Anuna Laila Mathew* and Sunu Alice Cherian
Department of Oral Medicine and Radiology, Pushpagiri College of Dental Sciences, India
*Corresponding Author:
Anuna Laila Mathew
Associate Professor, Department of Oral Medicine and Radiology
Pushpagiri College of Dental Sciences, Medicity, Tiruvalla
Kerala, India.
Tel: +91 8547431225
Email: drmathewdan@yahoo.co.in
Received date: November 25, 2016; Accepted date: November 29, 2016; Published date: December 05, 2016
Citation: Mathew AL, Cherian SA (2019) Combined Factor V and VIII Deficiency- A Rare Case with Dental Management. J Ora Med Vol.3 No.1:1
Copyright: © 2019 Mathew AL, et al. This is an open-access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
Keywords
Combined; Factor V; Factor VIII; Hemorrhagic disorder; Fresh frozen plasma; DDAVP
Introduction
Most important hereditary bleeding disorder in terms of prevalence and severity is von Willebrand’s disease, but hemophilia A and B are the other common congenital coagulation defects [1]. Familial multiple coagulation factor deficiency is a group of rare autosomal recessive inherited disorders with the deficiency of one or more coagulation factors. Usually, it is misdiagnosed as hemophilia A or some other factor deficiency [2]. As the bleeding tendencies are less and postoperative complications are rare, it goes undiagnosed. It is usually seen in consanguineous marriage. Dental considerations of these patients are important for the management of such patients in dental practice.
Case Report
A seven-year-old female child reported to the dental OPD with the complaint of a decayed tooth in the lower left posterior region of the jaw since six months. Initially, around the fourth month, she had mild, sharp pain on food impaction and was asymptomatic since two months.
Parents noticed large areas of bluish-red discoloration following trauma, bleeding following exfoliation of deciduous teeth since childhood, and also occasional epitasis and hematoma formation following intramuscular injections. No history of spontaneous bleeding into joints, muscles, bleeding on brushing or hematuria.
The patient had a history of consanguineous marriage of parents. Patient’s great grandmother, grant mother’s sister and her granddaughter have a positive history of bleeding. Intraoral examination revealed mixed dentition, root stumps of 75 (FDI classification), deep dentinal caries on 74 (Figure 1).
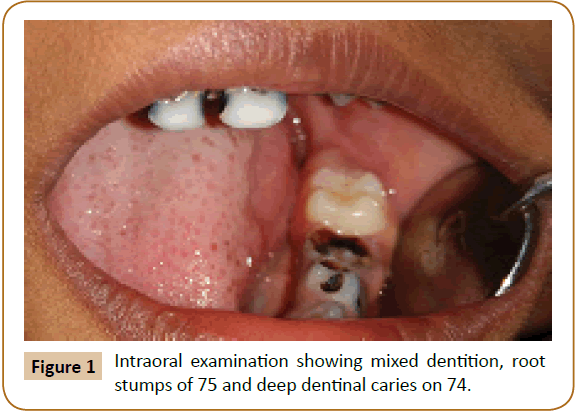
Figure 1: Intraoral examination showing mixed dentition, root stumps of 75 and deep dentinal caries on 74.
Routine hemogram showed Hemoglobin 10.9 gm%, total count and differential count were within the normal limits, bleeding time >5 minutes, (normal:2-6 minutes), clotting time- 11minutes, (normal:3-10 minutes), prothrombin time (PT) 22.4 seconds, (normal:11.4 seconds), activated partial thromboplastin time (aPTT) 57.9 seconds (control - 28.2 seconds), international normalized ratio (INR) 2.
Physician consultation was advised. Patient was referred to a hematologist and the following coagulation work up and Von Willebrand’s factor assay was done that showed that vWF was not deficient, and mixing study for factor assay was done. The mixed factor assay suggested combined factor V & VIII deficiency of 30% and 50% (Familial multiple clotting factor deficiency, type 1). Patient was advised to go for extraction of the root stump. Preoperatively rinsing with cholrhexidine mouth wash for 2 minutes before the administration of local infiltration was advised, extraction was done as atraumatically as possible, suturing of the socket was done with absorbable sutures. In our case the hematologist or the physician did not advise for any oral rinse like Amicar.
Minimal post extraction bleeding for one hour which subsided with pressure and pack. Deep caries management was done in all the carious teeth.
Conclusion and Discussion
Combined deficiency of factor V (F5) & factor VIII (F8) was first described in a pair of Swiss siblings in 1954 [2,3]. High incidence has been reported in consanguineous marriages. Inheritance of F5F8D is autosomal recessive. It is caused by a gene defect on chromosome 18. First gene for F5F8D reported in 1998 is LMAN1. Till 2006, around 138 patients in 81 families have been diagnosed with F5F8D, in which more than half of families were from, Israel, Iran, and Italy [4]. Families have also been reported from Thailand, India, Japan, North America, non-Ashkenazi Jews and Europe [5]. Most of the cases were not diagnosed properly due to mild bleeding manifestations and were misdiagnosed as having mild hemophilia A or parahemophilia (Factor V deficiency) [6,7]. It is more prevalent among Middle-Eastern Jews and non- Jewish Iranians, approximately 1:100000 [7].
