Keywords
Pancreas Measurement; Computed Tomography;
Ultrasound
Abbreviations
AP Anterior-Posterior; AC Abdominal Circumference;
SMV Superior Mesenteric Vein
Introduction
Pancreas is an elongated, accessory retroperitoneal
organ that lies between the duodenum on the right and
the spleen on the left [1]. Increasing age is associated with
reduction in size of body, tail and volume of the pancreas
[2, 3]. During childhood and adolescence, the volumes of
the total pancreas, pancreatic parenchyma and fat increase
linearly with age [4]. From age 20 – 60years, pancreas
volume reaches a peak and start declining afterwards [4, 5, 6, 7]. Mentioned in many studies is the relationship
between pancreas size, ethnicity, body weight, genetic
makeup and nutritional status [8, 9, 10]. Pancreatitis is one
of the commonest pancreatic pathology encountered in
clinical practice, and early detection significantly reduces
the mortality and morbidity [11]. Pancreatic cancer is the
twelfth most common cancer in the world [12] and fourth
leading cause of cancer deaths in both men and women
[9]. Attempts had been made to demonstrate the effect of certain diseases like diabetes mellitus type 1 & 2 on the
pancreas [13, 14, 15, 16].
Radiological imaging of pancreas is important tool
in early detection and staging of pancreatic diseases.
Diagnosing pancreatic lesion requires multimodality
approach [17, 18]. Abdominal ultrasound and computed
tomography (CT) are the most frequently used modalities
in evaluation of pancreatic lesion [19, 11]. Abdominal
ultrasound is widely available, even in developing
countries and it is non- invasive and inexpensive with no
risk of radiation effect or adverse effect of contrast agent
[20, 21]. Although the anatomical position of pancreas,
overlying bowel gas and level of sonographer’s experience
pose difficulties in ultrasound imaging of pancreas [22], it
is usually the first choice imaging modality [19, 23].
Since introduction of CT in late 1970’s, it has found
wide application in radiological investigations [24, 25].
Contrast-enhanced multi-slice CT remains the gold
standard in imaging acute pancreatitis and pancreatic
cancer [26, 27, 28, 29], significantly better than ultrasound
in demonstration of pancreas body and tail [30]. Unlike
developed countries, CT is not readily available in Nigeria
[31, 32]. The cost of diagnostic CT examinations is a
limitation to its utilization in developing countries [33].
In spite of the benefit of CT in imaging of pancreas, it has
associated radiation dose risk [34].
In view of the risk of radiation associated with CT and
limitations of ultrasound imaging of the pancreas, it is paramount that a study to compare pancreatic biometry
on both modalities be carried out to validate ultrasound
findings. Therefore, this study is to evaluate the pancreas
in normal adult Lagos population using computed
tomography and ultrasonography.
METHODS
Using convenient sampling method, 150 adult
outpatients were prospectively scanned using both
abdominal CT and US scans at Clinix Healthcare, Alhaji
Adejumo Avenue, Ilupeju, Lagos State. Ethical approval
was obtained from the relevant Research and Ethics
Committee board. Informed consent was obtained from
each of the patients that consented to participate in the
study before commencement of scan. Absolute patient
confidentiality was observed. Only patients who met the
inclusion criteria were included in the study. Exclusion
criteria were patients younger than 20 years and/or with
a past or present history of pancreatico-biliary disorders
including diabetes mellitus, and patients with abnormal
findings like presence of CT signs of any pancreatic or peripancreatic
pathology, presence of ascites or abdominal mass
compressing on pancreas, scan error or artefact that would
interfere with the ability to recognize the pancreatic contour,
scan with inadequate opacification of the duodenum, and
patient with limited ultrasound visualization of pancreas
segments. On the whole, 83 cases did not qualify for inclusion
based on the exclusion criteria and were thus excluded.
