Jiun Miin Lai1, Peter Crowley2, Mehrdad Nikfarjam1*
Department of Surgery
Department of Anatomic Pathology, University of Melbourne, Austin Health. Melbourne, Victoria, Australia
- *Corresponding Author:
- Mehrdad Nikfarjam
University Department of Surgery
Austin Health, LTB 8; Studley Rd, Heidleberg
Melbourne, Victoria 3084; Australia
Phone: +613-9496.5466
Fax: +613-9458.1650
E-mail: mehrdad.nikfarjam@gmail.com
Received January 14th, 2011 Accepted January 31st, 2011
Keywords
Lymphatic Metastasis; Lymphoma; Pancreatic Neoplasms; Pancreaticoduodenectomy
INTRODUCTION
Less than 20% of pancreatic cancers at diagnosis are resectable at the time of presentation and nearly all patients die of their disease [1]. Locally advanced disease and metastases to other viscera are the most common reasons for precluding surgical resection [2]. Lymph node involvement in particular is associated with a poor prognosis [3]. Even following complete resection, the majority of patients with pancreatic cancer develop recurrent disease. The risk of recurrence is highest in those with lymph node involvement.
Given the particularly poor prognosis of lymph node metastases when associated with pancreatic cancer, some centres may consider peri-pancreatic and intraabdominal lymphadenopathy as a marker of metastatic, incurable disease. We report two patients with peripancreatic lymphadenopathy who were found to have concurrent lymphoma, without evidence of pancreatic lymph node metastases. The finding of concurrent lymphoma and pancreatic cancer is discussed and patterns of lymph node enlargement that may help differentiate pancreatic lymph node metastases from other causes of lymphadenopathy are noted.
CASE REPORTS
The details of two patients with concurrent lymphoma and pancreatic adenocarcinoma are summarized in Table 1.
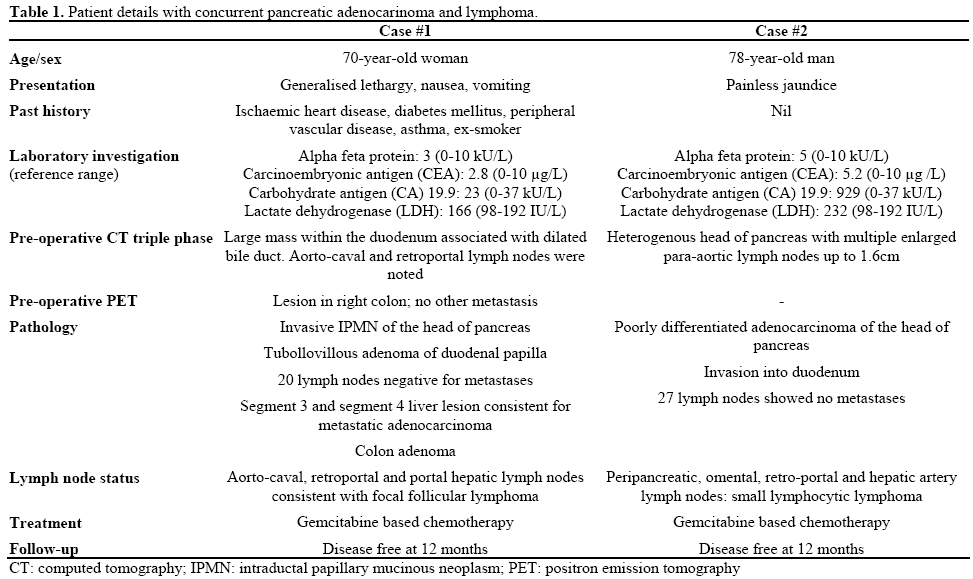
Case #1
A 70-year-old lady with several months of general lethargy, intermittent nausea and vomiting had abdominal computed tomography (CT) showing a large mass within the duodenum and associated bile duct dilatation. Pre-operative tumour markers were unremarkable. Endoscopy showed a large tumour arising from the ampulla causing partial obstruction of the duodenum. Aorto-caval and retro-portal lymphadenopathy was noted on imaging (Figure 1ab). Positron emission tomography (PET) scan showed no obvious metastatic disease but a lesion in the right colon. At the time of surgery a large ampullary mass causing partial gastric outlet obstruction was noted as well as a mass in the caecum. A few indiscrete lesions were removed from the liver that on frozen section were not typical of malignancy. A classic pancreaticoduodenectomy with retroperitoneal lymph node dissection and right hemicolectomy was performed. Final pathology showed concurrent ampullary tubulovillous adenoma and pancreatic invasive intra-papillary mucinous neoplasia (IPMN) (Figure 1c) and a dysplastic colonic adenoma. There was no evidence of lymph node metastases, although several enlarged nodes were noted to contain grade 2 follicular lymphoma (Figure 1d). One of the liver lesions on permanent sections was consistent with metastatic pancreatic adenocarcinoma. Post-operative lactate dehydrogenase level (LDH) was normal. The patient had post-operative gemcitabine based chemotherapy and is tumour free on CT imaging 12 months following surgery. No treatment was given for the lymphoma due to the patient’s lack of symptoms.
