Keywords
Infectious pancreatic necrosis virus; Pancreatitis, Acute
Necrotizing
Abbreviations
CT computed tomography; ERCP endoscopic
retrograde cholangiopancreatography; FNAB fine needle aspiration for
bacteriology; PCD percutaneous drainage
INTRODUCTİON
Acute necrotizing pancreatitis accounts for 10-15% of
all cases of acute pancreatitis. It is frequently accompanied
by a systemic inflammatory response syndrome and
multisystem organ failure and occasionally by infected
necrosis [1, 2]. Depending on the presence or absence of
necrosis, acute collections in the first four weeks are called
acute necrotic collections or acute peripancreatic fluid
collections. Once an enhancing capsule develops, persistent
acute peripancreatic fluid collections are referred to
as pseudocysts; and acute necrotic collections, as walledoff necrosis. All can be sterile or infected. The revised
classifications are used to standardize the terminology
among the radiologists, gastroenterologists, surgeons, and
pathologists to facilitate treatment planning and enable
precise communication among different departments and
institutions [3].
MATERIALS AND METHODS
The study was performed from January 2012 to January
2017. There were 126 consecutive patients (103 men
and 23 women; median age 39 years) with necrotizing
pancreatitis who underwent percutaneous catheter
drainage via CT guidance and were evaluated according
to the clinical criteria, radiological scores, drainage and
catheter characteristics, and complications. A retrospective
review of our cross-sectional interventional radiology
database over 60 months (5 years) identified all patients
who underwent primary CT-guided percutaneous drainage
(PCD) for acute necrotizing pancreatitis. Assessment of
the patient's clinical condition at initial percutaneous CTguided
PCD was based on criteria set forth by the revised
classification of Acute Pancreatitis – 2012, revision of
Atlanta classification, 1992. The revised classification
identifies early and late phases of the disease and classifies into mild, moderate and severe acute pancreatitis. The
mild acute pancreatitis has no organ failure, no local or
systemic complications. The moderate acute pancreatitis
has transient organ failure or local complications or
exacerbation of co-morbid diseases. The severe acute
pancreatitis has persistent organ failure for more than
48 hours [3]. The initial CT findings were calculated
according to the Modified CT Severity index. The Modified
CT Severity Index is a scoring system that incorporates the
extent of pancreatic necrosis (none, <30% or >30%) along
with peripancreatic inflammation (presence or absence of
fluid collections).
Procedures
Referral for radiological intervention was based on
suspicion of infection raised by fever, leucocytosis, renal
or cardiac compromise or general clinical deterioration
refractory to conservative medical care. The decision for
PCD was always multidepartment based on referral from
the clinical team for persistent sepsis, and departmental
guidelines according to the American College of Radiology
appropriateness criteria with radiological imaging
suggesting a liquefied drainable collection, rapidly
enlarging collections, collections larger than 5 cm,
collections causing obstruction and infected collections
[4]. Infection in the collection was assessed on the imaging
picture (collection with gas or the collection density has
higher Hounsfield Units than water) and in indeterminate
cases with prior needle aspiration. The Seldinger technique
was systematically used to place a catheter in each of the
necrotic collections via the most direct transperitoneal
route, avoiding intervening bowels and solid organs. One
or more multiperforated double-sump 14- to 16- French
catheters were placed to aspirate the cavity fluid and to
start with continuous irrigation with 1 L/drain/day of
normal saline. Later the new larger catheter was inserted
after sequential dilation. The goal was to increase the
diameter of the catheter to a maximum of 28–32 French
large-bore catheters whose distal holes were expanded
manually (Sherwood, Argyle) and additional holes made
where ever required. As for the initial drainage, continuous
and abundant daily irrigation was initiated, ranging from
0.5 to 1.5 L/drain/day of normal saline, depending on the
size of the collection. The decision to remove the catheters
and stop the drainage was based on clinical improvement
(i.e., control of the sepsis and hemodynamic stability),
resolution of the necrotic cavity on CT scan and when the
amount of drain fluid was less than 20 mL/day. The mean
time between presentation with pancreatitis and the first
interventional procedure was 25 days (range, 12-65 days).