The CT scans were performed on 64-slice Siemens
SOMATOM perspective CT scanner machine with the
following product features: Cardiac imaging with rotation
time of 33s, Isotropic special resolution of 24 mm, Spiral
artifact free imaging, STRATON high performance CT x-ray
tube, Z-sharp technology, and UFC detectors. Ultrasound
scans were carried out using SonoAce X8 (Medison
inc., Korea 2015) ultrasound machine with 3.5MHz
curvilinear probes. The transducer gain control was
adjusted to optimize visualization of the entire pancreas.
Body weight measurement was made with a weight scale
(RGZ- 160) manufactured in the year 2015 by Health &
Medical Equipment, England. Its weight range is 0 –160
kgs. Standing height was measured with a stadiometer
(seca 213) manufactured in the year 2008 by seca gmbh &
co.kg, Germany. The measuring range in cm is 20-205cm.
Abdominal circumference was measured with measuring
tape. Uni-dimensional measurements of the pancreas
head, body, and tail were taken on both CT and US. All the
measurements were recorded in a prepared data sheet. AP
diameters of pancreas head, body and tail were obtained
from same patients on Ultrasonography and Computed
Tomography.
The CT measurements were taken from the advantage
workstation, operator consul, of the CT machine. A
scanogram/scout was obtained to determine the range
of the scan for the procedure. In most cases, pre-contrast,
contrast and delay protocols were obtained. Pancreas
segments dimensions were taken for patients that met the
inclusion criteria after review by experienced radiologist. All measurements were obtained from the axial CT images
through the middle of the pancreatic head, body and tail.
Anterior-posterior (AP) dimensions were measured at
right angles to the longitudinal axis of the organ. The
largest diameter of the pancreas lying to the left of the
middle of the vertebral body was considered the head.
The head was measured on the scan slice that had the
plumpest pancreatic head. The body of the pancreas was
measured on the left margin of the vertebral body and the
tail opposite to the medial margin of the left kidney. The
transverse diameter of the adjacent vertebral body was
used as a reference as applied by Heuck et al. [5].
On ultrasound, patients were positioned in supine
position. Longitudinal scan (scout) of the epigastric region
was performed to identify the major upper abdominal
vessels such as aorta, coeliac axis, superior mesenteric
artery and vein, and splenic vein. Although the level
of pancreas body was identified in longitudinal scan,
pancreas itself was not clearly demonstrated. Transverse
trans-abdominal scans of the pancreas were performed at
a level 2.5-5 centimetres below the xyphisternum (20 - 30o
cranially) with the left lobe of the liver serving as acoustic
window into the pancreatic bed. Abdominal aorta, inferior
vena cava, superior mesenteric vein (SMV), portal vein,
and splenic vein were used as landmarks. In general, to
improve visualization of the pancreas, especially in cases
where it was poorly seen with the patient supine, the water
technique was used whereby patient drank some water to
displace stomach gas and provide acoustic window into the
pancreas. In some cases, semi-erect position was adopted
to displace epigastric bowel gas. The pancreatic tail was
imaged in the diagonal coronal plane with the patient
in the supine (30–45°) right posterior oblique position.
Some examinations were performed with patient in the
decubitus position. Change in position helped to overcome
difficulties arising from bowel gas [35]. AP Pancreas head,
body and tail dimensions were measured using technique
adopted by Meire & Farrent [36].
Assessment of intra-observer and inter-observer
reliability was performed. Thirty patients who met the
inclusion criteria were selected to evaluate the reliability
of the measurements of the pancreas segments, both on
CT and US scans technique. Two independent radiologists
with more than ten years’ experience, each made two
different measurements of the pancreas segments for
each patient, both on CT and US scans technique. They
were blinded to each other’s results for all the subset. The
measurements were subjected to paired sample T-test and
showed no significant difference in intra-observer reading
and inter-observer reading for the two modalities.
