Christine Thang1, Margaret Whitley2, Nilufar Izadpanah3, Daniel DeUgarte1 and Wendy Slusser1,4*
1Mattel Children's Hospital University of California Los Angeles, Los Angeles, California, USA
2RAND Corporation, Santa Monica, CA, USA
3California State University Northridge, Northridge, California, USA
4University of California Los Angeles Fielding School of Public Health, Los Angeles, California, USA
*Corresponding Author:
Wendy Slusser
Department of Pediatrics, Mattel Children's Hospital University of California Los Angeles
2231 Murphy Hall, Los Angeles, CA-90095-1405
Tel: 310- 825-6575
E-mail: WSlusser@mednet.ucla.edu
Received date: December 27, 2016; Accepted date: January 30, 2017; Published date: February 02, 2017
Citation: Thang C, Whitley M, Izadpanah N, DeUgarte D, Slusser W (2017) Barriers and Comorbidities from A Pediatric Multidisciplinary Tertiary Care Obesity Program. J Child Obes 2:2. doi: 10.21767/2572-5394.100025
Copyright: © 2017 Thang C. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Morbid obesity; Hypertension; Multidisciplinary clinic
Abbreviations
ALT: Alanine Aminotransferase; AST: Aspartate Aminotransferase; BMI: Body Mass Index; BP: Blood Pressure; HbA1c: Hemoglobin A1c; HDL: High-Density Lipoprotein; LDL: Low-Density Lipoprotein; SD: Standard Deviations
Introduction
The prevalence of childhood obesity in the United States remains high, with 17% of children reported as obese [1] and with associated higher risks of developing diabetes, cardiovascular disease, depression, gastrointestinal conditions, musculoskeletal problems, poor school performance, and disability [2-6]. Socioeconomic, ethnic, and racial disparities exacerbate the emergence of comorbid conditions [7]. Studies have identified psychosocial and familial factors as barriers to healthy weight management, highlighting the importance of addressing psychosocial well-being when managing pediatric obesity [8].
Higher BMI levels are associated with elevated BP and cardiovascular risk. The rate of progression from prehypertension (90th-95th percentile) to hypertension (>95th percentile) among children occurs at approximately 7-10% annually [9,10]. If preventive measures through healthy eating and physical activity are implemented to modify BP early among high-risk obese children, this may limit the progression to hypertension and cardiovascular disease. However, few effective interventions have been reported to improve dietary and physical activity habits among high-risk obese children [11].
The UCLA Fit for Healthy Weight Clinic (Fit Clinic) is a multidisciplinary tertiary weight management program that focuses on treating overweight and obese pediatric patients who have not met their healthy weight goals under the care of their primary care providers [12]. The multidisciplinary team following the American Academy of Pediatrics (AAP) Expert Committee Recommendations, consists of a general pediatrician, registered dietitian, and clinical psychologist. The Fit Clinic team identifies and addresses the patients’ barriers to healthy diet, physical activity, and emotional well-being, utilizing motivational interviewing strategies and different perspectives of healthcare. The purpose of this study was to identify the characteristics, comorbidities, and barriers to health for the morbidly obese pediatric patients seeking care at the Fit Clinic.
Methods
This study was approved by the University of California, Institutional Review Board.
The fit clinic
The Fit Clinic utilizes a multidisciplinary team approach consisting of a general pediatrician with a specialty in nutrition, a registered dietitian, and a clinical psychologist. There is also a pediatric surgeon on staff available to patients interested in exploring bariatric surgery. Patients referred to the clinic by their primary care providers are not making progress under their current primary care, and many have exhausted other strategies of weight control. During each Fit Clinic visit, all three healthcare providers individually rotate through to evaluate and counsel each patient. A patient’s medical, dietary, psychological, social, developmental, family, and physical activity histories are elicited and reviewed, and a full physical examination is conducted. A registration form (fitprogram.ucla.edu) aids in the collection of this information.
