Keywords
Acidosis; Digestive System; Pancreatic Juice; Pancreatitis
INTRODUCTION
Over the last sixty years, there has been an increase in digestive disorders, especially in the U.S. and developed countries. This increase cannot be explained solely by genetic factors, so the environmental causes come to the light of scientists and doctors. The Burden of Digestive Diseases in the United States might illustrate the medical statistic [1-4].
Researchers from the Mayo Clinic College of Medicine USA, in the study of more than 21,000 Americans, found that the prevalence of an average of one or more upper GI symptoms during the last 3 months was 44.9% [5].
There are 60 to 70 million people affected by digestive diseases in the U.S. [1]. This is an official medical statistic of the number of Americans seeking medical care at doctor offices and hospitals, but this number is only the tip of the iceberg. This statistic does not include people without medical insurance, people who use alternative methods of treatment, or individuals who simply accept their symptoms as “normal” and do not seek medical help.
The food revolution has had a significant impact on preparing, conserving, preserving, and dispensing modern food for the last 60 years. This decreases the amount of essential enzymes, vitamins, minerals, and bicarbonate in the foods. A deficiency of minerals such as potassium, magnesium, calcium, zinc, cobalt, and bicarbonates in modern food products shifts the body’s internal environment from slightly alkaline to acidic causing chronic metabolic acidosis.
The modern processed foods have been available for only several generations; therefore, genetic adaptation to these foods in such a short period is highly unlikely. Sugars, refined white flour and white rice, soft drinks and “trans” fats are man-made artificial acid-formed products that have an extraordinary impact on the digestive system and on the content of the pancreatic juice and bile.
PATHOPHYSIOLOGY OF METABOLIC ACIDOSIS
Metabolic acidosis is a condition that arises when the body generates too much acid or when the organs, which are liable for the elimination of acidic radicals, cannot remove or neutralize enough acids from the organism.
What causes the body to be acidic? The main factors are:
• The production of too many acidic substances, such as carbonic acid, lactic acid, ketenes, by human cells
• The production of too many acidic substances by microorganisms that reside inside the body, for example, constant fermentation in case of dysbiosis (Candida-yeast overgrowth or small intestine bacterial overgrowth – SIBO)
• The consumption of processed, acid-forming foods such as sugars, sodas, white flour, white rice, red meat
• Acute or chronic intoxication from acid producing substances including alcohol, chemicals, some acidosis-forming medications
• Low or improper function of the lungs, kidneys, liver and GI organs
• Dehydration and/or poor microcirculation
• Low capacity of buffer systems in the blood, mainly a low capacity of bicarbonate buffer
Body acids are produced as the end products of cellular metabolism. The average person generates from 50 to 100 mEq of acid per day from the metabolism of protein, carbohydrates, and fats, and from the loss of alkaline substances in the stools [6]. To maintain a normal pH, an equivalent amount of acid must be neutralized or excreted. The lungs, kidneys, blood, bones, skin, liver, gallbladder, stomach, and pancreas are involved in the regulation of the body’s acid-alkaline balance [7]. Many body functions are designed to regulate the acid-base balance, including respiration, excretion, circulation, digestion, and cellular metabolism.
The human body has a complicated, multifunctional mechanism to neutralize these acids or remove them from the body via (CO2) carbon dioxide, a gas that is eliminated by the lungs or, by keeping bicarbonate ions (HCO3-) in the blood by the kidneys. The kidneys and lungs are the principal organs that help manage the blood concentrations of CO2 and the bicarbonate ion (HCO3-), helping to control the pH of the blood.
The blood is normally slightly alkaline with a pH range of 7.35 to 7.45. The constancy of the blood pH is important for the body's capability to maintain a relatively unchanging internal milieu. The pH of the blood is constant, and the organism struggles to keep it constant to protect the brain, lungs, and the heart, which completely stop functioning if the pH in the blood falls even slightly.
In the bloodstream, there are substances identified as buffers, which act chemically to resist changes in the pH. The major buffer system in the blood is the CO2-bicarbonate buffer system (the “bicarbonate buffer”). It is the most powerful blood buffer for metabolic acids. It works in the following manner:
Lung  CO2 + H2O <==> H2CO3 <==> H + + HCO3- kidney
CO2 + H2O <==> H2CO3 <==> H + + HCO3- kidney
The formation of bicarbonate ions (HCO3-) occurs by the following reactions:
Hydration of CO2: CO2 + H2O => H2CO3
Dissociation of H2CO3: H2CO3 => H + + HCO3-
The H2CO3 / HCO3- - combination acts as the primary buffer in the blood.
The bicarbonate buffering system is essential in many different processes including:
- It is one of the key buffering systems used to maintain the pH of human blood.
- It protects the lumen of the stomach during the formation of hydrochloric acid.
- It neutralizes the pH of the chyme leaving the stomach and entering the duodenum.
- This is the main factor of alkalinity of pancreatic juice and bile.
NEGATIVE ACTION OF THE METABOLIC ACIDOSIS ON PANCREATIC JUICE, BILE, AND ENTIRE DIGESTIVE SYSTEM
The pancreas and liver are alkaline glands because they produce pancreatic juice and bile, which are normally alkaline solutions. The pancreatic juice has a pH of 8.0- 8.3, and the pH of liver bile is 7.8 [8]. The pancreas, liver, and gallbladder are the organs that are engaged in the human being’s acid – base balance. When acidity depletes the alkaline reserve in the body, this process destroys the function of the liver, gallbladder, and pancreas. The liver and the pancreas take the minerals and bicarbonates from the blood to create alkaline pancreatic juice and bile.
During metabolic acidosis, the organism chooses to save the vital organs, such as the brain, lung, and, heart at the expenses of peripheral “less essential” organs and tissues. The liver, gallbladder, and pancreas are the organs that suffer the most from over acidity in the body. In this situation, their capability to take minerals and bicarbonates from the blood becomes low, and the pH of their secretions drops (acidic pancreas and bile). The biochemistry, composition, and function of these organs change in a harmful way.