The collected data was categorized according to patient’s
age and sex, height, weight, BMI, and abdominal circumference
(AC). All data obtained in the study was documented and
analysed using SPSS version 23 for windows. Descriptive
statistics, mean ± standard deviation (SD), maximal (Max),
and minimal (Min) values were used. Independent samples
t- test was used to estimate the sex-related differences. Pearson’s correlation coefficient was used to evaluate
the correlations of the size of the pancreas with the
subject’s age, and parameters of body character. P-value
of less than 0.05 was considered to be statistically
significant. Linear regression models were performed
between the variables.
RESULTS
Table 1 showed that the mean age, height, weight, AC,
and BMI of the subjects were 48yrs, 161cm, 73Kg, 95cm
and 28 Kg/cm2 respectively.

It can be seen from Table 2 that on US, the mean AP
diameter of the pancreas head, body, and tail in the studied
population were 25.10 ± 2.75 mm (Range: 18.80 – 30.50
mm), 15.98 ± 1.86mm (Range: 10 – 20 mm), and 13.50
± 1.53 mm (Range: 10 – 17 mm) respectively. On CT, the
mean ± SD AP pancreas diameters of head, body , and tail
in the studied population were 26.77 ± 2.68 mm (Range
: 21.40 – 32.30 mm), 21.19 ± 2.12 mm (Range: 16.20 –
25.50mm), and 17.25 ± 2.12 mm (Range: 11.5 – 22.20
mm) respectively.

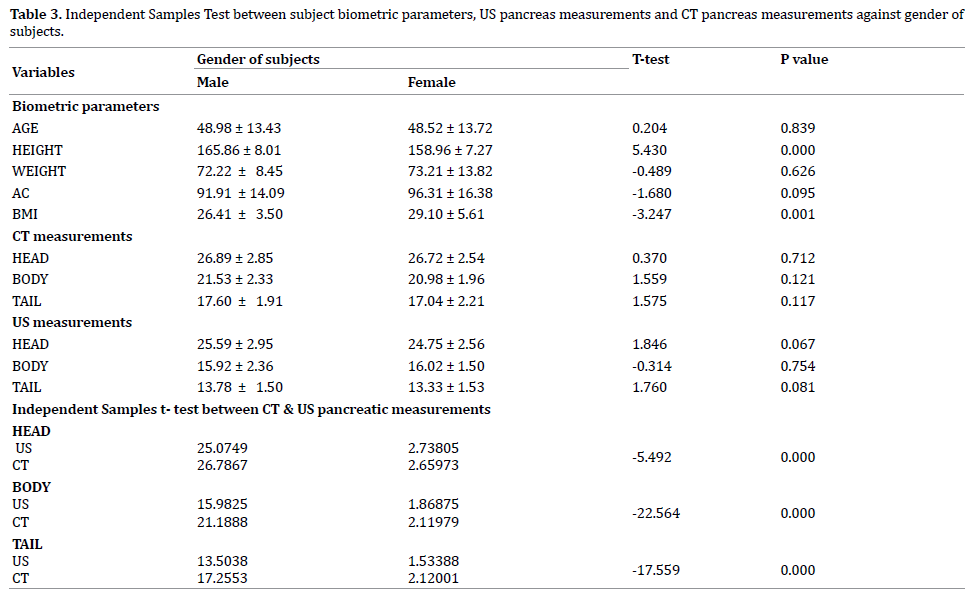
Table 3 showed that male subjects were significantly
taller than the female subjects (P< 0.001). Also, BMI
values of female subjects are significantly greater than
that of male subjects (P< 0.005). The mean pancreatic size
measurements in males were larger than in females but the
variation between the genders was not significant. It also
showed that Pancreas segments dimensions measured on
CT were significantly larger than that measured on US. The
result of independent samples T-Test revealed that only
height and BMI of the subjects were significantly different
between the genders (p<0.05). Independent sample t-test
performed between US values and CT values showed that
diameters of the pancreas segments measured on CT were
significantly larger than that measured on US (P= 0.000).
