Keywords
Antibodies, Monoclonal; cetuximab; erlotinib; gefitinib; Pancreatic Neoplasms; Protein Kinase Inhibitors; Radiotherapy; Receptor, Epidermal Growth Factor
Abbreviations
NCIC-CTG: National Cancer Institute of Canada Clinical Trials Group; TKI: tyrosine kinase inhibitors
Introduction
When overexpressed or inappropriately activated, epidermal growth factor receptor (EGFR) promotes a variety of oncogenic activities in human cells, including uncontrolled proliferation, angiogenesis, and inhibition of apoptosis. [1]. EGFR is frequently over expressed in pancreatic cancer [2] and overexpression is correlated with poor prognosis [3]. EGFR has been investigated as a target for systemic therapy in pancreatic cancer using both small-molecule tyrosine kinase inhibitors (TKI) and monoclonal antibodies against the extracellular domain of the EGFR.
Inhibiting EGFR appears to sensitize tumor cells to ionizing radiation, either through increasing the proportion of cells in the radiosensitive G1 phase of the cell cycle while decreasing the proportion in the radioresistant S phase [4], or through restoration of apoptosis [5] or even anti-angiogenic mechanisms [6]. Preclinical data suggests that adding EGFR inhibitors can increase the activity of gemcitabine and radiation in pancreatic cancer cell lines and tumors [7, 8]. The publication of the randomized clinical trial in locallyadvanced head-and-neck squamous cell carcinoma by Bonner et al. in 2006 was a watershed event that provided clinical validation for the combination of EGFR inhibitors with radiation [9]. The addition of cetuximab to radiation therapy led to a 10% absolute increase in three-year survival (55% versus 45%) and increased local control (50% versus 41%) compared with radiation alone.
A Ray of Hope?
In 2005, results of a National Cancer Institute of Canada Clinical Trials Group (NCIC-CTG) randomized study lead to the approval of erlotinib, a small-molecule inhibitor of EGFR, for use in combination with gemcitabine in unresectable, chemotherapy-naïve pancreatic cancer [10]. Although the NCIC-CTG trial was deemed successful, the 2- week survival benefit associated with the addition of erlotinib to gemcitabine was so modest that many oncologists questioned its clinical relevance. Furthermore, the rate of complete plus partial responses was only 8.6%, versus 8.0% in the gemcitabine-alone arm, suggesting that erlotinib has, at best, marginal anti-tumor activity. In light of the moderate incremental benefit of adding EGFR inhibition to chemotherapy and the known radiosensitizing properties of EGFR inhibitors, could combining EGFR inhibition, chemotherapy, and radiation therapy improve outcomes in localized pancreatic cancer?
Radiation Therapy and Pancreatic Cancer
Pancreatic cancer patients generally receive radiation either in the adjuvant setting, following a definitive resection, or for locally advanced, non-metastatic disease, in which no such surgery is possible. Although there is considerable controversy as to the exact benefit of radiotherapy in pancreatic cancer, there is randomized phase III data to support the use of radiation and chemotherapy both in the adjuvant [11] and locally advanced [12, 13] settings. In adjuvant therapy, the radiation fields typically encompass the tumor bed, the anastomoses and the regional lymphatics, in order to enhance locoregional control by sterilizing occult microscopic disease within the field. In treatment of locally advanced disease, some institutions have adopted a strategy of highly conformal therapy, treating only the gross tumor with a margin [14] while omitting the uninvolved lymphatics. Systemic therapies are generally thought to enhance the efficacy of radiation in two ways: by increasing the ability of radiation to kill tumor cells in the radiation field (radiosensitization), and by eliminating micrometastatic disease outside of the field (spatial cooperation). Given the potential of EGFR inhibitors as radiosensitizing agents, it makes sense that the benefits of combination therapy in pancreatic cancer should be evident in terms of increased local disease control.
