them requiring insulin. In 2 patients exocrine pancreatic insufficiency was demonstrated by low fecal elastase level during the followup, they were treated with oral pancreatic enzymes. One patient developed classical CP, with calcifications and intraductal stones 6 years after the initial episode and 3 years after a relapse. In most cases the functional and morphological recovery was complete, except for a certain degree of atrophy in the involved pancreatic segment in some patients. The functional recovery was confirmed by normal fecal elastase test, regular control of blood glucose and hemoglobin A1c level. We have not observed functional sequela or recurrence in type 2 AIP. Of the total group, there were 3 deaths, none of them related to pancreatic disease. None of our patients has developed neither pancreatic nor extrapancreatic malignancy till now.
Late outcome was worse in type 1 AIP: More frequent recurrence and permanent functional damage, and the only advanced chronic pancreatitis with calcifications was observed in this subgroup. In contrast, we have not observed functional sequela or recurrence in type 2. AIP and only three relapses in NOS AIP patients, with a complete recovery after repeated steroid treatment.
DISCUSSION
After several case reports, our descriptive, retrospective study is the first analysis of major experiences on AIP from South America. The prevalence of AIP is not known: it was estimated about 4.6/100.000 in Japan [9], with predominance of type 1, while the incidence was estimated in about 0.29/100.000/yr in a study published from Germany [24], being considered as a relatively rare disease also in Spain [25]. Type 2 was also rare in Korea [26], UK [27] and Hungary [28]. In a study of Schneider et al, no cases of AIP were found in patients with chronic alcoholic pancreatitis but autoimmune etiology was considered probable in 9% of non-alcoholic CP [24]. In our group, AIP has been diagnosed in the last years with a frequency similar to that of CP, which is considered a relatively rare disease in Chile [29]: 69 of our patients with AIP were seen after 2006 vs. 87 CP cases seen in the same period. Following our AIP patients with regular clinical, laboratory controls and even images if necessary, we found the progression to chronic pancreatitis in one exceptional case. On the other hand, only in 3 of our 121 CP cases we could detect some autoimmune factors [29], including also the present patient. These facts also supports our opinion: AIP cannot be considered simply as a subclass of CP [30]. In the worldwide accepted TIGAR-O classification [10], clinical characteristics, progressive evolution of pancreatic damage and even histology are very similar in toxic (T), idiopathic (I), genetic (G) etiologies and even in the recurrent (R) form, demonstrating that it is the same disease. However, obstructive (O) pancreatitis is considered as a separate entity in this classification, for its differences in the histology and the capacity to recover even completely, once the obstruction resolved. We think, that AIP is quite different if we compare to classic CP: on the basis of clinical characteristics, complete recovery in response to steroids, lack of exocrine and endocrine insufficiency and even its histology, we suggest that it should be considered as a distinct entity. While AIP patients do require regular control with gastroenterologist including pancreatic exocrine and endocrine function, this control must be focused on the eventual recurrence of the disease and search for involvement of other organs.
Type 1 AIP has been found dominant in Asia and type 2 almost exceptional [9, 26]. Almost exclusively type 1 was published in UK [27] and 3 type 2 were observed in 17 Hungarian cases [28]. Also in Spain, 45 of 52 patients were type 1 and only 5 of them type 2 [25]. Our experiences are similar to well-known literature data in several aspects: type 1 AIP was markedly more frequent, with similar demographic characteristics and excellent rapid response to steroid treatment, with a tendency to recurrence in about 25-30%. While the diagnosis of type 1. AIP has been established in the majority of cases without histology of pancreas, this classification was definitely confirmed by other criteria, as increased IgG4 serum level and/or other organ involvement by the IgG4 related disease. On the contrary, the only proof for type 2 AIP in our experience was the association with inflammatory bowel disease (IBD), in particular with ulcerative colitis (UC). We did not obtain histology of pancreas, because the cytology obtained by FNA via endosonography has a limited value in the diagnosis of AIP [31] and it is not without risk. Thus, the diagnosis of type-2 AIP in our material could be questionable in some cases, as it was shown in the recent national study from Japan [32]. In the future, improvement in the EUS biopsy needles [33, 34] can increase the diagnostic performance and histology hopefully will be available without elevated risk for the diagnosis of AIP, in particular for type 2. However, clinical characteristics of our patients considered as probable type 2-AIP were similar to those described elsewhere in the world: no gender difference, markedly younger age, no recurrence, normal serum IgG4 and rapid and complete response to steroids.
