Keywords
Myocardial infarction; Chronic total occlusion; Acute coronary syndromes; Left ventricular failure (LV); Multivessel coronary artery disease (MVD)
Introduction
Acute coronary syndromes (ACS) include patients with myocardial infarction with ST-segment elevation (STEMI), with myocardial infarction without ST-segment elevation (NSTEMI) and unstable angina (UA). Multivessel coronary artery disease (MVD) occurs in approximately 45% to 80% of patients with ACS, depending on both the type and the onset of ACS and many other cardiovascular risk factors [1-3]. The presence of multivessel disease is associated with worse overall prognosis in this group of patients [4].
Chronic total occlusion of coronary artery (CTO), defined as total vessel occlusion lasting more than 3 months with the assessment of blood flow in the artery at the level of TIMI 0-1, occurs in about 30% of patients with coronary artery disease (CAD) [5]. Some studies have shown that in patients with MVD worse prognosis concerns patients with the existence of chronic coronary artery occlusion, other than infarct related artery (non-IRA).
Coronary arteries demonstrate between individuals variable range of cardiac vasculature expressing the dominance of the right (in about 87% to 89%), the left coronary artery (in about 7% to 8%) or their “codominance” (up to 4%) [6-9]. It has been suggested that the presence of the left coronary artery dominance (LD) may be an independent predictor of mortality in patients with ACS [9,10], and/or of non-fatal myocardial infarction in patients with stable CAD [9].
Due to suggested in the literature a worse prognosis in patients with CTO [11] and a domination of the left coronary artery [9], there were made the attempts to compare these groups of patients in terms of clinical characteristics, the degree of the left ventricle (LV) damage in echocardiography and survival at follow-up. A similar analysis was also performed within the group of patients with the coexistence of these two adverse prognostic features.
Methods
Consecutive patients hospitalized in 2009-2010 in our Cardiology Department and who underwent coronary angiography because of ACS were observed retrospectively (n = 682). Based on angiographic images only 402 patients with MVD were extracted. In one third of these patients non-IRA CTO was found. The type of coronary artery dominance was specified. MVD was defined as the presence of min. 50% stenosis in at least two of the epicardial coronary arteries. The presence of at least one CTO of non-IRA with the vessel diameter greater than 2 mm was the qualifying CTO group criterion. The assessment of dominance was based on the criteria proposed by the guideline of American Heart Association [9,12].
As the dominance of the right coronary artery (RCA) the presence of posterior descending artery (PDA) extending from the RCA was adopted (Figure 1), whereas the dominance of the left coronary artery (LCA) was recognized for PDA’s departure from the circumflex artery (LCx-photo 2). The equivalent system of coronary vasculature was assumed as PDA’s departure from RCA with the simultaneous presence of a large postero-lateral branch diverging from the LCx and running around within the back interventricular groove. Angiographic assessment was carried out independently by two invasive cardiologists. The degree of the left ventricular damage was determined on the basis of ejection fraction (EF) by echocardiography performed during index hospitalization. Follow-up consisted of data from the hospital documentation and conducted telephone interviews during an average 466- day period (median 285 days) since the time of the ACS.