Figure 1. a. Aorto-caval lymph node enlargement clear noted (arrow). Biliary dilatation by an ampullary mass is also observed. b. Cross sectional
images further demonstrate enlarged aorto-caval lymph nodes (arrow). c. Focus of invasive ductal adenocarcinoma associated with intraductal
papillary mucinous neoplasm (H&E x400) d. Lymph node, follicular lymphoma. Immunohistochemical stain for CD20 showing back to back
follicles composed of CD20 positive B-cells (x40).
Case #2
A 78-year-old man was investigated for painless jaundice and found to have a pancreatic mass. Preoperative tumour markers were normal. LDH level was slightly elevated at 232 (reference range: 98-192 IU/L). Multiple enlarged para-aortic lymph nodes were also noted (Figure 2ab). The patient underwent an uncomplicated classic pancreaticoduodenectomy and lymph node dissection. A 3 cm pancreatic ductal adenocarcinoma was removed without evidence of lymph-node metastases (Figure 2c). The lymph nodes however contained small lymphocytic lymphoma (Figure 2d). The patient received post-operative gemcitabine based chemotherapy for pancreatic cancer. The lymphoma had not been treated at the time of last review, due to the stable nature of the disease on CT imaging and lack of symptoms. He is alive and well without obvious pancreatic cancer recurrence at 12 months follow-up.
Figure 2. a. Computed tomography identifying para-aortic lymphadenopathy, with one enlarged node clearly highlighted (arrow). b. Cross sectional
images further demonstrate this finding (arrow). c. Poorly differentiated duct adenocarcinoma of the pancreas (H&E x100). d. Lymph node, small
lymphocytic lymphoma (H&E x200).
DISCUSSION
Pancreatic cancer has an extremely poor prognosis with the only chance of cure being surgical resection [2]. Patients with pancreatic cancer and lymph node metastases have a particularly poor prognosis. An understanding of lymph node patterns of spread and causes for abdominal lymphadenopathy is important if we are to ensure that patients with resectable pancreatic cancer are not denied surgery by incorrect interpretation of intra-abdominal lymphadenopathy.
The word peri-pancreatic lymph node enlargement is used loosely without precise understanding of the specific pancreatic lymph nodes anatomy. It should be noted that the upper abdomen lymphatic channels generally follow the arterial supply and this holds true with the pancreas. Pancreatic head and uncinate process lymphatic drainage is complex. The more anterior rostral area drains along the gastroduodenal artery to the hepatoduodenal ligament as well as in the duodenopancreatic groove via the pancreaticoduodenal arcade. The lymphatics of the uncinate process and more inferior aspect of the pancreatic head drain via the inferior pancreaticoduodenal artery to the superior mesenteric nodal basin. They have numerous anastomoses and may drain into either the lymph nodes near the root of the celiac axis or superior mesenteric artery. Of importance, pancreatic cancer lymph node drainage usually terminates above the level of the left renal vein.
When one examines the patterns of lymph node spread in pancreatic cancer and lymphoma there are various differences. Costello et al. examined four patterns of distribution of lymph node enlargement in lymphoma and pancreatic cancer [4]. Four types of peri-pancreatic lymphadenopathy are described in for lymphoma. Type 1 is located in the pre-aortic retropancreatic region. Type 2 is pancreatiocosplenic lymphadenopathy. Type 3 is isolated celiac and/or portal lymphadenopathy. Type 4 includes diffuse, extensive lymphadenopathy. Data collected from staging laparotomies in those previously untreated lymphoma indicate that paraaortic lymph nodes involvement in lymphoma can be as high as 68% in non-Hodgkin’s lymphoma, 71% in mesenteric nodes, and 61% in splenic disease [5]. High quality CT has accuracy at detecting intra-abdominal disease in lymphoma in 90% of cases [6].