From the correlation analysis table, it can be seen that
for US measurements: Age showed strong correlation with
pancreas size; Pancreas head diameter correlated well
with subjects’ height; Pancreas head and tail correlated
with weight and; Pancreas body diameter correlated
with AC and BMI (P<0.05). For the CT measurements,
it was observed that: Age showed strong correlation
with pancreas size; Pancreas head and tail diameters
correlated well with subjects’ height and; Pancreas tail
correlated with weight (P<0.05). It was also shown from
the regression equations that there is linear relationship
between the pancreatic size and patient age (years), height
(cm), Abdominal Circumference (cm), weight (kg), and
BMI (Table 4).

ANOVA test performed to compare the mean of
measured AP diameters of pancreas segments on US and
CT according to age groups showed significant difference
at P < 0.05. Pancreas head, body, and tail diameter were
noted to differ between the age groups and to decline from
age 60years and above.
It can be observed that there is linear relationship
between ultrasound and CT pancreas measurements for
all the pancreatic segments. Equations were established
between pancreas diameters measured on CT and US:
US pancreas head size = 15.69 + 0.3501 x CT pancreas
head size.
US pancreas tail size = 9.31 + 0.2655 x CT pancreas tail
size.
US pancreas body size = 17.20 + 0.0898 x CT pancreas
body size.
DISCUSSION
Clinical examinations and routine radiological method
of evaluating pancreas are insensitive and non-specific in
diagnosis [37]. Other methods of evaluating the pancreas
such as endoscopic retrograde cholangiography (ERCP),
pancreatic arteriography, Percutaneous transhepatic
cholangiography have improved sensitivity and accuracy
but they are invasive procedures [37]. Ultrasonography
(US) and computed tomography (CT) of the pancreas
provide better and higher quality pancreas imaging and
thus, are the most frequently used modalities in evaluation
of pancreatic lesions [19, 11].
This study was carried out to compare normal US and
CT biometry of pancreas segments in normal Lagos State
adult population. Comparative study of pancreas size
measurements on US and CT showed that CT is better
modality in demonstration of pancreas segment especially
the tail in accordance with the findings of Kolmannskog et
al. [32]. Independent Sample T-Test performed between
US values and CT values showed that diameters of the
pancreas segments measured on CT were significantly
larger than that measured on US (P= 0.000) (Table 1).
The difference could be attributed to inclusion of splenic
veins and superior mesenteric veins to the diameter
of pancreas measured on CT. US was more effective in
distinguishing pancreas from surrounding vessels. This
agreed with the work of Kolmannskog et al. [32] who
compared pancreas segment diameters measured on
CT and US on same patients. They included 47 patients
in the study (Table 5, 6). Paivansalo [38] measured pancreas size on US and CT in 70 patients without
pancreas disease and reported that in 87% of the cases,
pancreas segments diameter measured by CT were
thicker than by US. However, he maintained that US was more effective in distinguishing pancreas parenchyma
from the surrounding retroperitoneal fat and vessels.
Equations (I, ii, iii) were established between pancreas
dimensions measured on CT and US (Figures 1-5).


Figure 1. AP Pancreas head and body dimensions on CT.
Figure 2. AP Pancreas tail dimension on CT.
Figure 3. AP Pancreas head dimension on US.
Figure 4. AP Pancreas body dimension on US.
Figure 5. AP Pancreas tail dimension on US.
US pancreas head size = 15.69 + 0.3501 x CT pancreas
head size…...(i)
US pancreas body size = 10.42 + 0.2698 x CT pancreas
body size......(ii)
US pancreas tail size = 9.82 + 0.2155 x CT pancreas
tail size………(iii)
CONCLUSION
Dimensions of the pancreas segments measured on CT
were significantly larger than that measured on US (P=
0.000). Ultrasound was more effective in distinguishing
pancreas from surrounding vessels.
Conflict of interest
There is no conflict of interest.