Patient Outcome
Patient outcome was categorized into four groups:-
control of sepsis and successful collection resolution on
PCD (A); successful collection resolution on PCD but later
Surgery (B); treatment failure on PCD then Surgery (C);
treatment failure on PCD & Surgery then Death (D). Control
of sepsis and successful resolution on PCD, was defined
as normalization of vital signs, resolution of leukocytosis and complete resolution of the collection with less than 10
ml daily drain output. The successful resolution on PCD
and later surgery, was defined as complete resolution of
the collection but, persistent sepsis likely secondary to
infected phlegmon leading to surgery. Treatment failure
on PCD and then surgery, was defined as incomplete
resolution of collection or multiple inaccessible loculated
collections not amenable to PCD drainage and persistent
sepsis warranting surgery. The treatment failure on PCD
and the surgery and death, was defined as incomplete
resolution of the collection on PCD and severe sepsis not
controlled by surgery ultimately leading to death. The
total length of hospital stay, length of hospital stay after
the initial percutaneous catheter drainage procedure and
the number of days elapsed before surgical debridement
was calculated. Cause of death and interval between
interventional procedure or surgery and patient death were
recorded. Complications related to the PCD interventional
procedures were recorded as hemorrhage, Pancreatico –
cutaneous Fistula, Pancreatico – enteric Fistula, Pancreatic
Abscess.
RESULTS
The successful drainage outcome is grouped into,
control of sepsis by PCD or complete resolution of
liquefied collection by PCD or stabilization of patient for
elective surgery, if needed. Successful PCD outcome i.e.
collection resolution was achieved in 108 (A+B) of 126
patients (85.7%). No surgery was required in 95 patients
(A) (75%). Of these 108 patients, 13 patients (B) had the
liquefiable part of the collection drained by PCD, but the
phlegmon caused persistent sepsis, and had to undergo
elective surgical necrosectomy, however, PCD helped in
stabilizing these patients and reducing the septic load in
the body for better surgical outcome. Rest of the 18 patients
did not have a successful outcome on PCD; of these, 16
patients (C) had treatment failure on PCD then surgery was
performed, and 2 patients (D) passed away with treatment
failure on PCD and surgery. Moderate pancreatitis
was observed in 102 patients and were managed with
PCD and surgery was not avoided. Severe pancreatitis
was observed in 24 patients, of those, 8 patients were
stabilized with PCD and elective surgery was performed
to remove non-liquefied infected phlegmon; 16 patients
had treatment failure on PCD and had to undergo surgical
necrosectomy; and 2 unfortunately had treatment failure
on PCD and with surgery and died. The procedure-related
complications were observed in six patients of which one
had hemorrhage due to the catheter eroding the vessel
and five had a pancreatico-cutaneous fistula. None of these
complications were lethal. Pancreatico-enteric fistula
developed in 3 patients and was not procedure related.
They underwent surgical management. Of the total 126
patients, 110 patients were managed as outpatients with
regular clinic visits. The major causes of acute pancreatitis
were cholelithiasis; alcohol, ERCP, hypertriglyceridemia,
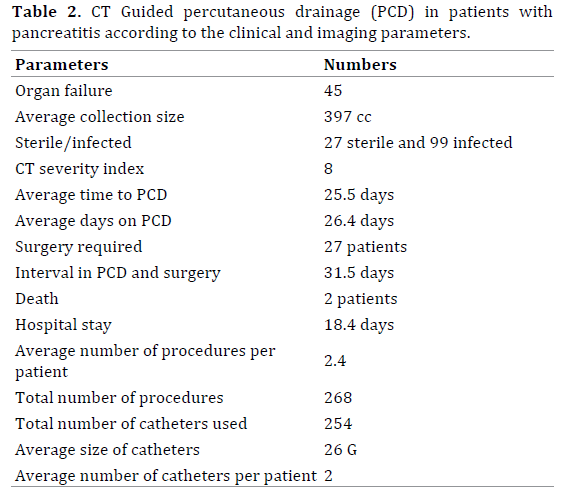
autoimmune, trauma and idiopathic. The detailed results
are listed in Tables 1, 2.

DISCUSSION
The mainstay of treatment of patients with acute
necrotizing pancreatitis traditionally has been surgical
debridement, however, morbidity with surgery has been
between 43%-89% and mortality between 9%-39% [5].
This high rate has been largely attributed to the presence of
comorbid medical conditions, including multisystem organ
failure, derived from a systemic response to pancreatitis.
