Keywords
capecitabine; Chemotherapy, Adjuvant; erlotinib; Fluorouracil; gemcitabine; oxaliplatin; Pancreatic Neoplasms; Radiotherapy
Abbreviations
CONKO: Charité Onkologie; EORTC: European Organization of Research and Treatment of Cancer; ESPAC: European Study Group for Pancreatic Cancer; GITSG: Gastrointestinal Tumor Study Group; GMCSF: granulocyte/macrophage-colony-stimulating factor; NCCN: National Comprehensive Cancer Network; RTOG: Radiation Therapy Oncology Group
INTRODUCTION
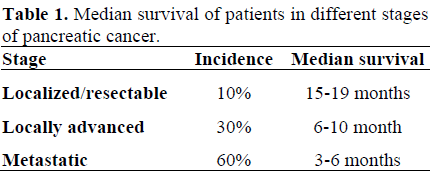
Pancreatic cancer is the fourth most common malignancy in the United States. The annual incidence rate is almost identical to the mortality rate with an estimated incidence of 37,170 new cases diagnosed and 33,370 deaths due to pancreatic cancer in 2007 [1]. Five-year survival rate remains less than 5% [1]. Poor prognosis had been attributed to inability to diagnose while tumor is resectable and its propensity towards early vascular dissemination and spread to regional lymph nodes. About 10%-20% of patients have resectable disease at the time of pancreatic cancer diagnosis; the curative resection rate is only 14% and median survival of 15-19 months [2]. The 5-year survival rate following resection is 25-30% for node-negative disease and 10% for node-positive cancers [3]. Local recurrence is usually attributed to the difficulty of achieving microscopically disease-free surgical margins, particularly at the retroperitoneal margin. These outcomes are improving, likely related to an increased proportion of patients undergoing operations at high-volume centers and the increased use of adjuvant therapies [4]. The high risk of local and systemic disease recurrence as well as overall poor prognosis laid down the rationale for adjuvant therapy after resection of pancreatic adenocarcinoma (Table 1). There is no consensus on what constitutes 'standard' adjuvant therapy. This controversy derives from several studies, each fraught with its own limitations. Standards of care also vary depending on which side of the Atlantic you are on: chemo-radiotherapy followed by chemotherapy is considered the optimal therapy in North America (Gastrointestinal Tumor Study Group: GITSG; Radiation Therapy Oncology Group: RTOG) while chemotherapy alone is the current standard in Europe (European Study Group for Pancreatic Cancer: ESPAC-1; Charité Onkologie: CONKO).
Chemo-Radiotherapy
The GITSG trial was the first prospective randomized trial suggesting survival advantage with postoperative chemo-radiotherapy using bolus 5-FU (median survival: 20 months vs. 11 months and 5-year survival: 18% vs. 8%) [5]. However this study was criticized for poor patient accrual, early termination, and small patient numbers, and some maintained that the radiotherapy dose was suboptimal (some authors advocate 50 Gy as a total effective dose)
Multiple authors have attempted to confirm its findings. The European Organization of Research and Treatment of Cancer (EORTC) compared 5-FU (25 mg/kg/day continuous infusion for 5 days every 4 weeks) with concurrent radiotherapy using a split course (40 Gy) with observation only in patients with resected pancreatic and periampullary cancer [6]. Klinkenbijl et al. were able to show a trend toward benefit in terms of median survival (24.5 months vs. 19.0 months; P=0.208) [6]. The subgroup analysis looking only at pancreatic cancer patients showed a trend toward benefit in median survival (17.1 months vs. 12.6 months; P=0.099) [6]. This study too was criticized for suboptimal dose of radiotherapy and split courses. Lower radiotherapy dose and split courses that may have allowed cancer repopulation between courses thereby under-estimating the benefit of chemo-radiotherapy (Figure 1).
Figure 1. EORTC: adjuvant chemo-radiotherapy.