References
- Parson SH. Clinically Oriented Anatomy, 6th edn. J Anat 2009; 215:474. [PMICID: PMC2766067]
- Syed AB, Mahal RS, Schumm LP, Dachman AH. Pancreas size and volume on computed tomography in normal adults. Pancreas 2012; 41:589-95. [PMID: 22158073].
- Sato T, Ito K, Tamada T, Sone T, Noda Y, Higaki A, et al. Age-related changes in normal adult pancreas: MR imaging evaluation. Eur J Radiol 2012; 81:2093-8. [PMID: 21906894].
- Saisho Y, Butter AE, Meier JJ, Monchamp T, Allen-Auerbach M, Rizza RA, et al. Pancreas volumes in humans from birth to age one hundred taking into account sex, obesity, and presence of type -2 diabetes. Clinical Anatomy 2007; 20: 933-42.
- Heuck A, Maubach PA, Reiser M, Feuerbach S, Allgayer B, Lukas P, et al. Age-related morphology of the normal pancreas on computed tomography. Gastrointest Radiol 1987; 12:18-22. PMID: 3792751].
- David AS, Paul SB. Paediatric Gastrointestinal imaging and intervention, 2nd edn. 699.
- Caglar V, Songur A, Yagmurca M, Acar M, Toktas M, Gonul Y. Age-related volumetric changes in pancreas: a stereological study on computed tomography. Surg Radiol Anat 2012; 34:935-41. [PMID: 22684677]
- Chao HC, Lin SJ, Kong MS, Luo CC. Sonographic evaluation of the pancreatic duct in normal children and children with pancreatitis. J Ultrasound Med 2000; 19:757-63. [PMID: 11065264].
- Yadav D, Lowenfels AB. The epidemiology of pancreatitis and pancreatic cancer. Gastroenterology 2013; 144:1252-61. [PMID: 23622135]
- Hassan AF, Ayad CE, Ebrahim TEM, Abdalla EA. Characterization of pancreas in Sudanese population of computed tomography. Int J Biomed Imaging 2014; 2:199-124.
- Ullal S, Joshi KS, Pant P. Computed Tomographic Evaluation of Pancreatitis and its complications. Pictoral review. Nepal J Med Sci 2012; 1:123-131.
- Ferlay J, Soerjomataram I, Dikshit R, Eser S, Mathers C, Rebelo M, et al. Cancer incidence and mortality worldwide: sources, methods and major patterns in GLOBOCAN 2012. Int J Cancer 2015; 136:E359-86. [PMID: 25220842]
- Alzaid A, Aideyan O, Nawaz S. The size of the pancreas in diabetes mellitus. Diabet Med 1993; 10:759-63. [PMID: 8261759]
- Vesterhus M, Haldorsen IS, Raeder H, Molven A, Njølstad PR. Reduced pancreatic volume in hepatocyte nuclear factor 1A-maturity-onset diabetes of the young. J Clin Endocrinol Metab 2008; 93:3505-9. [PMID: 18593771]
- Acar M, Degirmenci B, Tatli S. Short pancreas: evaluation with multi-detector row CT. Surg Radiol Anat 2010; 32:853-8. [PMID: 20165948]
- Agabi JO, Akhigbe AO. Comparative sonographic evaluation of the anteroposterior dimensions of the pancreas in diabetics and nondiabetics. Niger J Clin Pract 2016; 19:175-81. [PMID: 26856277]
- Catalano C, Laghi A, Fraioli F, Pediconi F, Napoli A, Danti M, et al. Pancreatic carcinoma: the role of high-resolution multislice spiral CT in the diagnosis and assessment of resectability. Eur Radiol 2003; 13:149-56. [PMID: 12541123]
- Chaudhary V, Bano S. Imaging of the pancreas: Recent advances. Indian J Endocrinol Metab 2011; 15(Suppl 1):S25-32. [PMID: 21847450]
- Tummala P, Junaidi O, Agarwal B. Imaging of pancreatic cancer: An overview. J Gastrointest Oncol 2011; 2:168-74. [PMID: 22811847]
- Rickes S, Unkrodt K, Neye H, Ocran KW, Wermke W. Differentiation of pancreatic tumours by conventional ultrasound, unenhanced and echo-enhanced power Doppler sonography. Scand J Gastroenterol 2002; 37:1313-20. [PMID: 12465731]
- Abam RO, Nwankwo NC. Sonographic measurement of the antero-posterior diameter of the head of pancreas in normal adult population in Port- Harcourt, South- South Nigeria. J Med Medical Sci 2011; 2:1162-117.