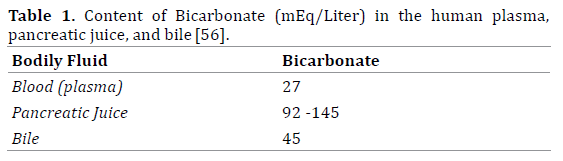
The importance of Bicarbonate
The bicarbonate content is a prime factor of alkalinity in bile and pancreatic juice. It is obvious that in bile and pancreatic juice, there is more bicarbonate than in the blood plasma. Scientists found that the pancreas and liver take bicarbonate ions primary from the blood. Intravenously injected bicarbonate labeled with the 11C radioisotope appears promptly in the pancreatic juice. Scratcherd, T and Case, RM and other researchers suggested that pancreatic secretion is directly related to the concentration of bicarbonate, and experiments suggested “most if not all the bicarbonate of pancreatic juice must come from plasma [9-11].” Bicarbonate secretion in the pancreatic duct is decreased by chronic systemic metabolic acidosis. The concentration of bicarbonate in pancreatic juice depends on the concentration of bicarbonate ions in the plasma [9].
When the acidic chyme travels from the stomach into the duodenum, the secretion of bicarbonate increases and then decreases, possibly because of the lowering of the amount of bicarbonate capacity inside the pancreas. Infusing bicarbonate into the blood throughout the digestive process promotes the increase of bicarbonate in the pancreatic juice. There is considerable evidence that there is a decrease in the amount of bicarbonate in the pancreatic juice and bile in patients with pancreatic diseases [12-13].
Lieb II J. and Peter V Draganov P. (2008) considered that decreasing the amount of bicarbonate in the pancreatic juice has practical clinical importance [14]. Duodenal acidity mostly depends on a lower amount of bicarbonate in the pancreatic juice and bile. In chronic pancreatitis patients who often suffer from pancreatic exocrine insufficiency, the duodenal pH is persistently low [13, 15]. A defective capacity to secrete bicarbonate in patients with pancreatic exocrine insufficiency is unfavourable for the digestive enzymes’ activity [16]. A low pH in the duodenum is one of the essential factors known to influence the activity of all the pancreatic enzymes [17].
Mc Clave, SA believed that while healthy people have a high bicarbonate concentration in the duodenum, patients with chronic pancreatitis have a low bicarbonate concentration. In this situation, the acidic milieu in duodenum inactivates the pancreatic enzymes. Pancreatic lipase stops working if the duodenal pH < 4.5 [18].
Talamini G. (2005) focused on the connection between duodenal acidity and lower exocrine pancreatic function [15]. He wrote that chronic pancreatitis patients often present with pancreatic exocrine insufficiency combined with a steadily low duodenal pH in the postprandial period. The duodenal acidity might increase the risk of pancreatic cancer in the course of chronic pancreatitis (Table 1) [15].
Metabolic acidosis with a low concentration of bicarbonate in the plasma negatively influences the pancreatic functions
The relationship between the rate of low pancreatic HCO3- secretion and high plasma H+-ion concentration was studied in numerous experiments. A proportional, opposed correlation was found between HCO3- secretion and an acidic shift in the plasma pH [10]. Different relationships were found between pancreatic HCO3- secretion and plasma HCO3- concentration in metabolic acidosis. Pancreatic HCO3- secretion falls to 41 ± 4% of controls during acidosis. Plasma H+-ion concentration seems to determine the rate of pancreatic HCO3- secretion [19].
J. Nimmo et al. (1970) found a lower amount of bicarbonate in the pancreatic juice in patients with pancreatic disorders compared with healthy volunteers [20]. Studies show a direct association between bicarbonate concentration and pancreatic juice flow. There is a positive correlation between the elimination of enzymes and bicarbonate concentrations [21]. The importance of plasma bicarbonate was demonstrated by in vivo experiments, in which pancreatic secretion was studied under the conditions of metabolic acidosis. Canine pancreatic secretion was halved when the plasma bicarbonate was lowered to 16 mEq/L [9].
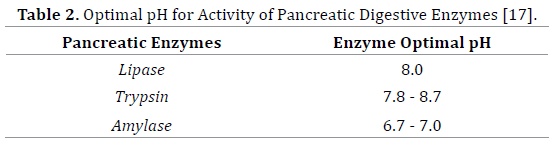
Extremely low pH values result in the complete loss of activity for most pancreatic digestive enzymes. The pH is a factor in enzyme stability. As with activity, there is a range of pH for the optimal stability for each enzyme. Normally, digestive enzymes have a pH optimal for maximum activity. Changes in the pH in the small intestine can alter the activity of the pancreatic enzymes.
A decrease in the activity of the pancreatic enzymes due to metabolic acidosis is critical for proper understanding of many symptoms of indigestion and functional gastrointestinal disorders. Improperly digested foods accumulate in the small intestine and irritate the gut’s walls. Bacteria and yeast ferment undigested foods by producing large quantities of gas (hydrogen, methane) and other toxic substances. The organism tends to eliminate this irritated and poisonous matter. There are only two directions for moving this undigested mass: up to the stomach and down to the large intestine. Moving the mass upwards can cause fullness, nausea, vomiting, heartburn, gas, bloating, cramps, and upper abdominal pain. If the undigested mass moves down, it can cause flatulence, diarrhoea, constipation, inferior abdominal pain. Many of these symptoms are remarkably similar to the symptoms of functional dyspepsia and/or irritable bowel syndrome (IBS) (Table 2). Almost 35% of the world population suffers from functional gastrointestinal disorders, involving approximately 40% of gastroenterologist and 12% of primary care practices [23].