Clinical Trials of EGFR Inhibitors and Radiation in Pancreatic Cancer
Tables 1 and 2 summarize the efficacy and toxicity, respectively, of different combinations of EGFR inhibitors, radiation, and chemotherapy in pancreatic cancer. The principal small-molecule EGFR inhibitors to be investigated in pancreatic cancer are gefitinib and erlotinib. Gefitinib was studied in combination with capecitabine and radiation by Czito et al. in pancreatic and rectal cancer patients [15]. Capecitabine was doseescalated from 650 mg/m2 bid to 825 mg/m2 bid, but dose-limiting gastrointestinal toxicity became apparent even at the lower dose level. Four patients were unable to complete chemoradiation and two required prolonged breaks. There were no radiographic responses and no locally advanced patients were rendered resectable. Maurel et al. tested gefitinib with radiation and escalating doses of gemcitabine in a cohort of locally advanced patients, and reported moderate acute toxicity [16]. However, three patients died before they could be evaluated. Out of the 15 evaluable patients, there was a single partial response. No patients were able to undergo surgery, and the median survival was only 7.5 months. The Brown University group reported results of a combination of escalating doses of erlotinib with gemcitabine, paclitaxel and radiation followed by maintenance erlotinib in a mixed population of locally advanced and margin-positive patients [17]. The main toxicities were gastrointestinal and hematologic, and a maximum tolerated dose of 50 mg/day of erlotinib was defined. Notably, the partial response rate was 46% and the median survival for locally advanced patients was 14 months. Recently, Duffy et al. described promising results of a combination of escalating doses of erlotinib with radiation and bi-weekly gemcitabine followed by maintenance weekly gemcitabine and erlotinib [18]. Although only 55% completed all protocol therapy, and one patient died of gastrointestinal bleeding during maintenance therapy, 53% had stable disease, and 35% had partial responses, with one patient later undergoing an R0 resection. The median survival was 18.7 months. Preliminary results of several small series combining erlotinib with radiation and chemotherapy in the neoadjuvant and adjuvant settings are shown in Table 1 [19, 20, 21].