Although not conclusive, these results showed a trend toward benefit of adjuvant therapy and led to the ESPAC-1 trial, the largest reported randomized study to date investigating the role of combination chemo-radiotherapy in pancreatic cancer [7]. This study, in fact, has sparked a new debate over the role of radiotherapy in the adjuvant therapy of pancreatic cancer. ESPAC-1 trial was 2x2 factorial designed study comparing adjuvant concurrent chemo-radiotherapy (bolus 5- FU/split course radiotherapy), chemotherapy alone (5-FU/leucovorin), chemo-radiotherapy followed by chemotherapy, and observation. Chemotherapy only arm had statistically significant benefit over observation arm in median survival (20.1 months vs. 15.5 months; P=0.009). However, chemoradiotherapy arm showed worse median survival compared with patients who did not receive chemo-radiotherapy (15.9 months vs. 17.9 months; P=0.05) [6]. Interpretation of this study is complicated slightly because two different study designs are used: a 2x2 factorial design and direct head-to-head comparisons (chemotherapy vs. no chemotherapy and chemo-radiotherapy vs. no chemo-radiotherapy). Eligible patients were pre-enrolled in one of the above strategies. The authors then reported their findings for each of the separate study designs as well as for the pooled data. Therefore, major criticism was made on this study for possible selection bias as both patients and clinicians were allowed to select which trial to enter, a concern of suboptimal radiotherapy, and for allowing the final radiotherapy dose to be left to the judgment of the treating physicians. Moreover, the treatment for patients in the chemo-radiotherapy group did not include post-radiotherapy adjuvant chemotherapy, making direct comparison to the GITSG trial difficult (Figure 2).
Figure 2. ESPAC-1: trial design.
The ESPAC-1 study uses only a 5-FU-based chemotherapy regimen; and certainly, a gemcitabine-based approach is the most logical place to start, which was recently evaluated in the RTOG 9704 study. RTOG 9704 study randomized 538 resected pancreatic cancer patients to evaluate benefit of adding gemcitabine to infusional 5-FU combined with radiotherapy [8]. One arm received 5-FU plus radiotherapy and the other arm was treated with gemcitabine before and after 5-FU plus radiotherapy. Patients with pancreatic head tumors (No. 380) showed benefit in median survival (18.8 months vs. 16.7 months; P=0.047) by the incorporation of gemcitabine before and after 5-FU plus radiotherapy. However, there was no significant difference when pancreatic body and tail cancers were all included (Figure 3).
Figure 3. RTOG 9704: post operative 5-fluorouracil
vs. gemcitabine as pre- and post-chemo-radiotherapy
for pancreatic cancer.
Chemotherapy Alone
While benefit of radiation therapy was inconclusive in randomized trials, Oettle et al. published the results of CONKO-001 study in JAMA this year [9]. CONKO-001 study randomized 368 patients with resected pancreatic cancer to gemcitabine or observation for 6 months. Tumor prognostic characteristics were similar in both arms. This trial showed statistically significant disease free survival benefit (13.4 months vs. 6.9 months; P<0.001) of gemcitabine over observation. Gemcitabine rendered a trend toward overall benefit (22.1 months vs. 20.2 months; P=0.06). This benefit of chemotherapy was consistent with the result from ESPAC-1 trial which showed benefit of 5-FU/leucovorin over no adjuvant therapy in pancreatic cancer patients (median survival of 19.7 months vs. 14.0 months) who had complete resection [7] (Figure 4). The CONKO-001 study has many worth mentioning points. Gemcitabine, the current standard of care in first line treatment, has clearly showed superiority over 5-FU in patients with advanced pancreatic cancer, both in terms of dramatic improvement in clinical benefit response as well as a modest improvement in median survival [10]. Therefore, ESPAC-1 (in which 5-FU was the chemotherapy agent of choice) and the Burris et al. study both provide a rationale for choosing gemcitabine arm in CONKO-001 study [7, 10]. CONKO-001 study also reconfirmed that single-agent chemotherapy with gemcitabine was generally well-tolerated in this study and most of the patients were able to complete the full six cycles of treatment [9]. On the other hand, the median disease free survival of patients in the observation-only was dismal (less than 7 months), underlying the fact in addition to further improve the adjuvant treatment regimens, specialized surgeries such as Whipple’s procedure should preferentially be carried out at high volume centers by experienced surgeons, where outcomes are known to be better [4].