In 1987, H. Worning wrote in Digestion that the prevalence of pancreatic diseases as the cause for dyspepsia varies in clinical materials between 0 and 25-30%. In his view, pancreatic function and pancreatic diseases are connected to different gastrointestinal diseases (duodenal ulcer, malabsorption syndromes, inflammatory bowel diseases, subtotal and total gastrectomy and to some extent in patients with hepatobiliary diseases) [24].
Okada R et al. (2009) considered that mild functional pancreatic disorders might trigger some cases of unexplainable chronic dyspepsia [25]. Eva Lindström et al. (1990) suggested that altogether, 66% of patients with abdominal pain had morphological and/or functional confirmation of pancreatic involvement [26]. Some researchers agree that the distinction between functional dyspepsia and the early stages of chronic pancreatitis is difficult [27]. The early stages of chronic pancreatitis and decreasing exocrine pancreatic function are commonly misdiagnosed.
According to the Second Giessen International Workshop on Interactions of Exocrine and Endocrine Pancreatic Diseases in 2008 “early chronic pancreatitis remains a diagnostic challenge as there is no gold standard for the diagnosis and pancreatic biopsy is risky and impractical. Reported data on the incidence and prevalence of chronic pancreatitis are unreliable and extremely variable. Chronic pancreatitis is clearly under – diagnosed” [28]. The diagnosis of the beginning of the pancreatic disorders might be missed in clinical practice because the symptoms of severe exocrine pancreatic deficiency (malabsorption syndrome and maldigestion) are not specific in the beginning of chronic pancreatitis. Early chronic pancreatitis and low exocrine pancreatic function due to metabolic acidosis are rarely suspected when the pain is mild or not present and when the symptoms are nonspecific (“dyspepsia”) in the absence of steatorrhea.
About 80,000 cases of pancreatitis annually occur in the USA. This is only the tip of the iceberg of digestive (pancreatic) diseases. Acute and chronic pancreatitis are diseases on the rise.
The diagnosis of chronic pancreatitis can be challenging since laboratory studies and imaging procedures may be normal, especially in the beginning of this process. Most attacks of pancreatitis are mild and go undiagnosed.
The authors completely agree with John Alfred Lott, who wrote in his book Clinical Pathology of Pancreatic Disorders that generally, pancreatic insufficiency is graded as mild when only bicarbonate output is decreased, moderate when enzyme output is also decreased and severe when fecal fat output is increased (steatorrhea) [29].”
Trypsinogen activity and pH
A well-known authority in the pancreatic diseases in the US, Professor David C Whitcomb, wrote in 2004 about the activation of digestive enzymes inside the pancreas. “Observations suggest that the key to controlling digestive enzyme activation and pancreatic injury is to control trypsin. The high pH in the duct inhibits activated trypsin by interfering with the transition between trypsinogen and trypsin” [30].
The suggestion that acidifying the pancreatic juice triggers the premature activation of trypsinogen to trypsin in the pancreatic ducts is not new. In 1953, Green NM and Work E., determined that the slow rate of reaction between a trypsin inhibitor and trypsin is pH dependent because both proteins have alkaline isoelectric points. The more alkaline the pancreatic juice, the higher the possibility of keeping trypsin inactive within the pancreas. Even neutral pH 7.0 can promote this activation [31].
Niederau C and Grendellin JH (1988) proposed that acidifying the pancreatic juice might play a role in the progression of acute pancreatitis [32]. Bhoomagoud M et al. (2009) believed that metabolic acidosis can be a risk factor for developing pancreatitis. They proved experimentally in vivo and in vitro that decreasing the pH (acidifying) raises the sensitivity of the acinar cells to zymogen activation [33].
Both clinical and experimental observations suggest that acidosis may increase the risk of developing acute pancreatitis. Peter Hegyi at al. (2011) emphasize that the failure of pancreatic ductal bicarbonate secretion (i.e., the decrease of luminal pH) can increase the risk or lead to pancreatitis [34].
Flushing inactive pancreatic enzymes prevents their premature activation
An additional protective mechanism for preventing the premature activation of trypsinogen to trypsin within the pancreatic duct is quickly sweeping zymogens out of the pancreas. Flushing and draining pancreatic juice that contains inactive enzymes, zymogens (trypsinogen), to the duodenum as soon as possible to prevent the premature activation of digestive enzymes inside the pancreas is extremely important for protecting the pancreas from the development of acute and chronic pancreatitis.
The pancreatic duct cells are responsible for fluid and bicarbonate secretion. A high concentration of ions, including bicarbonate, promotes water entering the lumen by osmosis. Water flushes the contents of the pancreatic duct lumen, including the zymogens, out of the pancreas into the duodenum. Low bicarbonate production can reduce the amount of water inside the pancreatic ducts. This increases the viscosity of pancreatic juice and slows its elimination [30].
According to Matsuno S et al. (1991), bicarbonate plays a key role in the viscosity of pancreatic juice in pancreatitis patients. They found that bicarbonate secretion and bicarbonate output are decreased, and the viscosity of pancreatic juice was substantially increased in pancreatitis. They believed that concentrated pancreatic juice could cause the progression of chronic pancreatitis [35].
Acidification of bile and bile refluxes
Normally, the alkalinity of bile depends on the amount of bicarbonate. A low amount of bicarbonate and a lower pH (acidification of bile) cause many negative biochemical alterations in the bile and biomechanical changes of bile elimination. If the bile becomes acidic, it becomes “aggressive”. Evidence suggests that acidifying the bile leads to the precipitation of the extremely corroded bile acids. For instance, 50% of the bile acids were precipitated at a pH less than 5, compared with only 26% at a pH greater than 6 [41]. In patients with chronic pancreatitis, there are often abnormalities of the motor interaction of the biliary system, duodenum, and stomach, which can result in severe duodenogastric reflux [16].