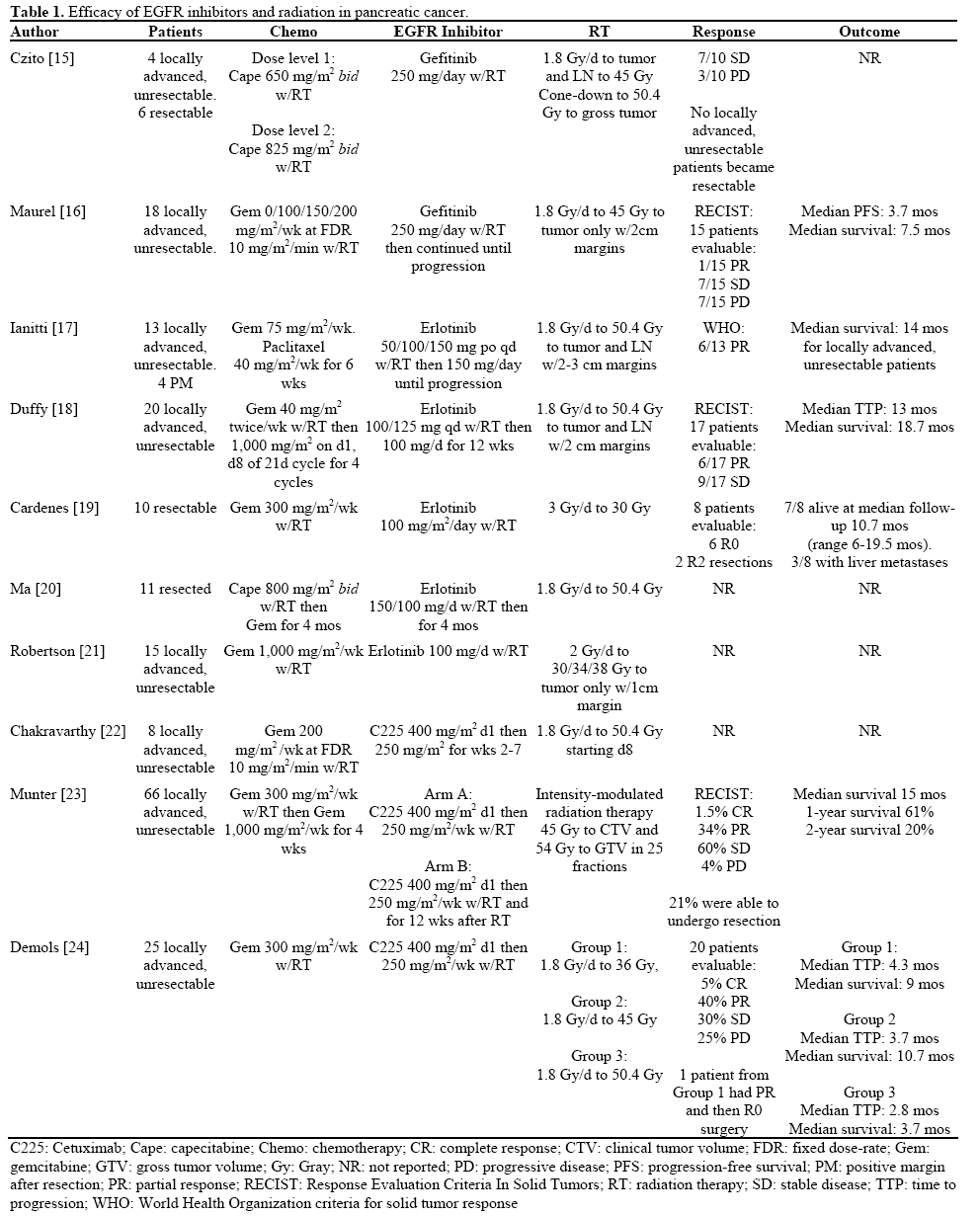
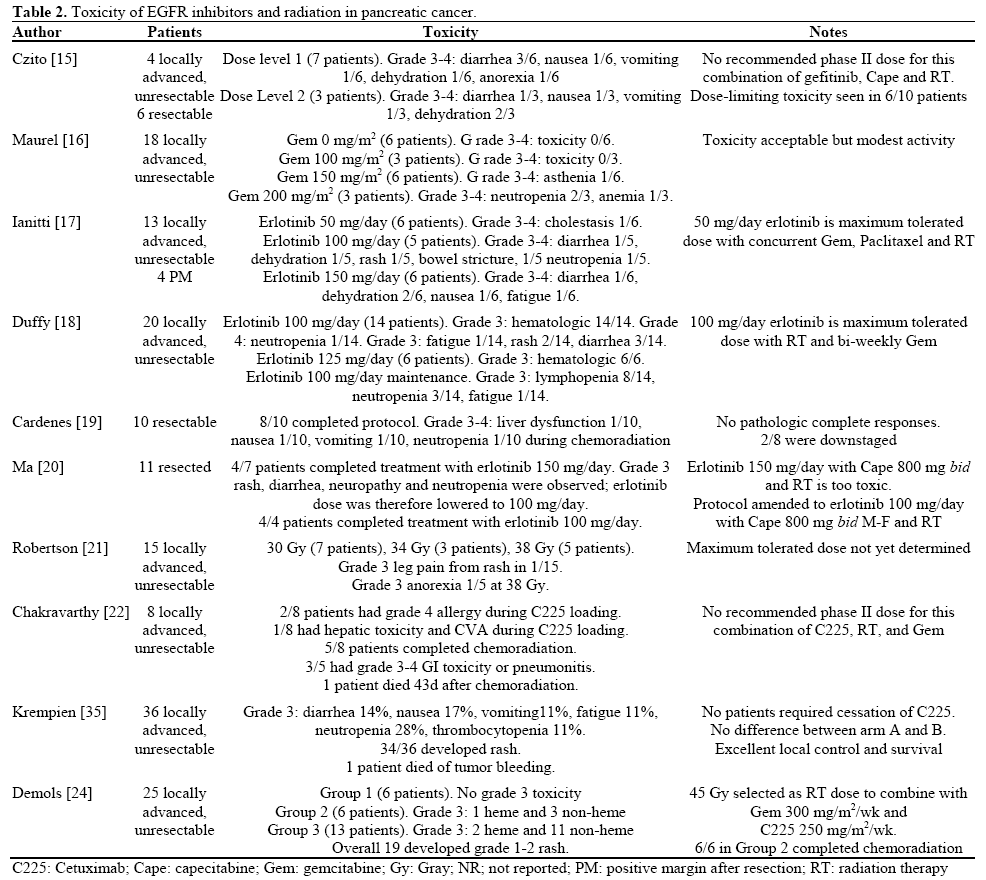
Early reports from several trials of the monoclonal antibody cetuximab in combination with radiation against pancreatic cancer have shown mixed results. Preliminary results of a phase I study conducted at Vanderbilt University have been published in abstract form. Weekly cetuximab and 50.4 Gy radiation were combined with weekly fixed dose-rate gemcitabine beginning at 200 mg/m2/week to treat 8 patients with locally advanced disease. Two patients had grade 4 allergic reactions and a third patient had liver toxicity and a stroke after the loading dose of cetuximab. The chemoradiation regimen was associated with substantial gastrointestinal toxicity, and one patient died of aspiration after completing the regimen [22]. In contrast, the University of Heidelberg has conducted a large phase II randomized study of gemcitabine, intensity-modulated radiation therapy and cetuxmab, followed by consolidation gemcitabine plus or minus cetuximab in locally advanced, unresectable patients. While no difference was seen between the two arms, the regimens had manageable toxicity. The rate of complete plus partial response was 35.5%, and the median survival for all patients was an encouraging 15 months. Twenty-one percent of patients were eventually able to undergo a potentially curative surgery [23]. Demols et al. treated 25 locally advanced patients with cetuximab, gemcitabine, and escalating radiation doses. One complete and 8 partial responses were seen, and one patient was able to undergo an R0 resection. A moderate dose of 45 Gy yielded the best survival and all 6 patients enrolled at this dose were able to complete treatment [24].
More Questions than Answers