Figure 4. CONKO-001: trial design.
Alternate Adjuvant Therapies
Interferon-alpha
Alternate adjuvant therapies have also been investigated. Picozzi et al. performed a phase II trial of an interferon-based chemotherapy regimen with concomitant post-operative adjuvant radiotherapy [11]. Forty-three patients received radiotherapy at a dose of 4,500 to 5,400 cGy (25 fractions over 5 weeks) and three-drug chemotherapy: continuous infusion 5-FU (200 mg/m2 daily, days 1 to 35), weekly intravenous bolus cisplatin (30 mg/m2 daily, days 1, 8, 15, 22, 29), and subcutaneous alpha, interferon (3x106 units, days 1 to 35). This chemoradiotherapy was followed by continuous infusion 5-FU (200 mg/m2 daily, weeks 9 to 14 and 17 to 22). Chemo-radiotherapy was generally initiated between 6 and 8 weeks after surgery. At a mean follow-up of 31.9 months, 67% of patients were still alive. The actuarial overall 1-, 2-, and 5-year survival rates were 95%, 64%, and 55%, respectively. Although the potential survival benefit with this regimen seems promising, but about 70% of the patients developed moderate to severe gastrointestinal toxicity. The confirmatory studies are under way.
Vaccines
The development of pancreatic cancer vaccines has been the subject of recent developments in the adjuvant treatment of pancreatic cancer [12]. Jaffee et al. developed an irradiated granulocyte/macrophage-colonystimulating factor (GM-CSF) transfected allogeneic whole cell line pancreas adenocarcinoma immunotherapy and previously reported the results of the first phase I trial establishing the safety of the GM-CSF-secreting tumor in patients with resected pancreatic cancer [13]. Most recently, their group presented the results of a phase II study of 60 patients with resected pancreatic adenocarcinoma administered a total of five immunotherapy treatments using two pancreatic cancer cell lines each delivering 2.5x108 cells intradermal [14]. Immunotherapy treatment one was administered 8 to 10 weeks following surgical resection. Patients subsequently were treated with 5-FU continous intravenous infusion with concurrent radiotherapy. Patients who were disease-free one month after completion of chemo-radiotherapy received immunotherapy treatment 2-4, each one month apart. A fifth and final booster immunotherapy treatment was administered 6 months after vaccine 4. One- and 2-year survivals are 88% and 76% respectively. The pancreas cancer vaccine was well tolerated. Treatment related side effects included transient vaccine injection site reactions. While the data is only preliminary, this study compares very favorably with the available published data.
Pancreatic Cancer Stem Cells
The cancer stem cell hypothesis suggests that neoplastic clones are maintained exclusively by a small subset of cells with stem cell properties within a tumor [15]. There has been strong evidence to support this theory in blood, brain, and breast cancers. Pilot studies are currently under way to study pancreatic cancer stem cells. The information gained may lead to new avenues to identify novel tumor cell markers for diagnostic purposes and to identify new cellular targets and will provide a cell population that can be used for testing new chemotherapeutic agents, biological modifiers, and immune-based therapies.