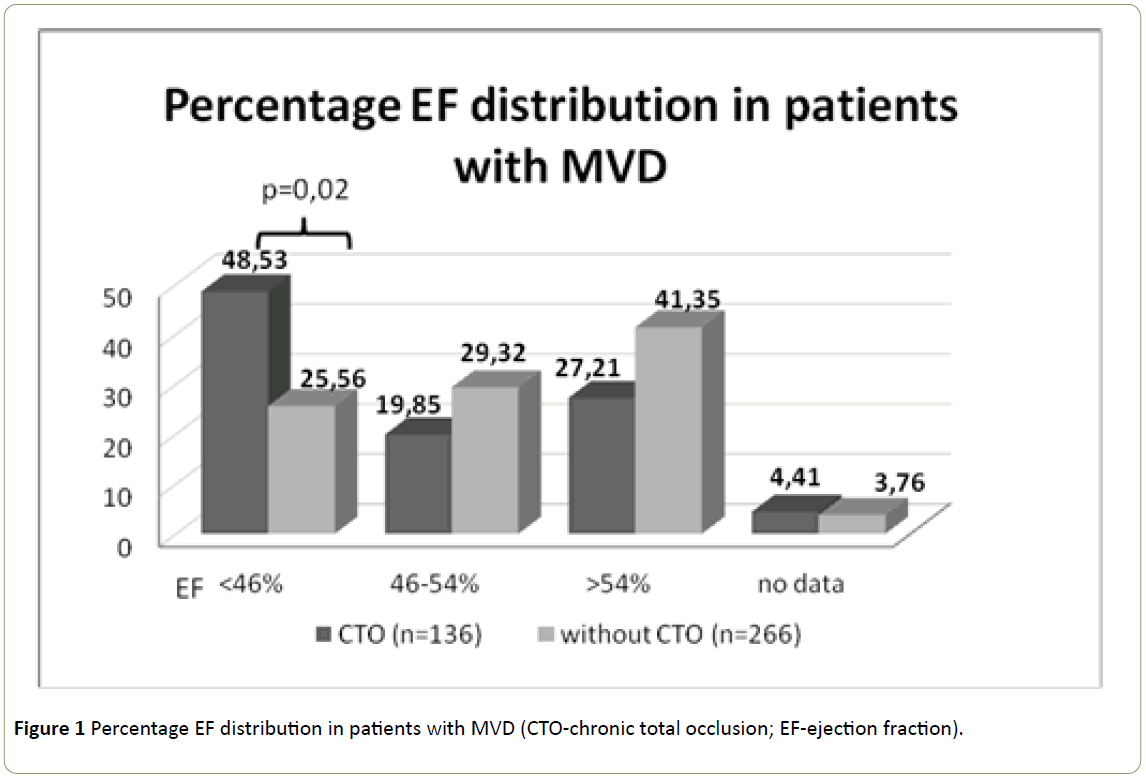
Figure 1: Percentage EF distribution in patients with MVD (CTO-chronic total occlusion; EF-ejection fraction).
Statistical Analysis
Continuous variables were expressed as mean value standard deviation, median and were analyzed by Student's t test. Categorical variables were expressed as numbers and/or percentages. Comparative statistics using the chi-square test with Yates correction for discontinuity or Fisher's exact test were performed. Graphic Kaplan-Meier method was used to describe survival in follow-up. P-value equal to or less than 0.05 were considered statistically significant.
Results
There were 402 consecutive patients undergone PCI because of ACS with MVD subsequently enrolled in this study. As many as 136 (33.8%) patients had at least one non-IRA CTO. Only 44 (10.95%) patients showed the dominance of LCA, 336 (83.58%) had RCA as the dominant one, and in 22 (5.47%) patients an equivalent coronary system was diagnosed.
In patients with CTO 18 of them (13.24%) showed the dominance of LCA, 108 (79.41%) RCA dominance, while an equivalent system was diagnosed in 10 (7.35%). Due to the small number of patients with the equivalent coronary artery system these data were not subjected to statistical analysis.
Clinical characteristics
The comparative characteristics of CTO vs non-CTO patients in individual groups was shown in Table 1.