Precipitated bile acids and other aggressive components from the acidic bile irritate the walls of the bile ducts, gallbladder, pancreatic duct, Sphincter of Oddi, Ampulla of Vater and duodenum. This induces spasms, irritation, inflammation, ulcers, etc. Irritations of the mucosa by precipitated bile acids initiate erosion, ulcers, and spasmodic contractions, which affect the proper flow of “aggressive” bile/pancreatic juice mixture.
“Aggressive” bile often creates reflux, which is the backflow of bile into the pancreatic duct or when bile runs upward from the duodenum into the stomach and oesophagus. Bile reflux has an impact on the duodenum and stomach and leads to further inflammation, ulcers, and cancer. Bile reflux often is associated with gastric acid reflux, and together they are terrible and inflame the lining of the oesophagus and can raise the risk of oesophageal cancer [37-39]. Biliary pancreatic reflux occurs when the bile goes back to the pancreatic duct and might initiate acute pancreatitis and/or aggravate chronic pancreatitis.
Decreasing the bile pH is a predisposing factor for producing gallbladder stones. According to Rege, RV and Moore, EW (1986), the acidification of bile is a key factor in developing gallbladder stones, which can block the bile and pancreatic ducts leading to damage to the liver, gallbladder, and pancreas [40].
The antimicrobial activity of pancreatic juice is pH dependent
A variety of factors controls the intestinal microbial homeostasis. Pancreatic juice plays an essential role in keeping the number of microorganisms in the small intestine low. Experiments on people with pancreatic fistulas or during endoscopic cannulation of the main pancreatic duct showed that the pancreatic juice in healthy persons was virtually sterile [42, 43]. Conducted tests show that pancreatic juice destroys almost the entire spectrum of microorganisms. Ramare F et al. (1993) uncovered a similarity between antibacterial factors in the pancreatic juice with trypsin [44]. Acidification of the pancreatic juice and a decrease in the pancreatic secretions make the pancreas more susceptible to infection.
Rubinstein, E et al. (1985) found that the antibacterial activity of pancreatic juice was pH dependent [45]. The antibacterial activity of pancreatic juice is extremely sensitive to pH, having an optimal activity at pH 8.5 (alkaline condition) and with a complete cessation of action at pH 7.0 (neutral reaction of solution) [46]. Metabolic acidosis, acidification of the pancreatic juice and the subsequent decreasing of the antibacterial activity of the pancreatic juice can be a causative factor for small intestine bacterial overgrowth (SIBO). This can be a reason for various symptoms of indigestion and abdominal pain.
Calcification
Chronic metabolic acidosis forces humans to obtain calcium from the bones into the blood to neutralize over acidity. The concentration of calcium in the blood and bodily fluids increases [47]. Calcium deposits in the blood vessels and internal organs (calcinosis) [7, 48] This might explain the common concurrent existence of osteoporosis, arteriosclerosis, and calcification of the inner organs. Calcification of the pancreas is a significant symptom of chronic pancreatitis [47, 49, 50].
The precipitation of calcium salts within the pancreatic duct leads to stones, which irritate or block the pancreatic duct causing pancreatitis. The precipitation of calcium salts inside the gallbladder results in stone manufacturing and possible obstruction of the bile ducts or sphincter of Oddi. This raises the pressure inside the pancreatic duct, activates digestive enzymes inside the pancreas, causing self-digestion and pancreatitis. In systems containing Ca2+ ions and unconjugated bile acids, the pH is important because it is the key determinant of the formation of the insoluble calcium salts, which are a component of bile stones [51].
Finally, normal exocrine pancreatic function is crucial for proper digestion. Metabolic acidosis leads to decreased bicarbonate in the blood and in the pancreatic juice. Bicarbonate is a main factor for the alkalinity of the pancreatic juice. In cases of metabolic acidosis, the pH of the pancreatic juice decreases (acidification). Acidic changes in pancreatic secretion can lead to the deterioration of the exocrine pancreatic functions, such as a low activity of pancreatic digestive enzymes.
Acidification of the pancreatic juice can activate trypsin inside the pancreatic duct, suppresses the flushing of the inactive pancreatic enzymes to prevent their premature activation, and decreases the antimicrobial activity of the pancreatic juice. These negative influences of metabolic acidosis, besides the pancreas, cause the acidification of bile with the consequent precipitation of the “aggressive” insoluble bile acids and the formation gallbladder stones. Many factors support that chronic metabolic acidosis can be a reason for numerous digestive disorders.
DISCUSSION: CLINICAL IMPLICATION
The authors’ presume that chronic metabolic acidosis destroys pancreas and entire digestion. Questions arise from this. Does chronic metabolic acidosis have clinical value in everyday practice? Is the chronic metabolic acidosis common condition in the modern human? The authors strongly believe that the subclinical, low grade, chronic metabolic acidosis is a rampant condition and can be considered as a “disease of civilization”.
Scientists have found that low grade chronic metabolic acidosis is a common problem in modern societies, and acidemia is a hidden problem that causes the development of many chronic degenerative diseases and accelerates the aging process [52-57]. Chronic metabolic acidosis affects most of the world’s population because of urbanization and a western lifestyle [58].
Researchers from the Department of Medicine and General Clinical Research Center, University of California, San Francisco, Frassetto L et al. (1997) demonstrated “low grade chronic metabolic acidosis exists generally in humans eating ordinary diets. This diet yields normal net rates of endogenous acid production (EAP) and that the degree of acidosis increases with age [52]”.
Chronic metabolic acidosis is dangerous for humanity. It involves most of the global population and might cause epidemic proportions of metabolic syndrome, diabetes, osteoporosis, kidney and gallbladder stones, cardiovascular diseases, digestive disorders, cancer, intestinal dysbiosis, and many other metabolic and degenerative diseases, which have increased over the past 50 years [7, 58].