Discussion
Pancreatic cancer remains a dismal disease with poor prognosis, even after curative resection and most aggressive combinemodality approaches. This serves as a sobering reminder that we need to push the envelope even further so that in the future, for patients who undergo resection of pancreatic cancer with “curative intent”, the curative intent is fulfilled more frequently than not. The varying results of these randomized trials make it difficult to establish a standard of adjuvant therapy for resected pancreatic adenocarcinoma. The absolute value of radiotherapy in this setting remains to be defined. The question is whether we should change our practice with regard to how we treat patients whose pancreatic cancer was resected based on ESPAC-1 study [7]. The answer is no - at least not yet. Radiotherapy, at the very least, serves to decrease the chances of local recurrence (not examined in this study), which ultimately may influence patients' quality of life down the road. However, a compelling argument can be made that identification of an effective systemic regimen to eradicate micrometastases and reduce the opportunity for metastasis may not be the most critical factor in improving these patients' chances for long-term survival. The ESPAC-1 study uses only a 5-FU-based chemotherapy regimen; and certainly, a gemcitabine-based approach is the most logical place to start, which was recently evaluated in the RTOG 9704 study [8]. Sub-group analysis of ESPAC-1 suggested a potential role for chemoradiotherapy only in patients with positive resection margins [7]. The CONKO-001 study did not include radiotherapy as a component of either study arm, and hence does not resolve the question of whether radiotherapy is an essential component of adjuvant therapy. On the other hand, RTOG 9704 included infusional 5-FU as a radiosensitizer with concomitant radiotherapy in both study arms. Although this study showed RTOG 9704 did suggest superior results for gemcitabine pre-chemoradiotherapy compared with 5-FU, but this improvement only applied to the subgroup of patients with tumors in the pancreatic head (for head: HR=0.79, 95% CI: 0.63-0.99, P=0.047; for body/tail tumors included: P=0.2) [8]. While both the CONKO-001 and RTOG 9704 studies support the use of gemcitabine as the systemic agent of choice in the adjuvant setting, the benefit of radiotherapy remains inconclusive in randomized trials. Our European colleagues have already commenced ESPAC-3 (Figure 3), the results of this trial will be important in underscoring the value of postoperative adjuvant chemotherapy using the modern chemotherapy (gemcitabine) versus 5-FU in the setting of resected pancreatic adenocarcinoma [16] (Figure 5).
Figure 5. ESPAC-3: trial design.
The story of development of chemotherapy regimens in the metastatic setting has also a bleak landscape. For the past 10 years, many cytotoxic and targeted agents have been pitted against, or combined with, gemcitabine in randomized phase III trials. No drug was shown to be superior to single-agent gemcitabine or when combined with gemcitabine, except two combinations: capecitabine plus gemcitabine vs. gemcitabine and erlotinib plus gemcitabine vs. gemcitabine [17]. It is worth mentioning that the results of these studies of combination chemotherapy regimens in patients with metastatic pancreatic cancer should not be extrapolated to the adjuvant setting, and routine use of such combinations (gemcitabine in combination with erlotinib or capecitabine, or a platinum compound) should not be undertaken in the post-operative adjuvant setting. Mornex et al. presented a multicenter phase II study of post-operative adjuvant gemcitabine plus oxaliplatin chemotherapy followed by chemoradiotherapy in patients with pancreatic carcinoma [18]. Fifty-four patients with potentially curative resection of pathologically confirmed adenocarcinoma of the pancreas with negative resection margins (R0) received gemcitabine 1,000 mg/m2 i.v. over 100 min on day1 and oxaliplatin 100 mg/m2 i.v. over 120 min on day 2 every 2 weeks for 6 cycles followed 4 weeks after by gemcitabine 100 mg/m2 i.v. over 30 min combined with radiotherapy 50 Gy (2 Gy fraction) for 5 weeks. Forty-nine patients received at least two induction cycles. Forty-six patients (85%) received the 6 planned induction cycles and 41 patients (76%) completed chemoradiotherapy. Gemcitabine plus oxaliplatin in post-operative adjuvant setting followed by gemcitabine plus radiotherapy demonstrated 71% of 1-year disease free survival rate with manageable toxicities. However, such results have to be validated in big randomized trials. At the Yale Cancer Center, we generally defer chemo-radiotherapy until after completion of chemotherapy. At that point, for fit patients - particularly those with high-risk features (large tumors, close or microscopically positive margins) and no radiological evidence of recurrent or metastatic disease - we will consider consolidative chemoradiotherapy, typically