Mauro Toniolo1*, Elisabetta Daleffe1, Luca Rebellato1, Domenico Facchin1 and Alessandro Proclemer1,2
1Division of Cardiology, University Hospital of “S. Maria Della Misericordia”, Udine, Italy
2I.R.C.A.B. Foundation, Udine, Italy
*Corresponding Author:
Mauro Toniolo Division of Cardiology
University Hospital of “S. Maria Della Misericordia”
P. le S. Maria Della Misericordia 15
33100 Udine, Italy
Tel: + 39 0432 552442
Fax: + 39 0432 554448
E-mail: mautoniolo@libero.it
Received date: February 06, 2017; Accepted date: February 12, 2017; Published date: February 14, 2017
Citation: Toniolo M, Daleffe E, Rebellato L, et al. Cardiac Arrest Induced by Anti-Bradycardia and Anti-Tachycardia Therapies of an Implantable Cardioverter Defibrillator. Interv Cardiol J 2017, 3:1. doi:10.21767/2471-8157.100047
Keywords
Cardiac arrest; Anti-tachycardia therapy; Antibradycardia therapy; Implantable cardioverter-defibrillators.
Introduction
Implantable cardioverter-defibrillators (ICD) can terminate ventricular tachy-arrhythmias (VTs) with shocks or antitachycardia pacing (ATP). Lots of studies demonstrated that ATP terminates most of VTs but with a 1% to 7% risk of acceleration or precipitation of these arrhythmias [1,2]. Also, anti-bradycardia therapy can have an intrinsic arrythmogenic risk [3].
Description
A 63-year-old man with a dilatative hypokinetic cardiomyopathy (ejection fraction 30%) due to a severe mitral regurgitation, permanent atrial fibrillation, NYHA class III, had a primary-prevention of sudden cardiac death indication to receive an ICD.
A single-coil transvenous defibrillation lead was positioned at the right ventricular apex. The device (Biotronik Lumax 740 VR-T) was programmed to minimize unnecessary right ventricular pacing (lower rate 50 beats per minute -bpm- with a hysteresis of 10 bpm). Regarding anti-tachycardia therapies, the device was programmed to two detection zones: one from 188 to 214 bpm with ATP (3 Burst) followed by shock therapy if pacing did not terminate the detected tachyarrhythmia and another one at 214 bpm or higher with direct shock therapy.
One week after ICD implant, the patient acceded to our emergency department because of syncope. Interrogation of the ICD revealed an unexpected phenomenon: after a pause in heart rhythm due to atrial fibrillation, we could see a single beat induced by anti-bradycardia therapy of ICD start to a monomorphic ventricular tachycardia (VT) with a medium heart rate of 200 bpm (Figure 1a). The ATP degenerated VT in a ventricular fibrillation (VF) (Figure 1b).
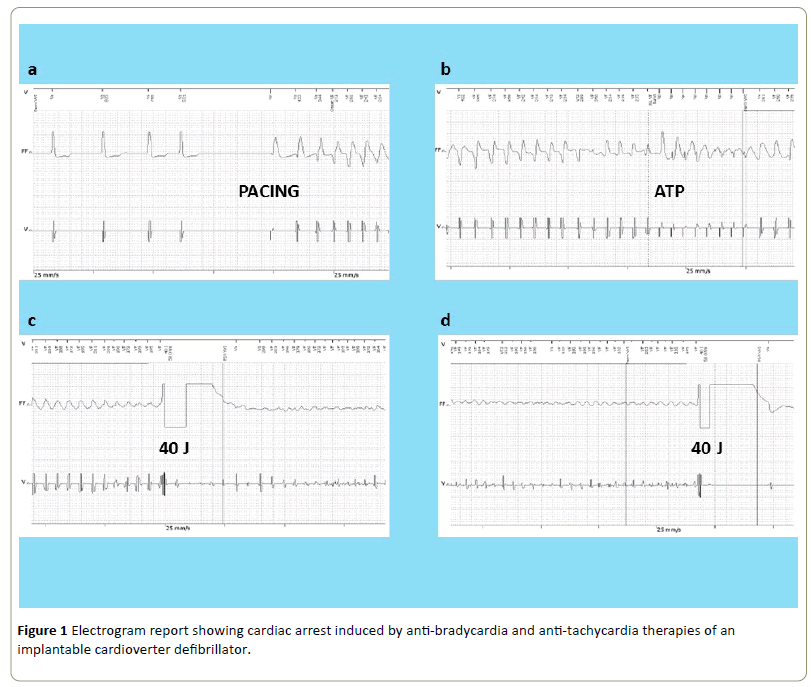
Figure 1: Electrogram report showing cardiac arrest induced by anti-bradycardia and anti-tachycardia therapies of an implantable cardioverter defibrillator.
The first 40 Joule shock did not interrupt VF but converted it in a very low amplitude VF (Figure 1c) that was not interrupted by a second 40 Joule defibrillations inverting shock polarity. Fortunately, VF was interrupted by a third 40 Joule shock (Figure 1d).
Following days, we decided to replace the single-coil defibrillation lead with a dual-coil lead to improve defibrillation threshold and we also modified anti-bradycardia programming reducing lower rate to 30 bpm and antitachycardia pacing with inactivation of ATP.
We decided not to change the position of defibrillation lead within the right ventricle and we decided not to perform a defibrillation test before hospital discharge for the poor hemodynamic stability of the patient.
After 1 year follow-up, the patient did not have further arrhythmic events.
The ICD is remarkably effective in preventing sudden cardiac death in high-risk patients [4], but it also has the capacity to provoke or worsen cardiac arrhythmias [1-3]. Tachyarrhythmias may result from the delivery of antitachycardia or anti-bradycardia therapies by tiered-therapy defibrillators.
References
- Klein RC, Raitt MH, Wilkoff BL, Beckman KJ, Caromilas J, et al. (2003) Analysis of implantable cardioverter defibrillator therapy in the antiarrhythmics versus implantable defibrillators (AVID) trial. J CardiovascElectrophysiol 14: 940-948.
- Wathen MS, DeGroot PJ, Sweeney MO, Stark AJ, Otterness MF, et al. (2004) Prospective randomized trial of empirical anti-tachycardia pacing versus shocks for spontaneous rapid ventricular tachycardia in patients with implantable cardioverter-defibrillators. Circulation 110: 2591-2596.
- Himmrich E, Przibille O, Zellerhoff C, Liebrich A, Rosocha S, et al. (2003) Pro-arrhythmic effect of pacemaker stimulation in patients with implantable cardioverter-defibrillators. Circulation 108: 192-197.
- Bardy GH, Lee KL, Mark DB, Poole JE, Packer DL, et al. (2005) Amiodarone or an implantable cardioverter-defibrillator for congestive heart failure (SCD-HeFT). N Engl J Med 352: 225-237.