Oncologists are right to be frustrated with the current state of affairs in pancreatic cancer. Articles reviewing progress made in pancreatic cancer typically begin by citing the incidence (37,680 cases expected in 2008 in the U.S. [25]), which continues to be nearly identical to the yearly death rate. The 11-month median survival for locally advanced pancreatic cancer patients in the E4201 trial [12], reported in 2008, is not markedly different from the 10-month median survival seen in the best arm of the Gastrointestinal Tumor Study Group (GITSG) trial from 1988 [13]. The success of erlotinib with gemcitabine in metastatic disease, however modest, marks the arrival of an additional therapeutic agent with proven activity against pancreatic cancer. The studies reviewed above represent the first tentative steps down a path that will hopefully lead us to new regimens with improved efficacy against pancreatic cancer.
What conclusions can be drawn so far from the published data? The heterogeneity of the data presented above makes it difficult to draw firm conclusions. The gefitinib trials used a fixed dose of gefitinib and escalating chemotherapy doses, while the larger erlotinib trials used fixed chemotherapy doses and escalating doses of erlotinib. Most patients were classified as having locally advanced disease, but the staging methods used were variable. Nonetheless, the published investigations of gefitinib with radiation and chemotherapy in locally advanced disease suggest little activity and the possibility for severe toxicity. In contrast, it seems that the combination of erlotinib, gemcitabine, and standard-dose and volume radiation is tolerable, with encouraging rates of response. The randomized cetuximab data reported by Munter et al. [23] demonstrated a high rate of response (35.5%) and intriguing resection data in a larger group of patients. Median survival was impressive at 15 months. Interestingly, the addition of consolidation cetuximab did not improve outcomes, although the trial was likely underpowered for this purpose. The Heidelberg group used intensity-modulated radiation therapy, which may have contributed to the tolerability of this regimen [26]. In contrast, Demols et al. found that the best survival rates were obtained with a moderate radiation dose of 45 Gy, whereas 50.4 Gy was more toxic and resulted in inferior survival [24].