| |
CTO (n=136) |
no CTO (n=266) |
p |
CTO+LD (n=18) |
no CTO+LD (n=26) |
p |
no CTO+RD (n=228) |
CTO+RD (n=108) |
p |
| Age: average ± SD (median) |
69.2 ± 11.9 (70) |
65.1 ± 11.3
-63 |
<0.001 |
72.1 ± 12.0
(74) |
63.7 ± 13.5
-62 |
0.04 |
65 ± 11.1
(63.5) |
69.6 ± 11.5
-70 |
<0.001 |
| Female |
27.20% |
34.50% |
0.3 |
44% |
38.40% |
0.8/0.9 |
33.30% |
27% |
0.4 |
| Hypertension |
88.20% |
83% |
0.7 |
94% |
77% |
0.7/0.9 |
82.30% |
86.10% |
0.8 |
| Hiperlipidemia |
78% |
79.30% |
0.9 |
83% |
73% |
0.77/0.95 |
81% |
76.80% |
0.7 |
| Diabetes |
20.60% |
12.80% |
0.08 |
5.50% |
15.40% |
0.36/0.67 |
13% |
24% |
0.05 |
| Renal failure |
16.20% |
5.30% |
0.001 |
16.70% |
3.80% |
0.18/0.42 |
5.30% |
15.70% |
<0.001 |
| Peripheral atherosclerosis |
9.60% |
3.60% |
0.04 |
11.10% |
3.80% |
0.38/0.78 |
4.00% |
9.30% |
0.06/0.11 |
| Post MI |
59.60% |
19.50% |
<0.001 |
72% |
11.50% |
0.005/0.01 |
19% |
57.40% |
<0.0001 |
| Post PCI |
20.60% |
14% |
0.14 |
22% |
7.70% |
0.23/0,45 |
19% |
18.50% |
0.95 |
| Post CABG |
10.30% |
0% |
<0.001 |
16.70% |
0% |
0.04/0.16 |
0% |
9.30% |
<0.0001 |
| Killip-Kimball 2-4 Class |
9.60% |
3.40% |
0.02 |
0% |
3.80% |
0.4/0.8 |
2.60% |
12% |
0.01/0.02 |
| CTO-chronic total occlusion; LD-left coronary artery dominance; RD-right coronary artery dominance After slash p-values are given for c2 test with Yate’s correction |
Table 1: Comparative characteristics of individual groups of patients.
In terms of clinical characteristics and cardiovascular risk factors in MVD patients without CTO statistically significant differences between groups with the dominant LCA and RCA were not observed, similarly as in CTO patients between groups with the dominant left vs right coronary artery (Table 2).
| |
LD (n=44) |
RD (n=266) |
p |
CTO+LD (n=18) |
no CTO+RD (n=108) |
p |
| 67.1+ -13.5 (66) |
66.5 +-11.4 (66) |
0.7 |
72.1 +-12.0 (74) |
69.6 +-11.5 (70) |
0.4 |
| Female |
41% |
31.30% |
0.4 |
44% |
27% |
0.3/0.4 |
| Hypertension |
84% |
84% |
0.9 |
94% |
86.10% |
0.8/0.95 |
| Hiperlipidemia |
77.30% |
79.40% |
0.9 |
83% |
76.80% |
0.83/0.98 |
| Diabetes |
11.40% |
16,40% |
0.5 |
50.50% |
24% |
0.13/0.23 |
| Renal failure |
9% |
8,60% |
0.9 |
16.70% |
15.70% |
0.93/0.79 |
| Peripheral atherosclerosis |
6.80% |
5,70% |
0.8 |
11.10% |
9.30% |
0.83/0.84 |
| Post MI |
36% |
31.80% |
0.7 |
72% |
57.40% |
0.6/0.7 |
| Post PCI |
13.60% |
16.10% |
0.7 |
22% |
18.50% |
0.87 |
| Post CABG |
60.80% |
3% |
0.3 |
16.70% |
9.30% |
0.4/0.66 |
| Killip-Kimball 2-4 Class |
2.30% |
5.70% |
0.4 |
0% |
12% |
0.14/0.3 |
| CTO-chronic total occlusion; LD-left coronary artery dominance; RD-right coronary artery dominance. After slash p-values are given for c2 test with Yate’s correction |
Table 2: Comparative characteristics of individual groups of patients.
ACS distribution
Graphical and statistical analysis of ACS distribution in different groups of patients is shown in Figure 2.

Figure 2: ACS distribution in individual groups of patients (CTO-chronic total occlusion; LD-left coronary artery dominance; RD-right coronary artery dominance).
Echocardiography
Echocardiographical EF assessment in separate groups of patients was presented in Figures 3-6.
