Rosen KG*
Department of Engineering, University of Borås, SE-50190 Borås, Sweden
*Corresponding Author:
Rosen KG
Department of Engineering, University of Boras, SE-50190 Borås, Sweden
Tel: 0733-72 22 02
E-mail: kg.rosen@neoventor.se
Received date: March 08, 2016 Accepted date: April 20, 2016 Published date: April 22, 2016
Citation: Rosen KG. Case Report Maternal Pyrexia + Biphasics. Gynecol Obstet Case Rep. 2016, 2:1.
Keywords
Preeclampsia, Labor, Cerebral Palsy, Fetal distress, STAN
Introduction
25 year old Para 0, preeclampsia developing during the last week of pregnancy.
Progress of labor
12:40 Meconium stained fluid noted at artificial rupture of membranes. 18:40 Epidural sited and pitocin infusion started due to slow progress.
20:04 Two Biphasic ST Events were noted and Paracetamol was given due to maternal temperature 37.9°C (100.2°F).
20:59-21:12 Four Biphasic ST Events were recorded. 21:24 Maternal temperature rise of 38.2°C (100.8°F). 21:35 Antibiotics were administered.
23:59 Vacuum extraction delivery for fetal distress.
Neonatal outcome
Baby girl. BW 3585 g. Apgar scores 0-1-3.
Cord sample pH 7.0 pCO2 not available to calculate base deficit in the extracellular fluid (BDecf) but base excess in the blood compartment (BE) was -16.6 mmol/l.
Immediate resuscitation with assisted ventilation and buffering. Early seizures and feeding problems indicating a more substantial brain injury, Magnetic resonance imaging (MRI) abnormalities and assessed as Cerebral Palsy likely due to hypoxic ischemic encephalopathy (HIE).
Assessment of Recording
High quality STAN recording starting at 12:33 and finishing at 23:39, 20 minutes before delivery (Figures 1-5).
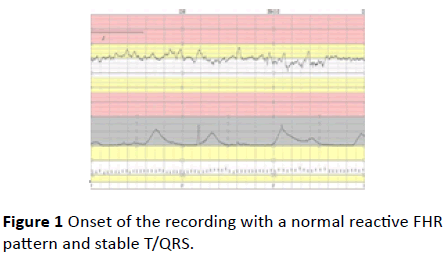
Figure 1 Onset of the recording with a normal reactive FHR pattern and stable T/QRS
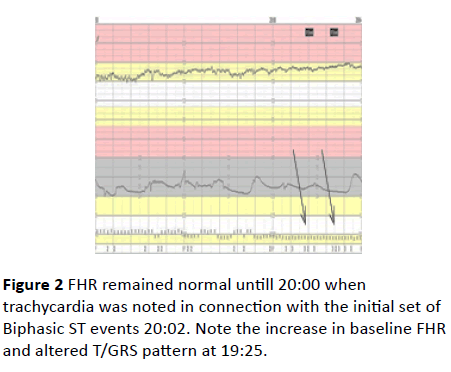
Figure 2 FHR remained normal untill 20:00 when trachycardia was noted in connection with the initial set of Biphasic ST events 20:02. Note the increase in baseline FHR and altered T/GRS pattern at 19:25.
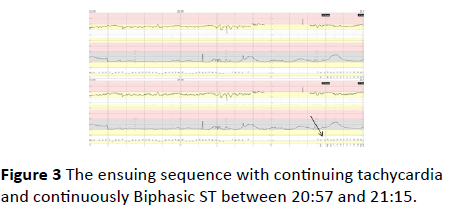
Figure 3 The ensuing sequence with continuing tachycardia and continuously Biphasic ST between 20:57 and 21:15.
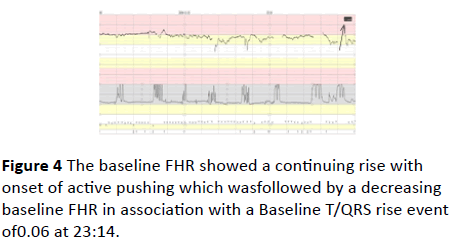
Figure 4 The baseline FHR showed a continuing rise with onset of active pushing which wasfollowed by a decreasing baseline FHR in association with a Baseline T/QRS rise event of 0.06 at 23:14.
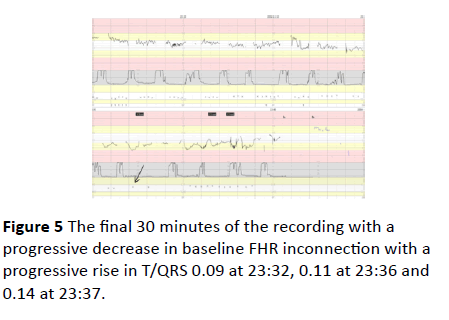
Figure 5 The final 30 minutes of the recording with a progressive decrease in baseline FHR inconnection with a progressive rise in T/QRS 0.09 at 23:32, 0.11 at 23:36 and 0.14 at 23:37.
Comments
A case captured during the development of intrapartum hypoxia in association with a fetal response to an inflammatory process causing metabolic acidosis, hypoxic encephalopathy and long-term sequel.
The STAN methodology is based on improving our ability to identify and interpret specific fetal reactions and respond appropriately. In case of maternal pyrexia, Biphasic ST would indicate a myocardium functionally affected from endotoxins such as lipid polysaccharide (LPS).
The continuously Biphasic ST sequence lasting >5 minutes in association with the rise in baseline FHR occurring 3 h before delivery should have been sufficient information to cause an intervention. Antibiotics would not affect endotoxins, nor would a scalp-pH provide additional information. Thus the appropriate intervention in case of maternal pyrexia, tachycardia and >2 Biphasic ST events would have been to deliver operatively.
To undertake an fetal scalp blood sample (FBS) at this point in time would not provide additional information as myocardial function in the term fetus would not be affected to the extent of a decrease in cardiac output lowered blood pressure and deteriorating gas exchange. Such a pattern may be found 2-4 h after the administration of endotoxin (LPS) (data from fetal sheep1). It seems most likely that the decrease in baseline FHR occurring in connection with the rise in T/QRS would serve to indicate more severely affected cardiacfunctioning caused by the time factor as well as the onset of contractions.
Current understanding of mechanisms behind brain tissue damage brings the combination of an inflammatory reaction and hypoxia to the fore. The combination of the two may also serve to explain the very early onset of neonatal seizures and adverse outcome.
Message
Biphasic ST + maternal temperature rise should always be considered as an indication of a fetus exposed to a bacterial infection.
References
- Blad S, Welin AK, Kjellmer I, Rosén KG, Mallard C (2008) ECG and Heart Rate Variability Changes in Preterm and Near-Term Fetal Lamb Following LPS Exposure. Reprod Sci.15:572-83.