Some would argue that, given the controversy surrounding the use of radiation in pancreatic cancer, efforts to add EGFR inhibition to radiation represent not a giant leap or even a small one, but a misstep. We would suggest that this is not the proper way to approach the issue. The theoretical benefits of radiosensitization and the clinical data published so far regarding radiation and EGFR inhibition in locally advanced pancreatic cancer offer sufficient promise to merit additional phase II investigation, at the least. In the pre-operative and adjuvant settings, more data and longer follow-up are needed to make an assessment. It is not clear which EGFR inhibitor should be combined with radiation. Cetuximab has the stronger clinical record as a radiosensitizer, and has approval specifically for this indication in head-and-neck cancer. Regarding the potential for controlling metastases, erlotinib has well-documented activity in advanced pancreatic cancer. A recent phase III randomized trial failed to show a statistically significant survival benefit to adding cetuximab to gemcitabine in advanced disease, although the absolute survival benefit (median survival of 6.4 versus 5.9 months) was similar to that seen in the NCIC trial with erlotinib [27]. In terms of tolerability, it is important to remember that even so called “targeted agents” can have significant systemic toxicity (particularly diarrhea), and that this is additive to the toxicity of “standard” chemotherapy and radiation. Maintenance or consolidation EGFR inhibition in conjunction with gemcitabine is an appealing concept, given the prevalence of metastatic disease, but unproven, and would also add to toxicity. The optimal radiation dose and volumes for locally advanced disease (tumor alone versus tumor and draining lymph nodes) remain additional unknown quantities. Finally, Lawrence et al. have published preclinical data suggesting that the sequencing of chemotherapy, EGFR inhibition and radiation may be clinically significant [28]. Given the number of factors in play, further phase I and II studies should be performed, and indeed a number are underway. Data from these studies should be studied carefully before moving into a cooperative group setting.
Efforts to define molecular markers that can select a cohort of pancreatic patients who will benefit from EGFR inhibition are ongoing. In the NCIC study, the intensity of immunohistochemical staining for EGFR did not predict response to erlotinib [10]. There is evidence to suggest that mutations in EGFR and increased EGFR gene copy number are related to tumor response to EGFR inhibition in certain tumor types. EGFR mutations appear to be rare in pancreatic cancer, and although increased EGFR copy number is relatively common finding, the implication of this finding with regard to EGFR inhibitor therapy has not yet been elucidated [29]. Researchers continue to evaluate other components of the EGFR signaling pathway, such as activated EFGR, in the search for a marker that will predict the response of pancreatic tumors to EGFR inhibition [30]. There is strong data to indicate that mutation of the K-ras gene, a downstream signaling intermediary of the EGFR family, predicts for a lack of response to cetuximab in colorectal cancer [31]. Likewise, non-small cell lung cancer patients with mutated K-ras do not respond to EGFR inhibition by TKIs [32]. A subset analysis of available samples from the NCIC trial showed that 76% had mutated K-ras, and there was a nonsignificant trend towards response to erlotinib in patients with wild-type K-ras [33]. While up to 90% of pancreatic tumors have K-ras mutations [34], the high response rates seen in Table 1 suggest that the biology of pancreatic cancer may be different with regard to the interaction of K-ras and EGFR. Alternatively, the mechanisms through which the combination of radiation, chemotherapy and EGFR inhibitors attack tumors may be different from those involved when chemotherapy and EGFR inhibitors are combined. Only 181 of the 569 patients enrolled on the NCIC trial had adequate tissue for retrospective molecular analysis [33]. Future studies should make every effort to incorporate prospective tissue banking and consider repeat biopsies to evaluate molecular responses during treatment to improve our understanding of the biology of EFGR inhibition in the setting of chemoradiation. Ultimately, improved patient selection through the use of biomarkers could greatly increase the chances for success of future phase III efforts.