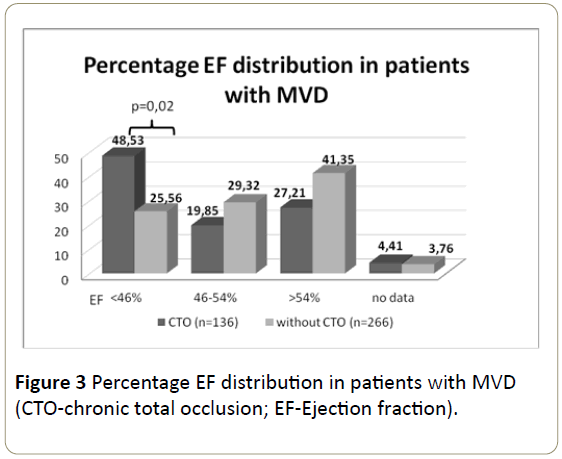
Figure 3: Percentage EF distribution in patients with MVD (CTO-chronic total occlusion; EF-Ejection fraction).
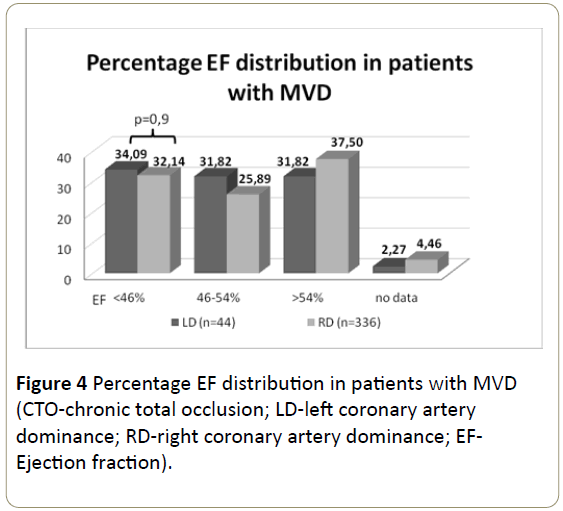
Figure 4: Percentage EF distribution in patients with MVD (CTO-chronic total occlusion; LD-left coronary artery dominance; RD-right coronary artery dominance; EFEjection fraction).
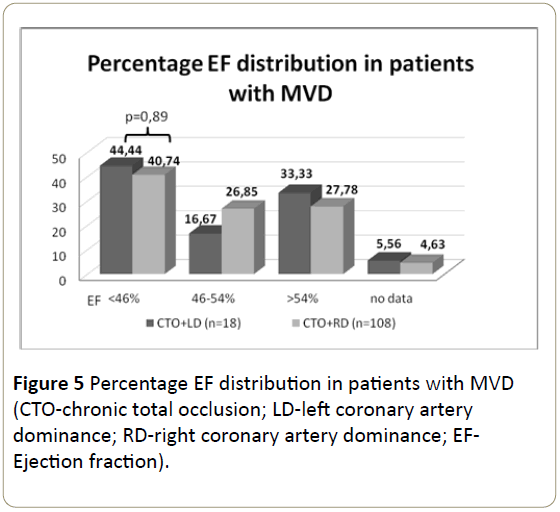
Figure 5: Percentage EF distribution in patients with MVD (CTO-chronic total occlusion; LD-left coronary artery dominance; RD-right coronary artery dominance; EFEjection fraction).
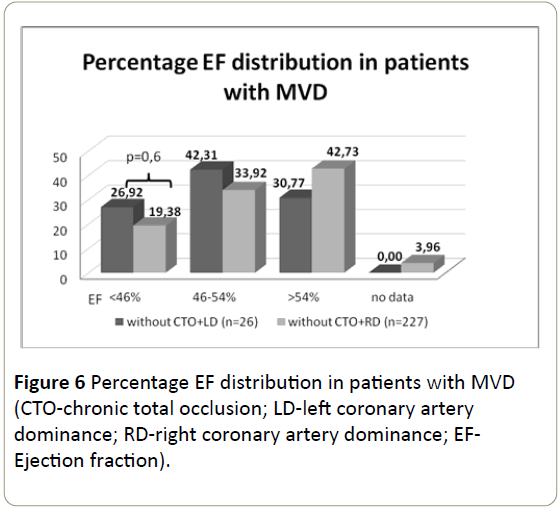
Figure 6: Percentage EF distribution in patients with MVD (CTO-chronic total occlusion; LD-left coronary artery dominance; RD-right coronary artery dominance; EFEjection fraction).