Our experience is consistent with the existence of significant differences between type 1 and type 2. AIP, both in clinical characteristics and outcome, but not in radiological findings and in steroid responsiveness, which are similar in both groups. We found some differences in the distribution but not in the character of morphological alterations detected by MRI: diffuse involvement of the pancreas and mass-forming lesions were considerably more frequent in type 1, but the parenchymal alterations and duct stricture were common in the three subgroups. In absence of increased IgG4 level or other diagnostic criteria, distinguish LPSP and IDCP at the moment of initial presentation is very difficult, almost impossible. In addition, there are several cases, when the clinical classification in type 1 or 2 is not possible, for this eventuality appeared a third, undetermined class, denominated as No Otherwise Specified (NOS) [22]. This subclass of AIP is probably a mixture of type 1 and 2 patients, without sufficient information to achieve a definitive classification. We found the NOS-AIP category useful for the clinical practice for the patients when the diagnosis of AIP was established with strong probability by other criteria – radiology and response to steroid - but without elevated IgG4 nor other organ involvement, as a consequence, the classification remained undetermined. Some of our patients were reclassified during follow-up.
While some spontaneous improvement does exist in this disease, complete recovery is far more frequent and even the late prognosis is better if the patient receive an adequate treatment [35]. The question is, which is the adequate treatment? [21, 36]. In our practice, steroid treatment was used in all patients as described. After recurrence or after association of other IgG4 related disease, we added Azathioprine and maintained its use for several years. Some groups argue in favor of maintenance steroid therapy: less relapse was seen if a low dose of 5 mg/day was maintained for two years [37]. However, about 70% of our type 1 patients, all patients with the type 2 AIP and 17 out of 20 NOS class had no relapse without maintenance treatment and we agree that the treatment must be individually tailored [38]. We did not observe recurrence after surgical resection of pancreas, even in the four cases without steroid treatment. However, the small number of the operated patients does not permit any conclusion and the surgery is certainly not the recommended treatment for AIP.
On the other hand, there are several doubts regarding the prognosis and late outcome of this disease. The likelihood of progressing to CP has been widely discussed. Biliary stenting by ERCP [39] and significant focal stenosis of main pancreatic duct [40] were found as risk factors for formation of pancreatic stones. In fact, we saw one exceptional patient with chronic calcifying pancreatitis and pancreatic ductal stones, who has previously undergone an ERCP when a suprapapillary stenosis of pancreatic duct was found, which disappeared after posterior steroid treatment. After the recovery, we observed diabetes somewhat more frequently (n=11) while overt exocrine insufficiency was detected only in 2 patients. Increased risk of pancreatic and even extrapancreatic cancer was published after AIP [41] but it was not confirmed by others [42]. No malignant tumors have been observed in our group.
Our study has several limitations. First of all, it is a retrospective study. We did not search for a histologic diagnosis in AIP. Obviously, the risks to obtain histology specimen of the pancreas is relatively elevated and the cytology has limited value. Thus, in contrast to our 44 type 1. patients, the classification of type 2 and NOS remains always a somewhat uncertain in our patients. The strength of our experience is in the relatively large number of patients who fulfilled all the other diagnostic criteria and in the long and regular follow-up.
