Sietze A Koopal1, Robby E Kibbelaar2, Jan A Zijlstra1, Jean Pierre EN Pierie1
1Department of Gastro-Intestinal Surgery, Leeuwarden Medical Center
2Laboratory of Public
Health Friesland, Department of Pathology. Leeuwarden, The Netherlands
- *Corresponding Author:
- Sietze A Koopal
Department of Abdominal Surgery
Medical Center Leeuwarden
P.O.Box 888
8901 BR Leeuwarden
The Netherlands
Phone: +31-58.28.66.666 (beeper 480)
Fax: +31- 58-28.66.946
E-mail: s.a.koopal@znb.nl
Received September 9th, 2005- Accepted September 26th, 2005
Keywords
Jaundice; Pancreas; Pancreaticoduodenectomy; Tuberculosis
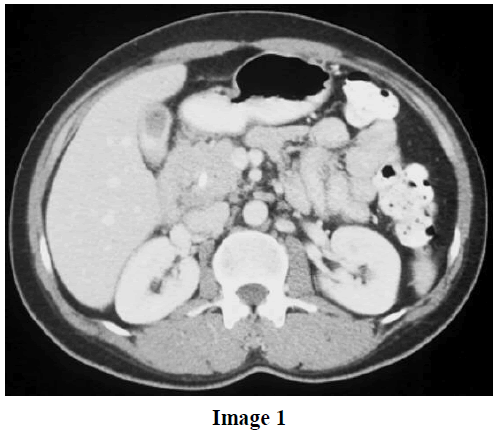
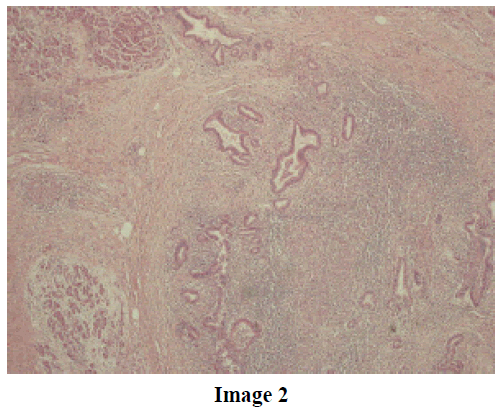
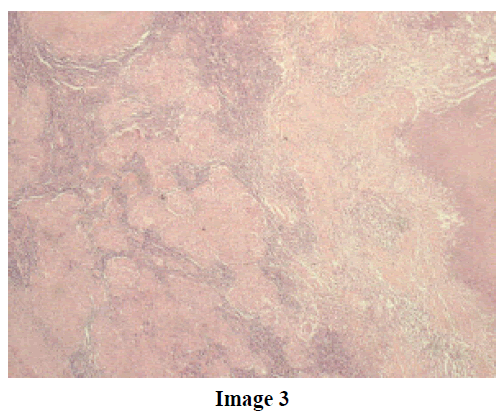
A 38-year-old male from Iraq without any history of previous infections presented at our institute with recently developed jaundice caused by a pancreatic head mass. A CT scan of the abdomen showed the mass in the pancreatic head without lymph node involvement or infiltration of the vascular structures (Image 1). ERCP revealed a double duct sign. Endoscopic stent placement adequately decompressed the common bile duct. At laparotomy, frozen section analysis of the lymph node samples (located at the hepatoduodenal ligament, diameter 1 cm, and the radix mesenterii, diameter 0.5 cm) showed no malignancy. A 4-cm mass was palpable in the pancreatic head and a pylorus-preserving pancreatic-duodenectomy was performed. Pathological examination of the specimen showed chronic pancreatitis caused by an extensive necrotizing granulomatous inflammation (Image 2); staining for acid fast bacilli were positive. The peripancreatic lymph nodes also showed typical caseating granulomas (Image 3). The patient was successfully treated with anti-tubercular therapy and is doing well. Isolated pancreatic tuberculosis is extremely rare [1] and is usually not suspected prior to exploratory laparotomy or even definitive histological examinations.
As recently described in literature, it is a relevant problem as abdominal tuberculosis is becoming more common as world-wide emigration increases and, therefore, it should be considered in the diagnosis for a pancreatic mass [2].
References
- D'Cruz S, Sachdev A, Kaur L, Handa U, Bhalla A, Lehl SS. Fine needle aspiration diagnosis of isolated pancreatic tuberculosis. A case report and review of literature. JOP. J Pancreas (Online) 2003; 4:158-62. [PMID 12853684]
- Woodfield JC, Windsor JA, Godfrey CC, Orr DA, Officer NM. Diagnosis and management of isolated pancreatic tuberculosis: recent experience and literature review. ANZ J Surg 2004; 74:368-71. [PMID 15144259]