Follow-up
The all-cause, average 466-day mortality of 682 patients during follow-up was 10.98%. Mortality during the observation period in the group of 276 patients with single-vessel
coronary artery disease amounted to 7.97%, while the mortality in the group of 402 patients with MVD was 13.18% (p = 0.15).
In patients with CTO and dominant LCA (n = 18) the allcause mortality was 28% while in the group with CTO and dominant RCA (n = 108) amounted to 17% (p = 0.55). In both groups the prognoses were worse if the myocardial infarction concerned dominant coronary artery (p = 0.8). The survival curves are shown graphically in Graphs 1-3.
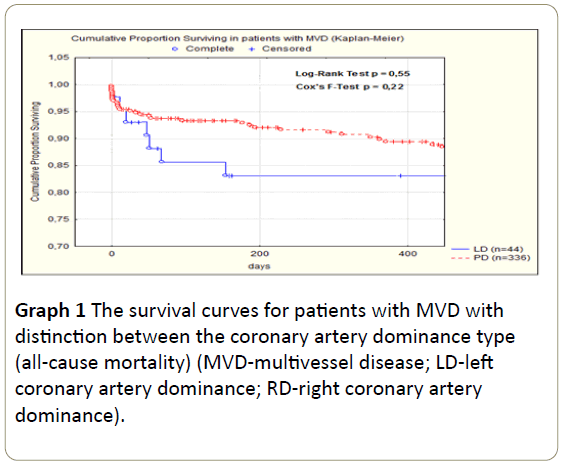
Graph 1: The survival curves for patients with MVD with distinction between the coronary artery dominance type (all-cause mortality) (MVD-multivessel disease; LD-left coronary artery dominance; RD-right coronary artery dominance).
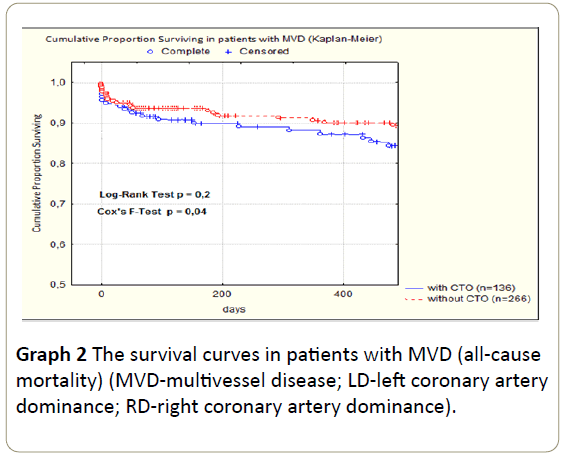
Graph 2: The survival curves in patients with MVD (all-cause mortality) (MVD-multivessel disease; LD-left coronary artery dominance; RD-right coronary artery dominance).
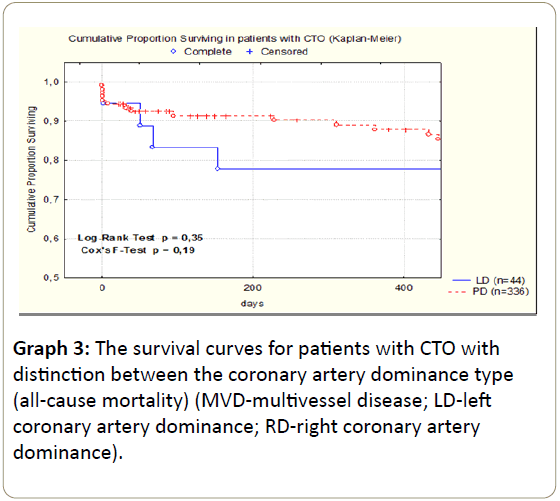
Graph 3: The survival curves for patients with CTO with distinction between the coronary artery dominance type (all-cause mortality) (MVD-multivessel disease; LD-left coronary artery dominance; RD-right coronary artery dominance).