CONCLUSION
AIP is a relatively new disease, we recognize it with a rapidly increasing frequency. Our experiences, until now the biggest in South America, show similar observations than in the rest of the world. The excellent and rapid response to steroid treatment permits to avoid unnecessary endoscopic and surgical interventions. Late prognosis is good, progression to advanced chronic pancreatitis is exceptional, significant endocrine and exocrine insufficiency is rare and no associated malignant disease was observed. When compared to CP, the morphology, clinical characteristics and late outcome of AIP are clearly different. In our experience, progression to CP can be avoided by treatment, regular follow-up and repeated treatment of recurrences.
Conflict of Interest
The authors do not have conflict of interest.
References
- Sarles H, Sarles JC, Muratore R, Guien C. Chronic inflammatory sclerosis of the pancreas: an autonomous pancreatic disease? Am J Dig Dis 1961; 6: 688-98. [PMID: 13746542]
- Yoshida K, Toki F, Takeuchi T, Watanabe S, Shiratori K, Hayashi N. Chronic pancreatitis caused by an autoimmune abnormality. Proposal of the concept of autoimmune pancreatitis. Dig Dis Sci 1995; 40: 1561-8. [PMID: 7628283]
- Kamisawa T, Funata N, Hayashi Y, Eishi Y, Koike M, Tsuruta K, et al. A new clinicopathological entity of IgG4-related autoimmune disease. J Gastroenterol 2003; 38:982-4. [PMID: 14614606]
- Chari ST. Diagnosis of Autoimmune Pancreatitis: The evolution of diagnostic criteria for a rare disease. Clin Gastroenterol Hepatol 2017; 15:1485-1488. [PMID: 28634132]
- Zhang L, Chari S, Smyrk TC, Deshpande V, Klöppel G, Kojima M, et al. Autoimmune Pancreatitis (AIP) Type 1 and Type 2. An International Consensus Study on Histopathologic Diagnostic Criteria. Pancreas 2011; 40: 1172-9. [PMID: 21975436]
- Hart PA, Levy MJ, Smyrk TC, Takahashi N, Abu Dayyeh BK, Clain JE, et al. Clinical profiles and outcomes in idiopathic duct-centric chronic pancreatitis (type 2 autoimmune pancreatitis): the Mayo Clinic experience. Gut 2016; 65:1702–1709. [PMID: 26085439]
- Lorenzo D, Maire F, Stefanescu C, Gornet JM, Seksik P, Serrero M, et al. Features of autoimmune pancreatitis associated with inflammatory bowel diseases. Clin Gastroenterol Hepatol 2018; 16:59-67. [PMID: ]
- Kim JW, Hwang SW, Park SH, Song TJ, Kim MH, Lee HS, et al. Clinical course of ulcerative colitis patients who develop acute pancreatitis. World J Gastroenterol 2017; 23:3505-3512. [PMID: 28596686]
- Kanno A, Masamune A, Okazaki K, Kamisawa T, Kawa S, Nishimori, I et al. Nationwide epidemiological survey of autoimmune pancreatitis in Japan in 2011. Pancreas 2015; 44:535-9. [PMID: 25815647]
- Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology 2001; 120:682-707. [PMID: 11179244]
- Li Z, Xu D, Wang Z, Wang Y, Zhang S, Li M, et al. Gastrointestinal system involvement in systemic lupus erythematosus. Lupus 2017; 26:1127-1138. [PMID: 28523968]
- Bourlon MT, Bourlon C, Atisha-Fregoso Y, Chable-Montero F, Teliz MA, Angeles-Angeles A, et al. Clinical and immunopathologic profile of Mexican patients with IgG4 autoimmune pancreatitis. ISRN Rheumatol 2012; 2012:164914. [PMID: 22666608]