In studies of lymph node patterns in pancreatic cancer,13 out of 40 had peripancreatic lymph nodes enlargement [4]. The distribution of lymph nodes being retropancreatic (9 out of 13), celiac (2 out of 13), pancreaticosplenic (1 out of 13) and portal (1 out of 13). Although the patterns of lymph node spread in pancreatic cancer can be along the same patterns as in lymphoma there are some general differences that should be considered. Diffuse intra-abdominal lymphadenopathy is not commonly associated with pancreatic cancer. In addition, lymph node metastases from pancreatic cancer generally occur above the level of the renal vein. Para-aotic and para-caval lymph node enlargement below this level should raise suspicions of an alternate cause of retroperitoneal lymphadenopathy.
In terms of concurrent pancreatic cancer and lymphoma, we could not identify any reported case in literature. Whether many such patients are not offered surgery due to lymph node enlargement based on imaging reports is unknown. Although no concurrent lymphoma and pancreatic cancer metastasis within the same node has been previously reported, these have been noted with other tumours. A case of metachronous lymphoma and early gastric cancer within the same node has been reported [7]. There is also a report of involvement of same lymph node by lymphoma and metastatic adenocarcinoma from primary colon cancer [8].
In the two cases presented, enlarged lymph nodes were noted, which may have been considered incurable disease. Neither patient had instrumentation of the biliary tree as an explanation for lymph node enlargement or exhibited evidence of current or past biliary sepsis. One patient had enlarged aorto-caval lymph nodes located below the renal vein. The other had para-aortic lymphadenopathy, once again mainly below the level of the renal veins. The pattern of lymph node enlargement was more in keeping with lymphoma than metastatic pancreatic cancer, as was confirmed on final pathology.
Both patients had advanced disease, with one confirmed to have liver metastases on final pathology and the other a locally advanced primary cancer. Of interest, none had pancreatic cancer metastases to the lymph nodes. Whether lymphoma in the peripancreatic lymph nodes alters the spread of pancreatic cancer to the nodes is unknown. Changes to the lymph nodes structure and microenvironment caused by lymphoma may prevent implantation and growth of pancreatic cancer in the nodes or lymphoma may simply obliterate any lymph node deposits of pancreatic cancer. Clearly this is only speculative.
CONCLUSION
Concurrent lymphoma and pancreatic cancer is a rare phenomenon but may be a cause of intra-abdominal lymph node enlargement in some patients. This has however not been reported previously. CT scanning is useful tool in assessing bulky lymph nodes in patients with intra-abdominal cancer. Interpretation of enlarged lymph nodes in patients with pancreatic cancer is important and has to be done precisely with clear understanding of lymphatic drainage. Not all cases represent metastases, even in patients with no history of intra-abdominal inflammation or biliary manipulation. This should not be used as a major determinant of incurable disease in patients with pancreatic cancer.
Conflicts of interest
The authors have no potential conflicts of interest
References
- Garcea G, Dennison AR, Pattenden CJ, Neal CP, Sutton CD, Berry DP. Survival following curative resection for pancreatic ductal adenocarcinoma. A systematic review of the literature. JOP J Pancreas (Online) 2008; 9:99-132.
- SimianuVV, Zyromski NJ, Nakeeb A, Lillemoe KD. Pancreatic cancer: progress made. Acta Oncol 2010; 49:407-17. [PMID 20059311]
- Konstantinidis IT, Deshpande V, Zheng H, et al. Does the mechanism of lymph node invasion affect survival in patients with pancreatic ductal adenocarcinoma? J Gastrointest Surg 2009; 14:261- 7. 4.
- Costello P, Duszlak EJJr, Kane RA, Lee RG, Clouse ME. Peripancreatic lymph node enlargement in Hodgkin's disease, non- Hodgkin's lymphoma, and pancreatic carcinoma. J Comput Tomogr 1984; 8:1-11. [PMID 6362986]
- Earl HM, Sutcliffe SB, Fry IK, Tucker AK, Young J, Husband J, et al. Computerised tomographic (CT) abdominal scanning in Hodgkin's disease. Clin Radiol 1980; 31:149-53. [PMID 7363543]
- Williams RG, Koehler PR. Normal anatomy and limitations in CT interpretation of lymph node disease. J Comput Tomogr 1979; 3:190-6. [PMID 262216]
- Durnali AG, Tokluoglu S, Alkis N, Ulas A, Turkoz FP. Primary gastric Hodgkin lymphoma and metachronous early gastric carcinoma: a case report. Med Oncol 2010 Oct 22.
- Bhanote M, Choksi M, Cassar P, Edelman M, DellaRatta R, Staszewski H. Metastatic adenocarcinoma of the colon and follicular lymphoma within the same lymph node: a case report and review of the literature. Int J Gastrointest Cancer 2005; 36:171-5. [PMID 16720913]