It is understandably difficult to think of “metabolic acidosis” when the standard lab tests for the acid-base balance are in the range traditionally considered normal [52, 55]. Ordinary tests cannot reveal the shift to acidity because humans have an enormous buffer capacity. Mild chronic metabolic acidosis can occur despite normal blood pH and bicarbonate levels [55]. In cases of metabolic acidosis, humans try to eliminate H+ ions in body fluids.
Repeated measurements of the saliva and urine pH can indirectly estimate the acid-base status. The saliva and urine pH, which are constant, lower than 6.6 can be a sign of chronic metabolic acidosis. The degree of metabolic acidosis is mild as judged by the degree of the blood acidbase imbalance, but it cannot be considered mild as judged by its negative physiological effects [52, 55].
There are many reasons for chronic metabolic acidosis. Three can have substantial implications on the health of the current world population.
1. Modern food
2. Alcohol consumption
3. Overusing of acidosis-formed medications
Modern food and metabolic acidosis
It is recognized that humans had to function at their highest physical and mental performance to survive for thousands of years. Weaker individuals or groups of people had greater chances of being eaten by predators, taken over by aggressors, succumbing to diseases and being annihilated by natural disasters. Theories surrounding the “survival of the fittest” dictate that those who are fit well for their environment will survive. The pancreatic and liver functions and the entire digestive system of our ancestors worked perfectly well for millennia fitted for the hunter/ fisher/gatherer natural diet. This diet promoted slightly an alkaline state in the human body [57, 59, 64].
The human digestive system cannot absolutely adapt to modern, chemically modified, artificial and often toxic products, which are staples of the current western diet. People cannot properly digest the foods that they are usually eating. Net acid-producing animal foods, sugars, and cereal grains have replaced alkali-rich fruits and vegetables. One of the most prevalent and preventable results is low-grade chronic metabolic acidosis, which when left untreated poses a substantial threat to human health.
The role of nutrition in human acid-base homeostasis has received growing attention in recent years. The Second International Acid-Base Symposium, Nutrition–Health– Disease was held in Munich, Germany, September 8–9, 2006. International researchers, doctors, and scientists provided deeper understanding and updates in the scientific research of the relation between diet, acidbase homeostasis, physiology, and pathophysiological consequences. They said: “Although in healthy humans, homeostatic mechanisms and the kidneys' capacity to excrete acid equivalents can prevent strong diet-induced alterations in blood pH, even moderate increases in blood hydrogen ion levels as a result of unfavourable diet composition can have long-term consequences for the occurrence and progression of a number of diseases [59].”
Many nutrition scientists estimate the net systemic acid load supplied by the diet [net endogenous acid production (NEAP)]. The NEAP for 159 replicated pre-agricultural diets was minus 88 ± 82 mEq/d; these were net baseproducing. The NEAP for the standard American diet (as recorded in the third National Health and Nutrition Examination Survey) was plus 48 mEq/d; these were net acid-producing [58].
It is clear that food is a primary cause of chronic acidity in the body. It has potential medical significance because almost all the genes and epigenetic regulatory systems humans carry today were originally selected for behaviourally modern people who appeared in Africa between 100,000 and 50,000 years ago [64].
According to Sebastian A. et al. (2002), “The historical shift from negative to positive NEAP was accounted for by the displacement of high-bicarbonate-yielding plant foods in the ancestral diet by cereal grains and energy-dense, nutrient-poor foods in the contemporary diet—neither of which is net base-producing” [58].
Alcohol consumption and chronic metabolic acidosis
Alcohol causes inflammation to the stomach, liver, pancreas, and intestines, which impairs the digestion and assimilation of food. In addition to the direct toxic effect on the liver and pancreatic cells, alcohol is a strong acid productive agent that causes chronic metabolic acidosis and the deterioration of the exocrine pancreatic function [60, 61]. Many studies show that in Western countries, alcohol is the most frequent associated factor with chronic pancreatitis (50-80% of cases) [7].
In the U.S., 10 to 20% of men and 5 to 10% of women sometime in their lives will meet the criteria for alcoholism, depending on the criteria used. These rates are equal to the rates for many countries in Western Europe [62].
Ethanol is metabolized by two pathways: the oxidative and non-oxidative pathway. Acetaldehyde and reactive oxygen species (ROS) are the main by-products of the oxidative metabolic pathway. The non-oxidative metabolism of ethanol is characterized by its esterification with the production of fatty acid ethyl esters [63]. All three byproducts of ethanol metabolism are believed to be acidforming substances [64].
Medications and metabolic acidosis
There is no extensive research about chronic metabolic acidosis and prolonged consumption of the pharmaceutical drugs [65]. Clinical studies point at acute clear-cut cases of metabolic acidosis that is confirmed by laboratory data in hospital. It could be presumed that this is the only tip of the iceberg.
Several facts indicate that various over-the-counter and prescription medications can create metabolic acidosis [66, 67].
Elevated serum pancreatic enzymes have been reported in patients treated with drugs. List of drugs associated with pancreatic hyperenzymemia is presented in article of Luca Frulloni et al. (2005) [68].
In the article “Pharmacologically-Induced Metabolic Acidosis”, Liamis G et al. (2010) wrote a review about possible mechanism and medications that cause metabolic acidosis [69]. The acid-forming actions of common medications via metabolic acidosis can negatively affect the digestive organs and digestion. This is a large area for experimental and clinical studies.
Possible correlations between the prevalence of metabolic acidosis and digestive disorders
We did not find a medical statistic that shows the prevalence of low grade, chronic metabolic acidosis in the modern population. If we consider the predominance of the acidforming, processed foods such as sugars, white flour and rice, meats, grains and dairy products, the consumption of alcohol and acidosis-producing medications, it can be presumed that the prevalence of low-grade, chronic metabolic acidosis can occur in epidemic proportions. We strongly believe that the burden of the digestive diseases in the United States and all over the world has long-term, pathophysiological consequences from the epidemic of metabolic acidosis.