Conclusions
The combination of EGFR inhibition with concurrent chemoradiation in locally advanced pancreatic cancer has shown promising tumor response rates in the range of 30-40% with acceptable toxicity and median survival times in excess of 14 months. Further prospective studies are needed to determine the optimal combination and schedule of EGFR inhibitor, chemotherapy, and radiation and to validate molecular markers that can identify a set of patients who are most likely to respond.
Conflict of interest
The authors have no potential conflicts of interest
References
- Baselga J. Why the epidermal growth factor receptor? The rationale for cancer therapy. Oncologist 2002; 7 Supp 4:2-8. [PMID 12202782]
- Tsiambas E, Karameris A, Lazaris AC, Talieri M, Triantafillidis JK, Cheracakis P, et al. EGFR alterations in pancreatic ductal adenocarcinoma: a chromogenic in situ hybridization analysis based on tissue microarrays. Hepatogastroenterology 2006; 53:452-7. [PMID 16795991]
- Ueda S, Ogata S, Tsuda H, Kawarabayashi N, Kimura M, Sugiura Y, et al. The correlation between cytoplasmic overexpression of epidermal growth factor receptor and tumor aggressiveness: poor prognosis in patients with pancreatic ductal adenocarcinoma. Pancreas 2004; 29:e1-8. [PMID 15211117]
- Huang SM, Harari PM. Modulation of radiation response after epidermal growth factor receptor blockade in squamous cell carcinomas: inhibition of damage repair, cell cycle kinetics, and tumor angiogenesis. Clin Cancer Res 2000; 6:2166-74. [PMID 10873065]
- Ciardiello F, Caputo R, Troiani T, Borriello G, Kandimalla ER, Agrawal S, et al. Antisense oligonucleotides targeting the epidermal growth factor receptor inhibit proliferation, induce apoptosis, and cooperate with cytotoxic drugs in human cancer cell lines. Int J Cancer 2001; 93:172-8. [PMID 11410862]
- Baumann M, Krause M, Dikomey E, Dittmann K, Dörr W, Kasten-Pisula U, Rodemann HP. EGFR-targeted anti-cancer drugs in radiotherapy: preclinical evaluation of mechanisms. RadiotherOncol 2007; 83:238-48. [PMID 17502118]
- Buchsbaum DJ, Bonner JA, Grizzle WE, Stackhouse MA, Carpenter M, Hicklin DJ, et al. Treatment of pancreatic cancer xenografts with Erbitux (IMC-C225) anti-EGFR antibody, gemcitabine, and radiation. Int J RadiatOncolBiolPhys 2002; 54:1180-93. [PMID 12419447]
- Morgan MA, Parsels LA, Kollar LE, Normolle DP, Maybaum J, Lawrence TS. The combination of epidermal growth factor receptor inhibitors with gemcitabine and radiation in pancreatic cancer. Clin Cancer Res 2008; 14:5142-9. [PMID 18698032]
- Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, et al. Radiotherapy plus cetuximab for squamous-cell carcinoma of the head and neck. N Engl J Med 2006; 354:367-78. [PMID 16467544]
- Moore MJ, Goldstein D, Hamm J, Figer A, Hecht JR, Gallinger S, et al. Erlotinib plus gemcitabine compared with gemcitabine alone in patients with advanced pancreatic cancer: a phase III trial of the National Cancer Institute of Canada Clinical Trials Group. J ClinOncol 2007; 25:1960-6. [PMID 17452677]
- Kalser MH, Ellenberg SS. Pancreatic cancer. Adjuvant combined radiation and chemotherapy following curative resection. Arch Surg 1985; 120:899-903. [PMID 4015380]
- Loehrer PJ, Powell ME, Cardenes HR, Wagner L, Brell JM, Ramanathan RK, et al. A randomized phase III study of gemcitabine in combination with radiation therapy versus gemcitabine alone in patients with localized, unresectable pancreatic cancer: E4201. J ClinOncol 2008; 26(15S):4506. ASCO Annual Meeting.