Providers utilize treatment strategies that include nutritional and psychological education, motivational interviewing, counseling, and behavior intervention therapies targeted at improving daily routines, emotional health, diet, and physical activity. Motivational interviewing is the major strategy, utilizing a patient-centered approach that helps establish the foundation for subsequent goal setting [13]. The patient and family identify lifestyle modifications and quantify their level of confidence in reaching them. The team will reflect and summarize both verbally and in writing the lifestyle modifications.
The individualized behavior change goals for healthy eating, physical activity, emotional wellbeing, and family support are then followed up at subsequent monthly visits. Healthy eating goals often focus on hunger management, portion control, decreasing sugar-based beverage intake, increasing fruit and vegetable intake, and modifying eating behaviors [12]. Healthy physical activity goals are structured to increase daily activity from often a baseline sedentary level.
The healthy emotional wellbeing goals focus on anxiety, psychosocial stressors, and emotional eating. Following the multidisciplinary discussions, one to two healthy eating, physical activity, emotional wellbeing, and family goals are selected and followed up at subsequent visits. Appropriate medical referrals are also made including sleep studies to rule out obstructive sleep apnea, an often under-diagnosed co-morbid condition [14].
Study design and patient demographics
A retrospective medical chart review was conducted of 115 patients enrolled in the Fit Clinic. Eligible subjects were boys and girls, 3 to 22 years of age with BMI over 85%, seen at the Fit Clinic between April 2008 and October 2011. Self-identified (by the parent or patient, depending on the age) comorbidities and barriers that prevented the patient from engaging in physical activity and healthful eating were documented, assessed, and discussed with the pediatrician. After the initial evaluation, patients had follow-up appointments with the Fit Clinic multidisciplinary team scheduled at approximately one-month intervals. Anthropometric and blood pressure data were collected in clinical charts at each visit. Of note, no changes were made to already existing hypertensive pharmaceutical regimens among patients in this study sample.
Collection of data and classification of clinical outcomes
Height, weight, BP, and when available, laboratory data were abstracted from patient medical records. Baseline laboratory values were not available for all Fit Clinic patients since they were ordered based on clinical judgment and protocols and not for research purposes. Barriers to physical activity and healthy eating were abstracted from the baseline registration forms. BMI was calculated as weight in kilograms divided by height in meters squared (kg/m2).
BMI of ≥ 85th – 94th percentile for age and gender was classified as “overweight” and ≥ 95th percentile was defined as “obese” [12]. BP values were categorized using national data from the Centers for Disease Control and the National Heart, Lung and Blood Institute Task Force on Blood Pressure Control in Children [10]. Abnormal fasting lipid levels were based on values recommended by the AAP [15].
Abnormal fasting blood glucose was based on the American Diabetes Association and the International Expert Committee recommendations [15-17].
Statistical analysis
Statistical analysis was completed using STATA software. Descriptive statistics were calculated for all variables. The paired t-test was used to assess for differences among clinical measures at baseline and after a number of clinic visits.
Results
Baseline characteristics of fit clinic patients
The sample included 115 Fit Clinic patients enrolled during the study interval. The mean number of clinic visits was three with an average of one month between visits. The mean age at the first visit was 13 years old. The number of males (49.6%) and females (50.4%) were near equal.
Average baseline BMI was 34 with a mean percentile of 98%. Among all patients, 97% were categorized as obese based on BMI, and 30% were classified as pre-hypertensive or hypertensive based on their blood pressures.
Abnormal total cholesterol level >200 mg/dl was observed in 19 (24%). 33% of patients had borderline to elevated LDL, 43% of patients had abnormal, or low, HDL levels, and 54% of patients had elevated triglycerides.
Six patients (8%) had borderline elevated fasting glucose levels (100-125 mg/dl). Seven (12%) had elevated hemoglobin A1c. AST and ALT were above normal in 8% and 17% of children, respectively.
Comorbidities and barriers to healthful eating and physical activity
An average of 5.8 comorbid systems was identified at the first clinic visit. Among the more frequently listed comorbidities were those related to gastrointestinal (32%), respiratory (36%), psychiatric (41%), ears/nose/mouth/throat (50%), cardiovascular (52%), endocrine (70%), skin (79%), and constitutional (fever, night sweats, chills, fatigue, weight change) (97%).