- Blejter J, Weller S, Pace R, Cusumano H, Giambini D. Autoimmune pancreatitis: an adolescent case and review of literature. J Pediatr Surg 2008; 43:1368-72. [PMID: 18639699]
- Barreda F, Contardo C, León A, Navarrete J, Figueroa R, Attanasio F. Primary sclerosing cholangitis associated with Sjögren's syndrome, retroperitoneal fibrosis and chronic pancreatitis. Report of a case. Rev Gastroenterol Peru 1989; 9:106-14. [PMID: 2519235]
- Bellido-Caparó A, Espinoza-Ríos J, Aguilar V, García C, Pinto JL, Tagle Arróspide M, et al. Autoimmune pancreatitis type 1: a case report. Rev Gastroenterol Peru 2017; 37:254-7. [PMID: 29093590]
- Donet JA, Czul F, Peña NA, Barkin JS. Type 1 autoimmune pancreatitis: case scenario and review of the disease. Rev Gastroenterol Peru 2016; 36:252-255. [PMID: 27716763]
- Chebli JMF, Chebli LA, Ribeiro TCDR, Gaburri PD. Severe hypoproteinemia as a harbinger of Ménétrier’s disease in autoimmune pancreatitis. Rev Assoc Med Bras 2017; 63:215-218. [PMID: 28489125]
- Geraldino GC, Polizelli DV, Pedroso CL, de Toledo RA, Bertazzi GR, de Toledo RA, et al. Systemic lupus erythematosus presenting as autoimmune parotitis and pancreatitis - Case Report. Acta Reumatol Port 2010; 35:241-243. [PMID: 20734546]
- Rueda JC, Duarte-Rey C, Casas N. Successful treatment of relapsing autoimmune pancreatitis in primary Sjögren's syndrome with rituximab: report of a case and review of the literature. Rheumatol Int 2009; 29:1481-5. [PMID: 19137434]
- Muñoz S, Mancilla C, Moyano L, Castillo C, Rossi R, Brahm J, Berger Z. Autoimmune pancreatitis. Report of 10 cases. Rev Med Chile 2010; 138:295-302. [PMID: 20556331]
- Shimosegawa T, Chari S, Frulloni L, Kamisawa T, Kawa S, Mino-Kenudson M et al. International consensus diagnostic criteria for autoimmune pancreatitis: guidelines of the International Association of Pancreatology. Pancreas 2011; 40: 352-358. [PMID: 21412117]
- Ikeura T, Manfredi R, Zamboni G, Negrelli R, Capelli P, Amodio A, et al. Application of international consensus diagnostic criteria to an Italian series of autoimmune pancreatitis. UEG Journal 2013; 1:276-284. [PMID: 24917972]
- Yu KH, Chan TM, Tsai PH, Cheng CH, Chang PY. Diagnostic Performance of serum IgG4 levels in patients with IgG4-related disease. Medicine 2015; 94:e1707. [PMID: 26469909]
- Schneider A, Michaely H, Weiss C, Hirth M, Rückert F, Wilhelm TJ, et al. Prevalence and incidence of autoimmune pancreatitis in the population living in the Southwest of Germany. Digestion 2017 Sep 29; 96:187-198. [PMID: 28957814]
- López-Serrano A, Crespo J, Pascual I, Salord S, Bolado F, del-Pozo-García AJ, et al. Diagnosis, treatment and long-term outcomes of autoimmune pancreatitis in Spain based on the International Consensus Diagnostic Criteria: A multi-center study. Pancreatology 2016; 16:382-390. [PMID: 26944001]
- Kamisawa T, Ryu JK, Kim MH, Okazaki K, Shimosegawa T, Chung JB. Recent Advances in the Diagnosis and Management of Autoimmune Pancreatitis: Similarities and Differences in Japan and Korea. Gut Liver 2013; 7: 394-400. [PMID: 23898377]