Despite the availability of several clinical (Ranson criteria,
Acute Physiology and Chronic Health Evaluation II score)
and radiologic (Balthazar scoring system, modified CT
severity index) grading systems, accurate prediction
of outcome and best treatment of patients with acute
necrotizing pancreatitis remains difficult. The risk of
infection increases with the duration of the disease,
reaching a peak during the third week with an incidence
rate of 71% [6, 7]. Clinical, biologic, and radiologic signs
are not specific enough to reveal infection of the necrosis.
Many recent studies suggested that routine laboratory
parameters like blood urea nitrogen, hematocrit,
procalcitonin, C-reactive protein, and creatinine have a
significant association in predicting the occurrence of
infected pancreatic necrosis secondary to necrotizing
pancreatitis [8, 9]. Aspiration and culture can provide
bacteriologic confirmation of infection with both high
sensitivity and specificity [10]. It is generally accepted that,
in IPN, the infected non-vital solid tissue has to be removed
to control the sepsis. Surgical necrosectomy has been the
preferred treatment of years, with very variable mortality
rates ranging from 3% to 42% [11]. Common complications
of necrotizing pancreatitis are a pancreatic abscess, pancreatico-cutaneous fistula, pancreatico-enteric fistula,
and hemorrhage. The pancreatic abscesses, can be treated
with debridement and lavage. The pancreatico-cutaneous
fistula results when the pancreatic secretions leak through
the drain site or wound. The role of percutaneous catheter
drainage in such cases is to help closure of fistula with
drainage of fluid collection. Octreotide helps in reducing
exocrine pancreatic secretions in cases of pseudocyst
recurrence, pancreatic fistula from percutaneous drainage,
or elective treatment to restrict pancreatic drainage [12, 13]. Pancreatico-enteric fistula, is leakage of pancreatic
secretions into the bowl, either duodenum or colon. These
can be managed with transpapillary stenting of disrupted
pancreatic duct or surgery. Life-threatening hemorrhage
into the gastrointestinal tract, retroperitoneum, or
peritoneal cavity complicates acute pancreatitis in only
1–3% of patients. CT angiography and digital subtraction
mesenteric angiography can detect the bleeding site in
approximately 80% of cases and arterial embolization can
achieve definite hemostasis in 35–50% and helps stabilize
critically ill patients to permit elective surgery [14].
PCD of IPN is a well-recognized minimally invasive
alternative treatment to primary surgical necrosectomy.
Freeny et al. first described a homogeneous group of 34
patients exclusively treated by PCD for IPN using precise
definitions of necrosis and infection. They recorded a
clinical success rate of 47% and were able to identify
multiorgan failure and central necrosis on CT as two
predicting factors of poor response to catheter drainage
[15]. The clinical success and mortality rely mainly and
strongly on the commitment and the close cooperation
among radiologists, surgeons, gastroenterologists, and
intensivists who are willing to take care of such patients.
Image guided PCD has been found to be an effective
alternative to surgical debridement in the treatment of
selected patients with infected pancreatic necrosis. Wasler et al. has evaluated the clinical utility of CT-guided PCD in
patients with sterile pancreatic necrosis and concluded
no benefit in draining sterile collections versus simple
aspiration, however, there is increased risk of bacterial
colonization [16]. It is conceivable, however, that a
patient with sterile necrosis whose condition continues
to deteriorate despite aggressive supportive therapy may
also benefit from percutaneous catheter drainage [17]
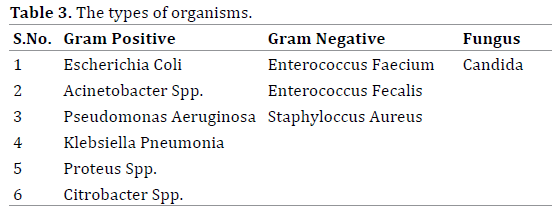
(Figures 1, 2). In infected pancreatic collections, the most
common gram-negative organism isolated was Escherichia
Coli and the most common gram-positive organism was
Enterococcus Faecium. Few patients had polymicrobial
infection [18]. The types of organisms isolated are included
in Table 3.
Figure 1. Coronal and axial CT images showing large collection along the pancreatic tail extending along the left paracolic gutter up to the pelvis with
multiple air foci suggesting abscess formation (White sold arrow).
Figure 2. Coronal images of the same patient showing multiple pigtail drainage catheters (14 Fr) within the collection (White Solid arrows).
In our study, the sterile necrosis was found in 21% of
patients and this did not correlate with patient outcome.