using capecitabine or infusional 5-FU. Based on the results of CONKO-001, a 6-month course of standardinfusion gemcitabine or a regimen similar to RTOG 9704 (only in head of pancreas) both can be considered appropriate options. Both options yield a median survival of approximately 20 months. However, in light of the systemic nature of pancreatic cancer with high rates of distant recurrence, delivering systemic treatment (gemcitabine) as the immediate next step after surgery before any consideration of radiotherapy is probably the best strategy (modified RTOG 9704 strategy: gemcitabine upfront followed by chemo-radiotherapy). Using this approach, patients who have an early systemic recurrence are selected out and spared the morbidity associated with abdominal radiotherapy. This approach is further strengthened by the fact that there is always a possibility of delaying initiation of chemotherapy by the surgery and then further delay by the initiation of radiotherapy. In the EORTC trial, of 110 patients in the treatment arm, 21 (20%) received no treatment because of excessive delay due to post-operative complications [6]. Investigators of ESPAC-1 study also are of the opinion that delay in the administration of chemotherapy in those patients undergoing combination chemoradiotherapy might explain the inferior outcome [7]. The true incidence and effect of delay due to post-operative complications are unknown. The National Comprehensive Cancer Network (NCCN) recommends that investigational options be considered in all phases of disease management [19]. Additionally, until further data are available, the NCCN recommends postoperative radiotherapy, administered at a dose of 45-54 Gy, with concurrent 5-FU with or without additional chemotherapy (gemcitabine based), or chemotherapy alone (gemcitabine based) for all patients after curative resection for pancreatic cancer, regardless of nodal status. One way of eliminating potential treatment delays that may be associated with adjuvant therapy is to consider neoadjuvant chemoradiotherapy or chemotherapy. In addition, this approach leads to increased survival, down-staging marginal lesions, and sparing patients with rapidly progressive disease unnecessary surgery [20]. Single institution studies including neoadjuvant chemoradiotherapy as well as chemotherapy have shown promise and provide the framework for larger controlled trials evaluating the role of neoadjuvant therapy in the management of both resectable and marginally resectable lesions.
Conclusions
Based on the conflicting results of the studies mentioned above, what is the best modality of adjuvant therapy for a patient who has undergone successful resection for a pancreatic adenocarcinoma, has recovered adequately, and now wants to know how he or she should be treated? The answer is not there yet but at present a 6-month course of standard-infusion gemcitabine (CONKO-001) or a regimen similar to RTOG 9704 (only in head of pancreas) both can be considered appropriate options. However, the best approach will be to enroll the patient on a clinical trial. Early detection strategies, better identification of precursor lesions and highrisk groups, direction of patients to highvolume centers for surgical and oncologicexpertise, and from ongoing trials designed to identify active agents (chemotherapeutic, immunotherapeutic, and other) and implement their use in appropriate patient groups are warranted to improve outcome in this population of patients.
Conflict of interest
The author has no potential conflicts of interest
References
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun
MJ. Cancer statistics, 2007. CA Cancer J Clin 2007;
57:43-66. [PMID 17237035]
- Yeo CJ, Cameron JL, Lillemoe KD, Sitzmann JV,
Hruban RH, Goodman SN, et al.
Pancreaticoduodenectomy for cancer of the head of the
pancreas: 201 patients. Ann Surg 1995; 221:721-3.
[PMID 7794076]
- Lim JE, Chien MW, Earle CC. Prognostic factors
following curative resection for pancreatic
adenocarcinoma: a population- based, linked database
analysis of 396 patients. Ann Surg 2003; 237:74-5.
[PMID 12496533]
- Birkmeyer JD, Warshaw AL, Finlayson SR, Grove
MR, Tosteson AN. Relationship between hospital
volume and late survival after
pancreaticoduodenectomy. Surgery 1999; 126:178-83.
[PMID 10455881]
- Kalser MH, Ellenberg SS. Pancreatic cancer.
Adjuvant combined radiation and chemotherapy
following curative resection. Arch Surg 1985; 120:899-
903. [PMID 4015380]
- Klinkenbijl JH, Jeekel J, Sahmoud T, van Pel R,
Couvreur ML, Veenhof CH, et al. Adjuvant
radiotherapy and 5-fluorouracil after curative resection
of cancer of the pancreas and periampullary region:
phase III trial of the EORTC gastrointestinal tract
cancer cooperative group. Ann Surg 1999; 230:776-82.
[PMID 10615932]
- Neoptolemos JP, Stocken DD, Friess H, Bassi C,
Dunn JA, Hickey H, et al. A randomized trial of
chemoradiotherapy and chemotherapy after resection
of pancreatic cancer. N Engl J Med 2004; 350:1200-10.