- Sirli R, Sporea I. Ultrasound examination of the normal pancreas. Med Ultrason 2010; 12:62-5. [PMID: 21165455]
- Lalith S, Ilangovan G. Comparative study of ultrasonography and computed tomography in diagnosis of acute pancreatitis. Inter J Contem Med Surg Rad 2019; 4:C28-C33
- Lower AS, Kay CL. Recent Development in CT: Review of the clinical applications and advantages of multi-detector CT. Imaging 2006; 18: 62-67.
- Brenner DJ, Hall EJ. Computed tomography--an increasing source of radiation exposure. N Engl J Med 2007; 357:2277-84. [PMID: 18046031]
- Patel SV, Spencer JA, el-Hasani S, Sheridan MB. Imaging of pancreatic trauma. Br J Radiol 1998; 71:985-90. [PMID: 10195019]
- Von-Hoff DD, Evans DB, Hruban RH. Pancreatic cancer. Endoscopic staging: EUS, ERCP. Sudbury: Jones and Bartlett Publishers. 2005; 181–190.
- William RJ. Blumgant‘s Surgery of liver pancreas and biliary tract. 2012; 843.
- Hirota M, Satoh K, Kikuta K, Masamune A, Kume K, Hamada S, et al. Early detection of low enhanced pancreatic parenchyma by contrast-enhanced computed tomography predicts poor prognosis of patients with acute pancreatitis. Pancreas 2012; 41:1099-104. [PMID: 22699199]
- Kolmannskog F, Swensen T, Vatn MH, Larsen S. Computed tomography and ultrasound of the normal pancreas. Acta Radiol Diagn (Stockh) 1982; 23:443-51. [PMID: 7158408]
- Erondu OF, Okoro CR, Aniemeka JI, Ugwu AC. Patterns of CT referrals among physicians in the South-South region of Nigeria. American J Sci Indus Res 2011; 2:482-487.
- Uduma UF, Eduwem UD, Obong VJ. 288 Pioneer Computed Tomographic Examinations in University of Uyo Teaching Hospital, Uyo, Nigeria. Int J Trop Dis Health 2014; 4:233-243
- Saini S, Sharma R, Levine LA, Barmson RT, Jordan PF, Thrall JH. Technical cost of CT examinations. Radiology 2001; 218:172-5. [PMID: 11152797]
- Shrimpton PC, Hillier MC, Lewis MA, Dunn M. National survey of doses from CT in the UK: 2003. Br J Radiol 2006; 79:968-80. [PMID: 17213302]
- Muffin J. The Pancreas. In: David Sutton editor. Text book of Radiology and Medical Imaging. Churchill Livingstone, Edinburgh 2007.
- Meire HB, Farrant P. Pancreatic ultrasound--a systematic approach to scanning technique. Br J Radiol 1979; 52:562-7. [PMID: 465941]
- Lee JK, Stanley RJ, Melson GL, Sagel SS. Pancreatic imaging by ultrasound and computed tomography: a general review. Radiol Clin North Am 1979; 17:105-117. [PMID: 461738]
- Päivänsalo M. Normal pancreatic echogenicity: relation to structural unevenness and thickness in CT. Ann Clin Res 1984; 40:69-71. [PMID: 6732175]