This observation supports the hypothesis, substantiated
by other investigators, that multisystem organ failure
is a more reliable indicator of poor patient outcome and
severity of severe pancreatitis than is the presence of
infected necrosis [19]. Our study also had similar outcome
with worse prognosis and multiple procedures in patients
with severe pancreatitis secondary to multiorgan failure.
These multiple procedures may be secondary to multiple loculated collections or persistent infected collections or
slow liquefaction of the pancreatic necrosis and phlegmon
not amenable to catheter drainage. Vigilant follow-up,
including daily irrigation of pancreatic cavities with the
assessment of the patient's vital signs, WBC count, and
catheter drainage output is needed. Each catheter should
be irrigated with sterile saline solution at least once
daily. Abdominal CT should be performed periodically
on the basis of clinical status and amount of drainage
to check for residual and undrained fluid collections.
The CT findings help determine adequate drainage,
development of additional non-communicating collections
or complications.
Several interventional therapy regimens, including
endoscopic retrograde cholangiopancreatography
(ERCP) and sphincterotomy, fine needle aspiration for
bacteriology (FNAB), percutaneous or endoscopic drainage
of peripancreatic fluid collections, pseudocysts, and late abscesses, as well as selective angiography and catheterdirected
embolization of acute pancreatitis associated
bleeding complications have been well established as
diagnostic and therapeutic standards in the management
of acute pancreatitis. The risk of infection increases with
the extent of intrapancreatic and extrapancreatic necrosis
[17]. The mortality for sterile necrosis is low and can
usually be successfully treated by a conservative approach,
although surgery might be required for late complications
or persistent severe pancreatitis [20]. The mortality rate
for patients with infected pancreatic necrosis is higher
than 20%, and up to 80% of fatal outcomes in acute
pancreatitis are due to septic complications [21]. Freeny et
al. developed a technique of percutaneous drainage which
not only drained infected necrosis passively but included
necrosectomy by adding aggressive irrigation through
large bore percutaneous catheters (28 F) [15]. Some
centers described combined percutaneous retroperitoneal
necrosectomy, fragmentation of necrotic pancreatic and
peripancreatic tissue with a snare catheter and Dormia
baskets, continuous lavage of the cavity, and repeated
bronchoscopic visualization of the cavity to successfully
treat and avoid surgery in a patient [22]. In our patient
population large bore 20–32 F catheters were placed
under CT guidance, with a retroperitoneal approach from
the left side or the most accessible route. The necrotic
and solid material was fragmented and removed actively
with aspiration and irrigation of the cavity was performed
using up to 2-3 liters of normal saline solution per day
and additionally, manual aspiration of solid material was
performed on a daily basis till the time patients were in the
hospital (Figure 3). This helped in reducing the infected
material from the abdominal cavity and in reducing the
leucocytosis. Many times the catheters needed to be
replaced during irrigation procedures as large chunks of
infected fat necrosis would get occlude the catheters. The
replacement of the catheters was easy as these chronic
catheters had epithelized tracts which don't collapse easily.
Similar methods have been described in the literature.
Figure 3. Axial CT images showing pancreatic tail collection with large bore (28 Fr) catheter within it (Solid white arrow). Part of the Pigtail catheter (14
Fr) visualized in the anterior aspect of the collection (Hollow white arrow) used for irrigation purposes. Also visualized is the part of the nasojejunal tube
in the duodenum (Solid black arrow).
In patients with treatment failure with PCD, another
method of treatment is with double catheter lavage along
with percutaneous flexible endoscopic debridement which
may prevent surgical debridement [23]. Some researchers
suggested that endoscopic transmural drainage of walled
off necrosis with multiple stents to be safe and effective in
avoiding direct endoscopic necrosectomy [24, 25].
To our knowledge, our study is the largest reported to
date, to assess the clinical utility of CT-guided percutaneous
catheter drainage in patients with drainable symptomatic
pancreatic necrosis. Our study had few limitations,
including the retrospective nature, the variability of
experience among the interventional radiologists and
surgeons involved in the treatment of these patients. There
is a concern regarding the hospital stay of these patients
related to repeated procedures and subsequently an
increase in the length of hospital stay with the minimally
invasive procedures, however, we could manage most
patients on an outpatient basis. Once the drain output
reduces and sepsis is controlled, the patients were
discharged with the drainage catheter connected to stoma
bag for easy care at home. The patients were educated
about the drain care and monitoring the drain output on a
daily basis and advised to report to the emergency room if
the drain output falls abruptly (suggesting drain blockage)
or the collection becomes hemorrhagic or they develop
signs of sepsis. The patients were followed with regular
visits to the gastroenterology or interventional radiology
clinic. In the clinic the dedicated drain care team would
take care of dressing changes, suturing the dislodged
drain sutures and monitor the output (steadily decreasing
or increasing). We were able to manage 110 out of 126
patients on an outpatient basis with regular visits to the
clinic. No complication related to outpatient management
was reported.