The most commonly identified barriers to healthy eating were lack of self-discipline (63%), that dieting “is hard work” (55%), and dislike of healthy foods (30%).
With respect to physical activity, the most commonly cited barriers were lack of self-discipline (41%), lack of someone to engage in physical activity with (38%), self-consciousness about appearance (33%), and lack of energy (28%).
Less than 10% of subjects selected lack of money, equipment, or time as barriers to healthy eating or physical activity.
Trends in BMI and BP
At initial evaluation, 100% of Fit Clinic patients had BMI values at or above the 85th percentile. Although there was no statistically significant decrease in BMI, there was an overall trend of a reduction or stabilization in BMI. The distribution of BMI for Fit Clinic patients is shown in Figure 1.
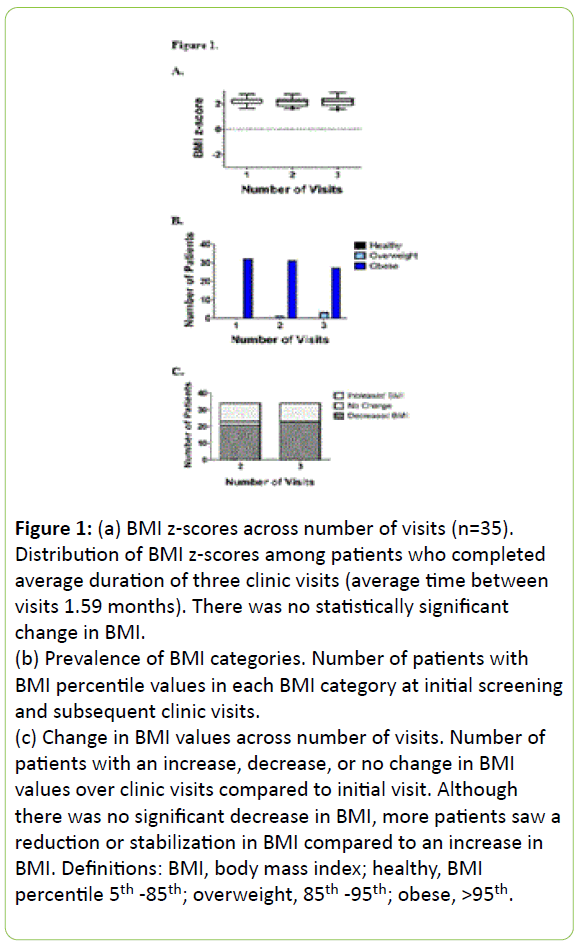
Figure 1: (a) BMI z-scores across number of visits (n=35). Distribution of BMI z-scores among patients who completed average duration of three clinic visits (average time between visits 1.59 months). There was no statistically significant change in BMI.
(b) Prevalence of BMI categories. Number of patients with BMI percentile values in each BMI category at initial screening and subsequent clinic visits.
(c) Change in BMI values across number of visits. Number of patients with an increase, decrease, or no change in BMI values over clinic visits compared to initial visit. Although there was no significant decrease in BMI, more patients saw a reduction or stabilization in BMI compared to an increase in BMI. Definitions: BMI, body mass index; healthy, BMI percentile 5th -85th; overweight, 85th -95th; obese, >95th.
Using the subset of patients who completed the average of three clinic visits, 26% of patients were outside the normotensive range. After three clinic visits, there was a significant improvement (p<0.05) in BP across these patients. It was noted that 82% of patients in the elevated BP category moved into the normotensive range.
Patients saw a reduction of their BP from the hypertensive to the pre-hypertensive category or to the normotensive range. No patients jumped into a higher BP category. Figure 2 illustrates BP outcomes among patients after three clinic visits.