- Treatment of locally unresectable carcinoma of the pancreas: comparison of combined-modality therapy (chemotherapy plus radiotherapy) to chemotherapy alone. Gastrointestinal Tumor Study Group. J Natl Cancer Inst1988; 80:751-5. [PMID 2898536]
- Murphy JD, Adusumilli S, Griffith KA, Ray ME, Zalupski MM, Lawrence TS, Ben-Josef E. Full-dose gemcitabine and concurrent radiotherapy for unresectable pancreatic cancer. Int J RadiatOncolBiolPhys 2007; 68(3):801-8. [PMID 17379445]
- Czito BG, Willett CG, Bendell JC, Morse MA, Tyler DS, Fernando NH, et al. Increased toxicity with gefitinib, capecitabine, and radiation therapy in pancreatic and rectal cancer: phase I trial results. J ClinOncol 2006; 24:656-62. [PMID 16446337]
- Maurel J, Martin-Richard M, Conill C, Sánchez M, Petriz L, Ginès A, et al. Phase I trial of gefitinib with concurrent radiotherapy and fixed 2-h gemcitabine infusion, in locally advanced pancreatic cancer. Int J RadiatOncolBiolPhys 2006; 66:1391-8. [PMID 16965868]
- Iannitti D, Dipetrillo T, Akerman P, Barnett JM, Maia-Acuna C, Cruff D, et al. Erlotinib and chemoradiation followed by maintenance erlotinib for locally advanced pancreatic cancer: a phase I study. Am J ClinOncol 2005; 28(6):570-5. [PMID 16317266]
- Duffy A, Kortmansky J, Schwartz GK, Capanu M, Puleio S, Minsky B, et al. A phase I study of erlotinib in combination with gemcitabine and radiation in locally advanced, non-operable pancreatic adenocarcinoma. Ann Oncol 2008; 19:86-91. [PMID 17878176]
- Cardenes HR, Chiorean EG, Perkins S, DeWitt J, Schmidt CM, Crowell P, et al. Neoadjuvant gemcitabine, erlotinib and hypofractionated radiation therapy for potentially resectable pancreatic cancer: A pilot study. J ClinOncol 2008; 26(15S):15578. ASCO Annual Meeting.
- Ma W, Herman JM, Laheru D, Messersmith WA, Jimeno A, Rudek M, et al. A phase I tolerability and pharmacokinetic study of adjuvant erlotinib (E) and capecitabine (Cap) with concurrent radiation (RT) in resected pancreatic cancer (PanCa) patients. 2008 ASCO Gastrointestinal Cancers Symposium (Abstract #217).
- Robertson JM, Hardy MM, Ballouz S, Jaiyesimi I, Margolis J, Jury R, et al. Conformal radiation therapy with concurrent full-dose gemcitabine and erlotinib for unresected pancreas cancer: a phase I trial. Int J RadiatOncolBiolPhys 2008; 72(1) Suppl1:S275.
- Charkravarthy AB, Berlin JD, Lockhart AC, Chana E, Parikha A, Kordowskia V, et al. A phase I study of cetuximab in combination with gemcitabine and radiation for locally advanced pancreatic cancer. Int J RadiatOncolBiolPhys 2008; 72(1) Suppl1:S250-S251.
- Munter M, Timke C, Abdollahi A, Friess H, Jaeger D, Heeger S, et al. Final results of a phase II trial [PARC-Study ISRCTN56652283] for patients with primary inoperable locally advanced pancreatic cancer combining intensity-modulated radiotherapy (IMRT) with cetuximab and gemcitabine. J ClinOncol 2008; 26(15S):4613. ASCO Annual Meeting.