The practical clinical benefit of our hypothesis is simple: to improve pancreatic function and entire digestion, beside other actions, normal acid-base homeostasis needs to be normalized by supplying humans with minerals such as sodium, potassium, magnesium, calcium, and bicarbonate. There are three natural ways for this to occur: alkalineformed plant based foods, healing mineral water, and mineral supplements.
There is no doubt about the therapeutic value of food or individual diets in the treatment of digestive disorders. Bicarbonate and minerals for the correction of metabolic acidosis and/or digestive disorders have been used in clinical practice for a long time.
For 500 hundred years, European doctors treated various digestive disorders in health mineral spas. Using sodiumpotassium- magnesium-bicarbonate healing mineral water for the treatment of liver, gallbladder, and pancreatic diseases has a long tradition, solid medical research, and positive clinical evidence. Within 3-4 weeks after drinking healing mineral water, medical doctors confirmed clinical improvements in their patients. At this time, many patients had increased bicarbonate levels in the blood and urine pH. Unfortunately, doctors explain the therapeutic effectiveness of the healing mineral water by other reasons but not the alkalizing action of this water [22, 63, 70, 71].
CONCLUSION
Digestive disorders are common in the modern world. The conventional treatment of these disorders is mostly symptomatic. The medical viewpoint on digestive disorders concentrates on the “hollow” organs such as the stomach and large intestines, and there is little attention paid to the “solid” digestive glands such as the pancreas and liver. There is no doubt that without the proper quality and quantity of the pancreatic juice and bile, the normal digestive process in the hollow chambers cannot occur. The pancreas is the core of the digestive system because it secretes the digestive enzymes.
Scientific studies and clinical evidence prove that the pancreas and liver are more vulnerable to a reduction in their functions because of metabolic acidosis. Acidifying the pancreatic juice and diminishing the activity of the digestive pancreatic enzymes can cause numerous digestive problems. The majority of the problems of the gastrointestinal tract is directly or indirectly related to the proper function of the pancreas. For that reason, a clinical diagnosis of gastrointestinal disorders de facto assumes pancreatic involvement. For now, there is not an effective and safe approach for improving the exocrine pancreatic function. Our hypothesis that chronic metabolic acidosis destroys digestion might help to identify other ways to solve the epidemic of gastrointestinal disorders and diseases.
Prospective clinical studies are required to confirm the preventive and treatment strategy of normalizing the acidbase balance in digestive and pancreatic disorders.
Conflicting Interest
Authors have no conflicts of interest.
References
- National Institutes of Health, U.S. Department of Health and Human Services. Opportunities and Challenges in Digestive Diseases Research: Recommendations of the National Commission on Digestive Diseases. Bethesda, MD: National Institutes of Health; 2009. NIH Publication 08– 6514.
- Everhart JE, ed. The Burden of Digestive Diseases in the United States. Bethesda, MD: National Institute of Diabetes and Digestive and Kidney Diseases. U.S. Dept of Health and Human Services; 2008. NIH Publication 09–6433.
- DeFrances CJ, Lucas CA, Buie VC, Golosinskiy A. 2006 National Hospital Discharge Survey. Natl Health Stat Report; 2008: 1-20. [PMID: 18841653]
- Cherry DK, Hing E, Woodwell DA, Rechsteiner EA. National Ambulatory Medical Survey: 2006 Summary. Hyattsville, MD: National Center for Health Statistics; 2008: 1-39. [PMID: 18972720]
- Camilleri M, Dubois D, Coulie B, et al. Prevalence and socioeconomic impact of upper gastrointestinal disorders in the United States: results of the US Upper Gastrointestinal Study. Clin Gastroenterol Hepatol 2005: 543-552. [PMID: 15952096]
- Koeppen BM, Stanton BA. Renal Physiology. Mosby Physiology Monograph Series. 2013.
- Melamed P, Melamed F. Healthy Pancreas, Healthy You. Part 1: Structure, Function, and Disorders of the Pancreas. Biotherapy Inc, San Francisco. https://www.smashwords.com/books/view/236176
- Guyton AC. Human physiology and mechanism of disease. 1987: 499.
- Scratcherd T, Case RM. The secretion of electrolytes by the pancreas. Am J Clinical Nutrition. 1973: 326-339 [PMID: 4266061]
- Case RM, Scratcerd T, D’A Wynne R. The origin and secretion of pancreatic juice bicarbonate. J Physiol. (London) 1970: 1-15. [PMID: 5500780]
- Ball EO, Tucker HF, Solomon AK, Vennesland B. The source of pancreatic juice bicarbonate. J. Biol Chem1941: 119.
- Johnson LR, Byrne JH. Essential Medical Physiology. Academic Press, USA, 2003.
- Matsuno S, Sasaki Y, Kobari M, et al. Initial Pathophysiological Changes in Chronic Pancreatitis Induced by Pancreatic Ductular Obstruction Model. Tohoku J Exp Med 1991: 199-210. [PMID: 1712129]
- Lieb JG II, Draganov PV. Pancreatic function testing: Here to stay for the 21st century. World J Gastroenterol. 2008; 20: 3149–3158 [PMC: 2712845 ]
- Talamini G. Duodenal Acidity May Increase the Risk of Pancreatic Cancer in the Course of Chronic Pancreatitis: An Etiopathogenetic Hypothesis. JOP. J Pancreas (Online) 2005; 6:122-127 [PMID: 15767727]
- Saunders J H, Wormsley K G. Pancreatic extracts in the treatment of pancreatic exocrine insufficiency. Gut 1975; 16: 157-162. [PMID: 236213]
- Introduction to Enzymes. Worthington Enzyme Manual. Worthington Biochemical Corporation. 2010. https://www.worthington-biochem. com/ introbiochem/default.html
- Mc Clave SA. Feeding the chronically ill patient. Audio-Digest Gastroenterology. 42nd Annual Gastroenterology Update. The Cleveland Clinic, Department of Gastroenterology and Hepatology. 2006.