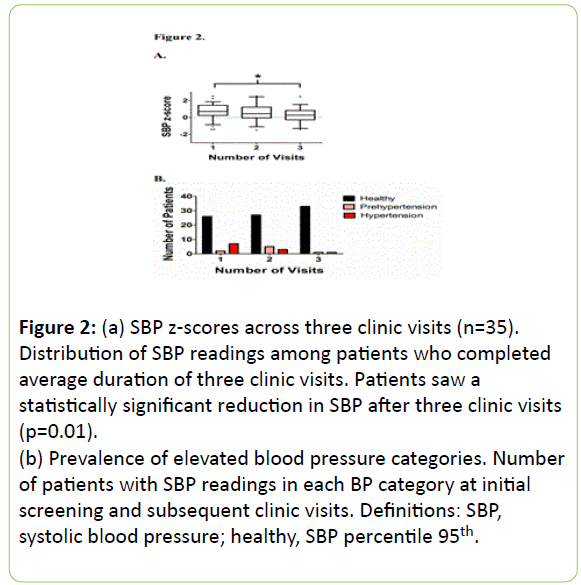
Figure 2: (a) SBP z-scores across three clinic visits (n=35). Distribution of SBP readings among patients who completed average duration of three clinic visits. Patients saw a statistically significant reduction in SBP after three clinic visits (p=0.01).
(b) Prevalence of elevated blood pressure categories. Number of patients with SBP readings in each BP category at initial screening and subsequent clinic visits. Definitions: SBP, systolic blood pressure; healthy, SBP percentile 95th.
Discussion
The preliminary data from this retrospective chart review of the Fit Clinic provides a glimpse into a cohort of overweight and obese children and adolescents whose efforts in weight management with their primary medical providers were unsuccessful. Multidisciplinary services are recommended for overweight and obese children and adolescents who do not stabilize or reduce their BMI in the primary care setting after 6-12 months of prevention-plus and structured weight management interventions [12]. The multidisciplinary treatment team, patient and family-centered approach, and behaviorallifestyle intervention and counseling are the components recommended by pediatric obesity researchers to curtail the growing pediatric obesity epidemic [11-12,18-20].
This report adds to the growing evidence that a multidisciplinary pediatric obesity clinic can impact overweight and obese patients. Other reports of clinical programs in the literature with comparable patient-centered approaches and multidisciplinary teams have reported similar overall small changes in BMI with reductions of 0.03 to 0.24 points [21-24]. Patients in the prehypertensive BP range have the most to benefit with respect to reversing the progression to hypertension and cardiovascular disease [25-28]. This report suggests that significant changes in BP can occur with small, even statistically non-significant changes in BMI. This may be attributed to personalized lifestyle modifications manifested in improved BPs preceding any change to BMI.
Although not every overweight or obese child is destined to become an overweight or obese adolescent or adult, it is recognized that pediatric obesity can precede adult obesity and can have adverse health consequences in adulthood related to premature mortality and cardiometabolic morbidity [29]. Abnormalities that begin in childhood precede many of the wellstudied obesity associated comorbidities in adulthood [30,31]. Many Fit Clinic patients already manifest known obesity related comorbidities as evidenced in self-reports and abnormal baseline laboratory values. Fit Clinic patients who average five obesity-related comorbidities already have more than what is reported in large U.S. population-based studies [5,30]. With an understanding of the association of obesity with other health conditions in childhood, pediatricians can better manage these patients by addressing additional factors beyond high BMI. Although not a random sample of the population, this cohort of morbidly obese pediatric patients nevertheless demonstrates that solely addressing BMI is not sufficient.
A multidisciplinary approach that incorporates a psychologist and nutritionist may prove to be the most beneficial option for obese pediatric patients to reach their healthy lifestyle goals. In a systematic review of the effectiveness of lifestyle interventions in childhood obesity, behavioral modifications in addition to diet changes were found to be essential elements in effective obesity management programs [32]. Patients attending the multidisciplinary Fit Clinic, which focuses on the commonly identified barriers to healthy diets and physical activity, exhibited successful trends in their BMI and BP. While lack of time and financial resources are often cited in the literature as impediments to healthy lifestyles, [7,33] psychological barriers are more commonly reported among Fit Clinic patients, including perceived lack of self-discipline and the challenges of lifestyle change. Whether pediatric patients lack awareness of socioeconomic factors in their lives compared to the adult population warrants further exploration.