In patients without CTO coronary dominance type did not affect the differences in the all-cause mortality (p = 0.96).
Discussion
In the present study patients with MVD hospitalized because of ACS were analyzed. Patients with non-IRA CTO compared to patients without CTO demonstrated to have been of the higher age at the time of index ACS, having more cardiovascular risk factors and more advanced atherosclerotic disease, and they also suffered from concomitant diseases affecting their prognosis.
A worse clinical condition of these patients on admission to hospital assessed by Killip-Kimball scale and significantly more often history of coronary artery bypass grafting also draws the attention. Also, more likely they suffered from diabetes. In patients with CTO significantly more frequent cause of hospitalization was NSTEMI, whereas in patients without CTOSTEMI.
This pattern was observed regardless of the type of coronary artery dominance. Since patients with CTO have more risk cardiovascular factors-as one might expect-they have a significantly greater degree of LV damage and their tendency to higher mortality and worse prognosis was demonstrated.
It is believed that in these patients the pathophysiological substrate of increased mortality is multifactorial. The possible reperfusion disturbances after the restoration of IRA patency, postreperfusion cardiomyocyte damage and microvascular ischemia with the coexistence of CTO also increases the area of heart muscle damage. Furthermore, if the artery responsible for the ACS is a source of collateral circulation to the area of chronically occluded artery vasculature, the above phenomena are particularly pronounced.
Similar conclusions were presented in the study by Claessen et al. [11], where it has been shown that in patients with STEMI undergoing primary PCI, the presence of CTO in a non- IRA is an independent predictor of early and late mortality. The results of our study on cardiovascular risk factors and LV damage extent in these patients are convergent with ones described in this announcement. However, in our observation the higher percentage of all-cause and cardiovascular mortality during follow-up in patients with CTO may be due to the fact, that in contrast to the literature quoted above less homogeneous group of patients with MVD undergoing coronary angioplasty including all types of ACS was enrolled. It is known that patients with NSTEMI have worse prognosis in long-term follow-up, which may have had a greater impact on mortality rate in our group.
When comparing patients with RD or LD in terms of the prevalence of cardiovascular risk factors and the degree of LV damage there were no significant differences. Moreover, the coexistence of CTO also had no effect on clinical differences between the two groups (Table 2).
Nevertheless, a slight trend toward higher mortality and a worse long-term prognosis for patients with LD can be noted. The study by Veltman et al. [9] showed that the presence of LD is associated with a statistically significant increased risk of nonfatal reinfarction. It is noteworthy that in the quoted study patients with LD compared to patients with RD did not differ in baseline cardiovascular risk, similarly like in our observations.
The discrepancies regarding the statistical significance for prognosis between our study and the announcement by Veltman et al. [9] may result from both: a way of assessing coronary vasculature (computed tomography angiography vs invasive coronarography) and the selection of observed patients (patients with ACS and MVD vs patients with suspected coronary artery disease in Veltman’s trial).
Analyzing the group of subjects with CTO and LD coexistence, one may note a trend to a higher incidence of at least moderate LV dysfunction (Figure 4) which, however, does not translate into a significant increase in mortality compared to patients without CTO and RD coexistence.
Conclusions
In summary, it seems that the main factor differentiating the prognosis is rather the presence of non-IRA CTO than coronary artery dominance type. However, as the presence of LD in some study groups may be an additional, negative cardiovascular risk factor, it seems appropriate to extend the observation of this subjects.
Limitations
The relatively short observation time and lack of clinical and echocardiographic assessment of all patients in the subsequent years after ACS may have a significant impact on the analysis of individual patients’ prognosis. Moreover, the group of patients with CTO comprised subjects with non-IRA CTO of a vessel diameter greater than 2 mm, taking in to account neither the vasculature extent nor primary or secondary arterial branches. As the CTO prevalence in the epicardial arteries goes for: LAD-over 30%, LCx-over 20% and RCA-over 40% [13,14]. It is known that the above mentioned factors seems to play an important role in the formation of collaterals and indeed in the given myocardial survival which obviously influences follow-up. A small number of patients in each group, especially in patients with left coronary artery dominance could also affect the result of these data analysis.