Combined factor V and VIII deficiency affects both males and females equally. The chances of inheriting factor V and factor VIII deficiency are 1 in 10,00,000 and 1 in 10,000 respectively. Therefore, the chances of inheriting both defective genes are 1 in 10 billion.
Clinical Manifestation
Bleeding symptoms appear to be comparable with single factor deficiency of F5 or F8. Spontaneous bleeding is uncommon; tendencies for easy bruising, epistaxis and menorrhagia have also been reported. Hemarthroses, gastrointestinaI bleed, hematuria, and intracranial bleed are rare. Excessive bleeding is common during or after trauma, like tooth extraction, surgery or labor.
The levels of F5 & F8 correlate with bleeding severity.
Life threatening bleeding is rare. Fresh frozen plasma is effective in life threatening hemorrhage. Factor VIII concentrate, Desmopressin (trade name DDAVP) also raises the factor VIII. DDAVP is used in mild to moderate bleeding; it can be used in combination with plasma infusion.
Considerations for Dental Treatment
Periodontal treatment
In severe periodontal disease, supra gingival scaling is advised. Subgingival scaling can be done when the inflammation decreases. Periodontal problems can be controlled by mouthwashes [8- 10]. Blood loss can be controlled locally with direct pressure or periodontal dressings with or without topical antifibrinolytic agents. Periodontal surgery is a high-risk procedure and has to be clearly explained and factor replacement is indicated.
Prosthodontics
Dentures can be given if the patient is comfortable with it. If removable partial denture is provided, the health of the remaining teeth has to be assessed.
Orthodontic treatment
Fixed and removable orthodontic appliances may be used with preventive measures.
Restorative procedures
Restorative treatment can be done providing care to protect the mucosa. Bleeding caused by the usage of matrix band and wooden wedges can be controlled by local measures like application of topical agents. If pulpectomy is indicated, do not perforate the apex [8-10].
Surgery
Simple extraction must be planned to minimize the risk of bleeding, excessive bruising or hematoma formation. If multiple extractions are required, only one or two teeth should be extracted in the first appointment to ensure that hemostasis can be achieved.
Perioperative period
Rinse with chlorhexidine mouth wash for two minutes before the administration of local anesthetic. Extraction should be done as atraumatically as possible. Suture the socket with absorbable sutures. Use local hemostatic measures and soft vacuum formed splint to protect the socket. Risk in airway obstruction due to inferior alveolar nerve block can be reduced by the use of the Gow-Gates technique. Local infiltration and periodontal ligament injection can be considered [11,12].
Postoperative period
No rinsing of mouth, or smoking, soft diet and no strenuous activities for 24 hours. Salt water gargling can be done, the day following extraction for 7 days.
Managing post-operative bleeding
Any bleeding point should be treated using local measures. Instruct the patient to sit up and bite on a 10% solution of Tranexamic acid damp gauze swab for at least 10 minutes. If patient has pain analgesic should be given.
The dental surgeon must enhance awareness among patients to improve the oral hygiene. Dentist must be prepared to deal with complications in a calm and efficient manner [10-12].
References
- Peyvandi F, Mannucci PM (1999) Rare coagulation disorders. Thromb Haemost 82: 1207-1214.
- Sadler JE (1997) Combined factors of V and VIII climbs on to the map. J Clin Invest 99: 555-556.
- Mansouritorghabeh H (2007) Combined factor V and factor VIII deficiency. Iran J Med Sci 32: 130-135.
- Dansako H, Ishimaru F, Takai Y (2001) Molecular characterization of the ERGIC-53 gene in two Japanese patients with combined factor V and factor VIII deficiency. Ann Hematol 80: 292-294.
- Mansouritorghabeh H, Rezaieyazadi Z, Pourfathollah AA (2004) Hemorrhagic symptoms in patients in patients with combined factor V and factor VIII deficiency in north-eastern Iran. Haemophilia 10: 271-275.
- Shetty S, Madkaikar M, Nair S (2000) Combined factor V and factor VIII deficiency in Indian population. Haemophilia 6: 504-507.
- Seligsohn U, Zivelin A, Zwang E (1982) Combined factor V and factor VIII deficiency among non-Ashkenazi Jews. N Eng J Med 307: 1191-1195.
- Jover-Cervero A, Poveda-Roda R, Bagan JV, Jimenez- Soraiano Y (2007) Dental treatment of patients with coagulation factor alterations: An update. Med Oral Patol Oral Cir Bucal 12: E380-387.
- Gomez-Moreno G, Cutando-Soriano A, Arana C, Scully C (2005) Hereditary blood coagulation disorders: management and dental treatment. J Dent Res 84: 978-985.
- Mannucci PM (1997) Desmopressin (DDAVP) in the treatment of bleeding disorders; the first 20 years. Blood 90: 2515-2521.
- Di Paola J, Nugent D, Young G (2001) Current therapy for rare factor deficiencies. Haemophilia 7: 16-22.
- Little JW, Falace DA, Miller CS, Rhodus NL (2002) Dental management of medically compromised patient. (6th ed), Mosby, Pp: 358-363.