Obesity has been recognized as a chronic disease that requires ongoing follow-up care [29]. Thus, it is important to evaluate the long-term success of pediatric weight management programs in mitigating the trajectory of pediatric obesity. Shortterm successes have been studied with noted improvements in weight and cardiometabolic outcomes [32]. The question arises whether positive effects can be sustained and followed into adulthood [34]. How pediatric obesity translates into and predicts adult morbidity and mortality is widely reviewed [29,31], but few studies exist that determine the long-term effectiveness of pediatric weight management and lifestyle intervention programs. This is probably due to difficulties in maintaining a cohort of pediatrics patients through adulthood.
The early successes of the Fit Clinic suggest the effectiveness of a tertiary care multidisciplinary approach at addressing barriers to healthy lifestyles. In tailoring its multifaceted approach to the unique needs of its patient population, the Fit Clinic has been successful in curtailing the progression of its patients toward unhealthy clinical outcomes. The Fit Clinic offers a promising intervention to decrease obesity rates and ameliorate disparities in pediatric obesity.
Acknowledgments
Thank you to Devoe Arnold, Chelsea Harman, and Virginia James who, as summer student interns, assisted in data entry.
References
- Ogden CL, Carroll MD, Kit BK, Flegal KM (2014) Prevalence of childhood and adult obesity in the United States, 2011-2012. JAMA 311: 806-814.
- Freedman DS, Khan LK, Dietz WH, Srinivasan SR, Berenson GS (2001) Relationship of childhood obesity to coronary heart disease risk factors in adulthood: the Bogalusa Heart Study. Pediatr 108: 712-718.
- Sinha R, Fisch G, Teague B, Tamborlane WV, Banyas B, et al. (2002) Prevalence of impaired glucose tolerance among children and adolescents with marked obesity. NEJM 346: 802-810.
- Weiss R, Dziura J, Burgert TS, Tamborlane WV, Taksali SE, et al. (2004) Obesity and the metabolic syndrome in children and adolescents. NEJM 350: 2362-2374.
- Slusser WM, Staten K, Stephens K, Liu L, Yeh C, et al. (2011) Payment for obesity services: Examples and recommendations for stage 3 comprehensive multidisciplinary intervention programs for children and adolescents. Pediatr 128: s78-s85.
- Halfon N, Larson K, Slusser W (2013) Associations between obesity and comorbid mental health, developmental and physical health conditions in a nationally representative sample of US children aged 10 to 17. Acad Peds 13: 6-13.
- Haas JS, Lee LB, Kaplan CP, Sonneborn D, Phillips KA, et al. (2003) The association of race, socioeconomic status, and health insurance with the prevalence of overweight among children and adolescents. Am J Public Health 93: 2105-2110.
- Porter JS, Bean MK, Gerke CK, Stern M (2010) Psychosocial factors and perspectives on weight gain and barriers to weight loss among adolescents enrolled in obesity treatment. J Clin Psychol Med Settings 17: 98-102.
- Kotchen TA (2010) Obesity-related hypertension: Epidemiology, pathophysiology, and clinical Management. Am. J. Hypertens 23: 1170-1178.
- National high blood pressure education program working group on high blood pressure in children and adolescents. (2004) The fourth report on the diagnosis, evaluation, and treatment of high blood pressure in children and adolescents. Pediatr 114: 555-576.
- O’Brien SH, Holubkov R, Reis EC (2004) Identification, evaluation, and management of obesity in an academic primary care center. Pediatr 114: e154-159.
- Barlow SE (2007) Expert committee recommendations regarding the prevention, assessment, and treatment of child and adolescent overweight and obesity: summary report. Pediatr 120: S164-S192.
- Sindelar HA, Abrantes AM, Hart C, Lewander W, Spirito A (2004) Motivational interviewing in pediatric practice. Curr Probl Pediatr Adolesc Health Care 34: 322-339.