References
- Sorajja P, Gersh BJ, Cox DA, McLaughlin MG, Zimetbaum P, et al. (2007) Impact of multivessel disease on reperfusion success and clinical outcomes in patients undergoing primary percutaneous coronary intervention for acute myocardial infarction. Eur Heart J 28: 1709-1716.
- Pres D, G?sior M, Polo?ski L (2010) Treatment of patients with coronary artery disease and diabetes mellitus. Art Hypertens 7: 112-117
- Sukiennik A, Król A, Jachalska A, Kozi?ski M, Fabiszak T (2007) Percutaneous coronary angioplasty in elderly patients: Assessment of in-hospital outcomes. Cardiol J 14: 143-154.
- Corpus RA, House JA, Marso SP, Grantham JA, Huber KC Jr, et al. (2004) Multivessel percutaneous coronary intervention in patients with multivessel disease and acute myocardial infarction. Am Heart J 148: 493-500.
- Bryniarski L, Zabojszcz M, Bryniarski K, Terlecki M (2010) Knowledge about chronic total coronary artery occlusions among Polish physicians. Post Kardiol Interw 6: 66-70.
- Claessen BE, van der Schaaf RJ, Verouden NJ, Stegenga NK, Engstrom AE, et al. (2009) Evaluation of the effect of a concurrent chronic total occlusion on long-term mortality and left ventricular function in patients after primary percutaneous coronary intervention. JACC Cardiovasc Interv 2: 1128-1134.
- Claessen BE, Hoebers LP, van der Schaaf RJ, Kikkert WJ, Engstrom AE (2010) Prevalence and impact of a chronic total occlusion in a non-infarct-related artery on long-term mortality in diabetic patients with ST elevation myocardial infarction. Heart 96: 1968-1972.
- Lexis CP, van der Horst IC, Rahel BM, Lexis MA, Kampinga MA, (2011) Impact of chronic total occlusions on markers of reperfusion, infarct size, and long-term mortality: a substudy from the TAPAS-trial. Catheter Cardiovasc Interv 77: 484-491.
- Veltman CE, de Graaf FR, Schuijf JD, van Werkhoven JM, Jukema JW, et al. (2012) Prognostic value of coronary vessel dominance in relation to significant coronary artery disease determined with non-invasive computed tomography coronary angiography. Eur Heart J 33: 1367-1377.
- Goldberg A, Southern DA, Galbraith PD, Traboulsi M, Knudtson ML, Ghali WA (2007) Alberta Provincial Project for Outcome Assessment in Coronary Heart Disease (APPROACH) Investigators. Coronary dominance and prognosis of patients with acute coronary syndrome. Am Heart J 154: 1116-1122.
- Claessen BE, Dangas GD, Weisz G, Witzenbichler B, Guagliumi G, et al. (2012) Prognostic impact of a chronic total occlusion in a non-infarct-related artery in patients with ST-segment elevation myocardial infarction: 3-year results from the HORIZONS-AMI trial. Eur Heart J 33: 768-775.
- Austen WG, Edwards JE, Frye RL, Gensini GG, Gott VL, et al. (1975) A reporting system on patients evaluated for coronary artery disease. Report of the Ad Hoc committee for grading of coronary artery disease, Council on Cardiovascular Surgery, American Heart Association. Circulation 51: 5-40
- Claessen BE, Dangas GD, Godino C, Henriques JP, Leon MB, et al. (2013) Multinational CTO Registry. Impact of target vessel on long-tern survival after percutaneous coronary intervention for chronic total occlusions. Catheter Cardiovasc Interv 82: 76-82.
- Hasegawa T, Godino C, Basavarajaiah S, Takagi K, Rezq A, et al. (2014) Differences in the clinical and angiographic characteristics of chronic total occlusion lesions in the three major coronary arteries. J Interv Cardiol 27: 44-49.