- Church NI, Pereira SP, Deheragoda MG, Sandanayake N, Amin Z, Lees WR, et al. Autoimmune pancreatitis: clinical and radiological features and objective response to steroid therapy in a UK series. Am J Gastroenterol 2007; 102:2417-25. [PMID: 17894845]
- Czakó L, Gyökeres T, Topa L, Sahin P, Takács T, Vincze A, et al. Autoimmune pancreatitis in Hungary: a multicenter nationwide study. Pancreatology 2011; 11:261-7. [PMID: 21625197]
- Berger Z, Mancilla C. Chronic pancreatitis. Retrospective review of 121 cases. Rev Med Chile 2016; 144:1544-1552. [PMID: 28393988]
- Berger Z, Mancilla C. Is autoimmune pancreatitis a subclass of chronic pancreatitis? Pancreatology 2016; 17: 55. [PMID: 28034552]
- Morishima T, Kawashima H, Ohno E, Yamamura T, Funasaka K, Nakamura M, et al. Prospective multicenter study on the usefulness of EUS-guided FNA biopsy for the diagnosis of autoimmune pancreatitis. Gastrointest Endosc 2016; 84:241-8. [PMID: 26777565]
- Kawa S, Okazaki K, Notohara K, Watanabe M, Shimosegawa T and Study Group for Pancreatitis Complicated with Inflammatory Bowel Disease: Autoimmune pancreatitis complicated with inflammatory bowel disease and comparative study of type 1 and type 2 autoimmune pancreatitis. J Gastroenterol 2015; 50:805-15. [PMID: 25399203]
- Runge TM, Hart PA, Sasatomi E, Baron TH. Diagnosis of autoimmune pancreatitis using new, flexible EUS core biopsy needles: report of 2 cases. Gastrointest Endosc 2017; 85:1311-1312. [PMID: 28522022]
- Kerdsirichairat T, Saini, SD, Chamberlain PR, Prabhu A. Autoimmune Pancreatitis Diagnosed with Core Biopsy Obtained from a Novel Fork-Tip EUS Needle. ACG Case Rep J 2017; 4:e7. [PMID: 28144612]
- Hirano K, Tada M, Isayama H, Yagioka H, Sasaki T, Kogure H et al. Long-term prognosis of autoimmune pancreatitis with and without corticosteroid treatment. Gut 2007; 56:1719–1724. [PMID: 23232048]
- Okazaki K, Chari ST, Frulloni L, Lerch MM, Kamisawa T, Kawa S et al. International consensus for the treatment of autoimmune pancreatitis. Pancreatology 2017; 17: 1-6. [PMID: 28027896]
- Masamune A, Nishimori I, Kikuta K, Tsuji I, Mizuno N, Iiyama T, et al. Randomised controlled trial of long-term maintenance corticosteroid therapy in patients with autoimmune pancreatitis. Gut 2017; 66:487–494. [PMID: 27543430]
- Frulloni L, de Pretis N, Amodio A. Maintenance therapy in autoimmune pancreatitis: a weak light into the darkness. Ann Transl Med 2017; 5:367. [PMID: 28936461]
- Matsubayashi H, Kishida Y, Iwai T, Murai K, Yoshida M, Imai K. Transpapillary biliary stenting is a risk factor for pancreatic stones in patients with autoimmune pancreatitis. Endosc Int Open 2016; 04: E912–E917. [PMID: 27540582]
- Maruyama M, Arakura N, Ozaki Y, Watanabe T, Ito T, Yoneda S, et al. Risk factors for pancreatic stone formation in autoimmune pancreatitis over a long-term course. J Gastroenterol 2012; 47:553–560. [PMID: 22183858]
- Shiokawa M, Kodama Y, Minami R, Sakuma Y, Kuriyama K, Ota Y, et al. Risk of cancer in patients with autoimmune pancreatitis. Am J Gastroenterol 2013; 108: 610–617. [PMID: 23318486]
- Hart PA, Law RJ, Dierkhising RA, Smyrk TC, Takahashi N, Chari ST. Risk of cancer in autoimmune pancreatitis: a case-control study and review of the literature. Pancreas 2014; 43:417–421. [PMID: 24622072]