- Demols A, Mahin C, Marechal R, Delaunoit T, Borbath I, Hendlisz A, et al. Cetuximab plus chemoradiation combined therapy for locally advanced inoperable pancreatic adenocarcinoma: a phase I study. J ClinOncol 2008; 26(15S);4629. ASCO Annual Meeting.
- American Cancer Society. Cancer Facts and Figures, 2008. Atlanta, GA, USA: American Cancer Society, 2008.
- Krempien R, Muenter MW, Huber PE, Nill S, Friess H, Timke C, et al. Randomized phase II--study evaluating EGFR targeting therapy with cetuximab in combination with radiotherapy and chemotherapy for patients with locally advanced pancreatic cancer-- PARC: study protocol (ISRCTN56652283). BMC Cancer 2005; 5:131-42. [PMID 16219105]
- Philips PA, Benedetti J, Fenoglio-Preiser C, Zalupski M, Lenz H, O'Reilly E, et al. Phase III study of gemcitabine [G] plus cetuximab [C] versus gemcitabine in patients [pts] with locally advanced or metastatic pancreatic adenocarcinoma [PC]: SWOG S0205 study. J ClinOncol 2007; 25(18S):4509. ASCO Annual Meeting.
- Nyati MK, Morgan MA, Feng FY, Lawrence TS. Integration of EGFR inhibitors with radiochemotherapy. Nat Rev Cancer 2006; 6:876-85. [PMID 17036041]
- Lee J, Jang KT, Ki CS, Lim T, Park YS, Lim HY, et al. Impact of epidermal growth factor receptor (EGFR) kinase mutations, EGFR gene amplifications, and KRAS mutations on survival of pancreatic adenocarcinoma. Cancer 2007; 109:1561-9. [PMID 17354229]
- Harsha HC, Jimeno A, Molina H, Mihalas AB, Goggins MG, Hruban RH, et al. Activated epidermal growth factor receptor as a novel target in pancreatic cancer therapy. J Proteome Res 2008; 7:4651-8. [PMID 18821783]
- Van Cutsem E, Landg I, D'haens G, Moiseyenko V, Zaluski J, Folprecht G, et al. KRAS status and efficacy in the first-line treatment of patients with metastatic colorectal cancer (mCRC) treated with FOLFIRI with or without cetuximab: The CRYSTAL experience. J ClinOncol 2008; 26(15S):2. ASCO Annual Meeting.
- Eberhard DA, Johnson BE, Amler LC, Goddard AD, Heldens SL, Herbst RS, et al. Mutations in the epidermal growth factor receptor and in KRAS are predictive and prognostic indicators in patients with non-small-cell lung cancer treated with chemotherapy alone and in combination with erlotinib. J ClinOncol 2005; 23:5900- 9. [PMID 16043828]
- Moore MJ, da Cunha Santos G, Kamel-Reid S, Chin K, Tu D, Parulekar W, et al. The relationship of K-ras mutations and EGFR copy number with Erlotinib on National Cancer Institute of Canada Trial PA.3. J ClinOncol 2007; 25(18S):4521. ASCO Annual Meeting.
- Almoguera C, Shibata D, Forrester K, Martin J, Arnheim N, Perucho M. Most human carcinomas of the exocrine pancreas contain mutant c-K-ras genes. Cell 1988; 53:549-54. [PMID 2453289]
- Krempien R, Munter MW, Timke C, Freiss H, Hartung G, Herfarth KK, et al. Cetuximab in combination with intensity modulated radiotherapy (IMRT) and gemcitabine for patients with locally advanced pancreatic cancer: A prospective phase II trial PARC-Study ISRCTN56652283). J ClinOncol 2007; 25(18S):4573. ASCO Annual Meeting.