- Raeder M, Mo A, Aune S. Effect of plasma H+-ion concentration on pancreatic HCO-3 secretion. Acta Physiologica Scandinavica. 2008;105: 420-427 [PMID: 36734]
- Nimmo J, Finlayson NDC, Smith AF, Shearman DJC. The production of calcium and magnesium during pancreatic function tests in health and disease. Gut. 1970; 11: 163–166. [PMID: 5441887]
- Case RM, Harper AA, Scratcherd T. The secretion of electrolytes and enzymes by the pancreas of the anaesthetized cat. J. Physiol. 1969;201:335-348 [PMID: 5780548]
- Benda, J. KarlovarskyMlynskyPramen. Domacipitnalecba. 1997.
- Lee OY, Schmulson M, Mayer EA. Common functional gastrointestinal disorders: Nonulcer dyspepsia and irritable bowel syndrome. Clinical Cornerstone. 1999;1: 57-71 [PMID: 10682182]
- Worning H. Exocrine Pancreatic Function in Dyspepsia. Digestion 1987; 37: 3-13. [PMID: 3497832]
- Okada R, Okada A, Okada T, et al. Elevated Serum Lipase Levels in Patients with Dyspepsia of Unknown Cause in General Practice. Med Princ Pract. 2009; 18: 130-136. [PMID: 19204432]
- Lindström E, Schenck H, Ihse I. Pancreatic exocrine and endocrine function in patients with pancreas divisum and abdominal pain. Int J Pancreatol. 1990; 6: 17-24. [PMID: 2230357]
- Ashizawa N, Hashimoto T, Miyake T, et al. Efficacy of camostatmesilate compared with famotidine for treatment of functional dyspepsia: Is camostatmesilate effective? Journal of Gastroenterology and Hepatology. 2005;21(4):767-771 [PMID: 16677167]
- Andren-Sandberg A, Hardt PD. Second Giessen International Workshop on Interactions of Exocrine and Endocrine Pancreatic Diseases. J Pancreas (Online) 2008; 9: 541-575. [PMID: 18648151]
- Lott JA. Clinical Pathology of Pancreatic Disorders. Humana Press, Totowa, New Jersey. 1997.59.
- Whitcomb DC. Advances in Understanding the Mechanisms Leading to Chronic Pancreatitis. Nat Clin Pract Gastroenterol Hepatol. 2004; 1: 46-52 [PMID: 16265044]
- Green NM, Work E. Pancreatic Trypsin Inhibitor. 2. Reaction with trypsin. Biochem J. 1953; May;54(2):347–352 [PMID: 13058883]
- Niederau C, Grendell JH. Intracellular vacuoles in experimental acute pancreatitis in rats and mice are an acidified compartment. J Clin Invest. 1988;81(1):229–236 [PMID: 3335639]
- Bhoomagoud M, Jung T, Atladottir J, et al. Reducing extracellular pH sensitizes the acinar cell to secretagogue-induced pancreatitis responses in rats. Gastroenterology. 2009; 137: 1083–1092. [PMID: 19454288]
- Hegyi P, Maleth J, Venglovecz V, Rakonczay Z. Pancreatic Ductal Bicarbonate Secretion: Challenge of the Acinar Acid Load. Front Physiol. 2011; 2: 36. [PMID: 21808623]
- Matsuno S, Sasaki Y, Kobari M, et al. Initial Pathophysiological Changes in Chronic Pancreatitis Induced by Pancreatic Ductular Obstruction Model. Tohoku J Exp Med 1991; 163: 199-210. [PMID: 1712129]
- Salo JA, Kivilaakso E. Contribution of trypsin and cholate to the pathogenesis of experimental alkaline reflux esophagitis. Scand J Gastroenterol 1984; 19: 875-881. [PMID: 6531656]
- Cronin J, Williams L, McAdam E, et al. The role of secondary bile acids in neoplastic development in the oesophagus. BiochemSoc Trans 2010; 38: 337-342 [PMID: 20298179]
- Roberto Penagini. Bile reflux and oesophagitis. European Journal of Gastroenterology &Hepatology: 2001; 13: 1-3 [PMID: 11204802]
- Arendt T, Nizze H, Mönig H, Kloehn S, Stüber E, Fölsch UR. Biliary pancreatic reflux-induced acute pancreatitis-myth or possibility? Eur J Gastroenterol Hepatol. 1999; 11: 329-335 [PMID: 10333208]
- Rege RV, Moore EW. Pathogenesis of calcium-containing gallstones. Canine ductular bile, but not gallbladder bile, is supersaturated with calcium carbonate. J Clin Invest. 1986; 77: 21–26 [PMID: 3944252]
- Fitzpatrick W J, Zentler-Munro P L, Northfield T C. Ileal resection: effect of cimetidine and taurine on intrajejunal bile acid precipitation and lipid solubilisation. Gut. 1986; 27: 66–72. [PMID: 3949238]
- Gregg JA. Detection of bacterial infection of the pancreatic ducts in patients with pancreatitis and pancreatic cancer during endoscopic cannulation of the pancreatic duct. Gastroenterology. 1977; 73: 1005- 1007. [PMID: 332575]
- Minelli EB, Benini A, Bassi C, Abbas H, Falconi M, Locatelli F, Marco R, Pederzolli P. Antimicrobial Activity of Human Pancreatic Juice and Its Interaction with Antibiotics. Antimicrob. Agents Chemother. 1996, 40: 2099. [PMID: 8878588]
- Ramare F, Nicoli J, Dabard J, et al. Trypsin-dependent production of an antibacterial substance by a human Peptostreptococcus strain in gnotobiotic rats and in vitro. Appl Environ Microbiol.1993; 59: 2876– 2883. [PMID: 8215361]
- Rubinstein E, Mark Z, Haspel J, et al. Antibacterial activity of the pancreatic fluid. Gastroenterology. 1985 Apr; 88(4):927-32 [PMID: 3882511]
- Pierzynowski SG, Zabielski R. Biology of the pancreas in growing animals. 1999; 131.