[PMID 15028824]
- Regine WF, Winter KW, Abrams R, Safran H,
Hoffman JP, Konski A, et al. RTOG 9704 a phase III
study of adjuvant pre and post chemoradiation (CRT)
5-FU vs. gemcitabine (G) for resected pancreatic
adenocarcinoma J Clin Oncol 2006; 24(18S):4007.
ASCO Annual Meeting Proceedings (Post-Meeting
Edition).
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr
J, Ridwelski K, et al. Adjuvant chemotherapy with
gemcitabine vs observation in patients undergoing
curative-intent resection of pancreatic cancer: a
randomized controlled trial. JAMA 2007; 297:267-77.
[PMID 17227978]
- Burris HA, Moore MJ, Andersen J, Green MR,
Rothenberg ML, Modiano MR, et al. Improvements in
survival and clinical benefit with gemcitabine as firstline
therapy for patients with advanced pancreas
cancer: a randomized trial. J Clin Oncol 1997;
15:2403-13. [PMID 9196156]
- Picozzi VJ, Kozarek RA, Traverso LW. Interferonbased
adjuvant chemoradiation therapy after
pancreaticoduodenectomy for pancreatic
adenocarcinoma. Am J Surg 2003; 185:476-80. [PMID
12727570]
- Laheru D, Jaffee EM. Immunotherapy for
pancreatic cancer: science driving clinical progress.
Nat Rev Cancer 2005; 5:459-67. [PMID 15905855]
- Jaffee EM, Hruban RH, Biedrzycki B, Laheru D,
Schepers K, Sauter PR, et al. Novel allogeneic
granulocyte-macrophage colony-stimulating factorsecreting
tumor vaccine for pancreatic cancer: a phase I
trial of safety and immune activation. J Clin Oncol
2001; 19:145-56. [PMID 11134207]
- Laheru D, Yeo C, Biedrzycki B, Solt S, Lutz E,
Onners B, et al. A safety and efficacy trial of lethally
irradiated allogeneic pancreatic tumor cells transfected
with the GM-CSF gene in combination with adjuvant
chemoradiotherapy for the treatment of
adenocarcinoma of the pancreas. J Clin Oncol 2007;
25(18S):3010. ASCO Annual Meeting Proceedings
(Post-Meeting Edition).
- Reya T, Morrison SJ, Clarke MF, Weissman IL.
Stem cells, cancer, and cancer stem cells. Nature 2001;
414:105-11. [PMID 11689955]
- Owen E. ESPAC-3(v2) Adjuvant Chemotherapies
in Resectable Pancreatic Cancer. The University of
Liverpool. Division of Surgery and Oncology.
Accessed July 19th, 2007.
- Saif MW. Pancreatic cancer: is this bleak
landscape finally changing? Highlights from the '43rd
ASCO Annual Meeting'. Chicago, IL, USA. June 1-5,
2007. JOP. J Pancreas (Online) 2007; 8:365-73. [PMID
17625289]
- Mornex F, André T, Louvet C, Seitz J, Ychou M,
Lledo G, et al. Postoperative adjuvant gemcitabine plus
oxaliplatin (GemOx) chemotherapy followed by
chemoradiation in patients with pancreatic carcinoma:
A multicenter phase II study. J Clin Oncol 2007;
25(18S):4520. ASCO Annual Meeting Proceedings
(Post-Meeting Edition).
- Tempero MA, Behrman S, Ben-Josef E, Benson
AB, Cameron JL, Casper ES, et al. Pancreatic
adenocarcinoma: Clinical Practice Guidelines in
Oncology. J Natl Compr Canc Netw 2005; 3:598-626.
[PMID 16194453]
- Tempero MA, Behrman S, Ben-Josef E, Benson
AB, Cameron JL, Casper ES, et al. Pancreatic
adenocarcinoma: Clinical Practice Guidelines in
Oncology. J Natl Compr Canc Netw 2005; 3:598-626.
[PMID 16194453]