- Shine NP, Harvey LC, Lannigan FJ (2005) Obstructive sleep apnea, morbid obesity, and adenotonsillar surgery: A review of the literature. Int J Pediatr Otorhinolaryngol 69: 1475-1482.
- Daniels SR, Greer FR (2008) Lipid screening and cardiovascular health in childhood. Pediatr 122: 198-208.
- American Diabetes Association. (2008) Diagnosis and classification of diabetes mellitus. Diabetes Care 31: S55-S60.
- Dolinksy DH, Armstrong SC, Walter EB (2012) The effectiveness of a primary care-based pediatric obesity program. Clinical Pediatr 51: 345-353.
- Quattrin T, Liu E, Shaw N, Shine B, Chiang E (2005) Obese children who are referred to the pediatric endocrinologist: Characteristics and outcome. Pediatr 115: 348-351.
- Nova A, Russo A, Sala E (2001) Long-term management of obesity in pediatric office practice: experimental evaluation of two different types of intervention. Ambul Child Health 7: 239-248.
- Sargent GM, Pilotto LS, Baur LA (2011) Components of primary care interventions to treat childhood overweight and obesity: a systematic review of effect. Obes Rev 12: e219-e235.
- Madsen KA, Garber AK, Mietus-Snyder ML, Orrell-Valente JK, Tran CT, et al. (2009) A clinic-based lifestyle intervention for pediatric obesity: efficacy and behavioral and biochemical predictors of response. J Pediatr Endocrinol Metab 22: 805-814.
- Skelton JA, DeMattia LG, Flores G (2008) A pediatric weight management program for high-risk populations: a preliminary analysis. Obesity 16:1698-1701.
- Denzer C, Reithofer E, Wabitsch M, Widhalm K (2004) The outcome of childhood obesity management depends highly upon patient compliance. Eur J Pediatr 163: 99-104.
- Sabin MA, Ford A, Hunt L, Jamal R, Crowne EC, et al. (2007) Which factors are associated with a successful outcome in a weight management program for obese children? J Eval Clin Pract 13: 364-368.
- Chen X, Wang Y (2008) Tracking of blood pressure from childhood to adulthood: a systematic review and meta-regression analysis. Circulation 117: 3171-3180.
- Webber LS, Srinivasan SR, Wattigney WA, Berenson GS (1991) Tracking of serum lipids and lipoproteins from childhood to adulthood. The Bogalusa Heart Study. Am J Epidemiol 133: 884-899.
- Williams CL, Hayman LL, Daniels SR, Robinson TN, Steinberger J, et al. (2002) Cardiovascular health in childhood: a statement for health professionals from the committee on atherosclerosis, hypertension, and obesity in the young (AHOY) of the council on cardiovascular disease in the young, American Heart Association. Circulation 106: 143-160.
- Ogden CL, Yanovski SZ, Carroll MD, Flegal KM (2007) The epidemiology of obesity. Gastroenterology 132: 2087-2102.
- Reilly JJ and Kelly J (2011) Long-term impact of overweight and obesity in childhood and adolescence on morbidity and premature mortality in adulthood: systematic review. Int J Obes 35: 891-898.
- Raitakari OT, Juonala M, Kahonen M, Taittonen L, Laitinen T, et al. (2003) Cardiovascular risk factors in childhood and carotid artery intima-media thickness in adulthood. The cardiovascular risk in young finns study. JAMA 290: 2277–2283.
- Dietz WH (1998) Health consequences of obesity in youth: Childhood predictors of adult disease. Pediatr 101: 518-525.
- Ho M, Garnett SP, Baur L, Burrows T, Stewart L, et al. (2012) Effectiveness of lifestyle interventions in child obesity: Systemic review with meta-analysis. Pediatr 130: e1647-e1671.
- Mauro M, Taylor V, Wharton S, Sharma AM (2008) Barriers to obesity treatment. Eur J Intern Med 19: 173-180.
- Kirk S, Zeller M, Claytor R, Santangelo M, Khoury PR, et al. (2005) The relationship of health outcomes to improvements in BMI in children and adolescents. Obes Res 13: 876-882.