- Agraharkar M. et al. Hypercalcemia. 2012. https://emedicine. medscape.com/article/240681- overview
- Wiederkehr M, Krapf R Metabolic and endocrine effects of metabolic acidosis in humans. Swiss Med Wkly 2001; 131; 127-132 [PMID: 11416968]
- Lesniak RJ, Hohenwalter MD, Taylor AJ. Spectrum of Causes of Pancreatic Calcifications. AJR January 2002; 178: 79-86. [PMID: 11756092]
- Mateen MA, Muheet KA, Mohan RJ, Rao PN, Majaz HM, et al. Evaluation of Ultrasound Based Acoustic Radiation Force Impulse (ARFI) and eSie touch Sonoelastography for Diagnosis of Inflammatory Pancreatic Diseases JOP. J Pancreas (Online) 2012; 13: 36-44. [PMID: 22233945]
- Hofmann AF, Mysels KJ. Bile acid solubility and precipitation in vitro and in vivo: the role of conjugation, pH, and Ca2+ ions. Journal of Lipid Research. 1992; 33:617-626 [PMID: 1619357]
- Frassetto L, Morris RC, Sebastian A. Potassium Bicarbonate Reduces Urinary Nitrogen Excretion in Postmenopausal Women. Journal of Clinical Endocrinology and Metabolism 1997; 82: 254-259 [PMID: 8989270]
- Frassetto L, Sebastian A. Age and systemic acid-base equilibrium: analysis of published data. J Gerontol. 1996; 51:91-99. [PMID: 8548506]
- Frassetto L, Morris Jr RC, Sebastian A. Effect of age on blood acid-base composition in adult humans: role of age-related renal functional decline. Am J Physiol. 1996; 271: 1114–1122 [PMID: 8997384]
- Eaton SB, Konner MJ, Cordain L. Diet-dependent acid load, Paleolithic nutrition, and evolutionary health promotion. Am J Clin Nutr 2010; 91: 295–297. [PMID: 20042522]
- Ströhle A, Hahn A, Sebastian A. Estimation of the diet-dependent net acid load in 229 worldwide historically studied hunter-gatherer societies. Am J Clin Nutr 91: 406-412. 2010. [PMID: 20042527]
- Alpern RJ, Sakhaee K. The clinical spectrum of chronic metabolic acidosis: homeostatic mechanisms produce significant morbidity. Am J Kidney Dis. 1997; 29: 291-302. [PMID: 9016905]
- Sebastian A, Frassetto LA, Sellmeyer DE, Merriam RL, Morris RC. Estimation of the net acid load of the diet of ancestral preagricultural Homo sapiens and their hominid ancestors. Am J Clin Nutr 2002; 76: 1308-1316. [PMID: 12450898]
- Vormann J, Remer T. Dietary, Metabolic, Physiologic, and Disease- Related Aspects of Acid-Base Balance: Foreword to the Contributions of the Second International Acid-Base Symposium. J. Nutr 2008; 138: 413- 414. [PMID: 18203912]
- Gullo L. Alcohol and Chronic Pancreatitis: Leading or Secondary Etiopathogenetic Role? JOP. J Pancreas (Online) 2005; 6: 68-72. [PMID: 15650289]
- Irving HM, Samokhvalov AV, Rehm J. Alcohol as a Risk Factor for Pancreatitis. A Systematic Review and Meta-Analysis. JOP. J Pancreas (Online) 2009; 10: 387-392. [PMID: 19581740]
- Criddle DN1, Raraty MG, Neoptolemos JP, Tepikin AV, Petersen OH, et al. Ethanol toxicity in pancreatic acinar cells: Mediation by nonoxidative fatty acid metabolites. Proc Natl Acad Sci USA. 2004; 101: 10738–10743. [PMID: 15247419]
- Solc, P. Karlovarskalazenskaleba a medicinanaprelomu 20. A21. Stoleti. 2000.
- Peter Melamed, PhD, Felix Melamed, LAc, MSTCM, CHt. Healthy Pancreas, Healthy You. Part II. Healing Foods in the Digestive (Pancreatic) Disorders. EBook 2012, Biotherapy, Inc, San Francisco. https://www.smashwords.com/books/view/240466
- Judge BS. Metabolic Acidosis: Differentiating the Causes in the Poisoned Patient. Med Clin N Am 2005; 89: 1107–1124 [PMID: 16227056]
- Gunnerson KJ, Pinsky MR. Lactic Acidosis. https://emedicine.medscape.com/article/167027-overview.
- Hisato Igarashi at al Acetaminophen-Induced Acute Pancreatitis. A Case Report. JOP. J Pancreas (Online) 2009; 10: 550-553. [PMID: 19734636]
- rulloni L, Patrizi F, Bernardoni L, Cavallini G. Pancreatic Hyperenzymemia: Clinical Significance and Diagnostic Approach. JOP. J Pancreas (Online) 2005; 6: 536-551. [PMID: 16286704]
- Liamis G et al. Pharmacologically-Induced Metabolic Acidosis. Drug Saf. 2010; 33: 371-391. [PMID: 20397738]
- Burckhardt P. The effect of the alkali load of mineral water on bone metabolism: interventional studies. J Nutr 2008 Feb;138(2):435S- 437S [PMID: 18203918]
- McCance K, Huether S. Pathophysiology: the biologic basis for diseases in adults and children. 2nd ed. 1994, Mosby.