CONCLUSION
Percutaneous catheter drainage is a safe and effective
technique for treating infected acute necrotizing pancreatitis. Appropriate selection of patients should
be performed to maximize the benefit of percutaneous
procedures. Treating necrotizing pancreatitis requires
dedicated multidisciplinary team efforts from the
physicians, surgeons, radiologist and the drain
management team. Many patients can be managed on
an outpatient basis reducing the hospital stay and the
healthcare cost. The patient, the referring physician, and
the radiologist must be ready to handle the number of
catheters, the catheter changes, multiple imaging scans,
and the duration of drainage.
Conflict of Interest
The authors have no conflicts of interests to declare.
References
- Banks PA, Freeman ML. Practice Parameters Committee of the
American College of Gastroenterology. Practice guidelines in acute
pancreatitis. Am J Gastroenterol 2006; 101:2379-2400. [PMID: 17032204]
- Pandol SJ, Saluja AK, Imrie CW, Panks PA. Acute pancreatitis: bench to
the bedside. Gastroenterology 2007; 132:1127 -1151. [PMID: 17383433]
- Thoeni RF. The Revised Atlanta Classification of Acute Pancreatitis:
Its Importance for the Radiologist and Its Effect on Treatment. Radiology
2012; 262:751-764. [PMID: 22357880]
- Bennett S, Lorenz JM. The role of imaging-guided percutaneous
procedures in the multidisciplinary approach to treatment of
pancreatic fluid collections. Semin Intervent Radiol 2012; 29:314-8.
[PMID: 24293805]
- Perez A, Whang EE, Brooks DC, Moore FD Jr, Hughes MD, Sica GT, et
al. Is severity of necrotizing pancreatitis increased in extended necrosis
and infected necrosis? Pancreas 2002; 25:229-233. [PMID: 12370532]
- Madenci AL, Michailidou M, Chiou G, Thabet A, Fernández-del Castillo
C, Fagenholz PJ. A contemporary series of patients undergoing open
debridement for necrotizing pancreatitis. Am J Surg 2014; 208:324-31.
[PMID: 24767969]
- Beger HG. Surgical management of necrotizing pancreatitis. Surg Clin
North Am 1989; 69:529–549. [PMID: 2658162]
- Baudin G, Chassang M, Gelsi E, Novellas S, Bernardin G, Hébuterne
X, et al. CT-guided percutaneous catheter drainage of acute infectious
necrotizing pancreatitis: assessment of effectiveness and safety. AJR Am J
Roentgenol 2012; 199:192-9. [PMID: 22733912]
- Chen HZ, Ji L, Li L, Wang G, Bai XW, Cheng CD, Sun B. Early prediction
of infected pancreatic necrosis secondary to necrotizing pancreatitis.
Medicine 2017; 96(30). [PMID: 28746189]
- Navalho M, Pires F, Duarte A, Goncalves A, Alexandrion P, Tavora
I. Percutaneous drainage of infected pancreatitic fluid collections in
critically ill patients: correlation with C-reactive protein values. Clin
Imaging 2006; 30:114 -119. [PMID: 16500542]
- Paye F, Rotman N, Radier C, Nouira R, Fagniez PL. Percutaneous
aspiration for bacteriological studies in patients with necrotizing
pancreatitis. Br J Surg 1998; 85:755–759. [PMID: 9667700]
- Werner J, Feuerbach S, Uhl W, Buchler MW. Management of acute
pancreatitis: from surgery to interventional intensive care. Gut 2005;
54:426–436. [PMID: 15710995]
- vanSonnenberg E, Wittich GR, Casola G, Brannigan TC, Karnel F,
Stabile BE, et al. Percutaneous drainage of infected and noninfected
pancreatic pseudocysts: experience in 101 cases. Radiology 1989;
170:757-761. [PMID: 2644662]
- D'Agostino HB, vanSonnenberg E, Sanchez RB, Goodacre BW,
Villaveiran RG, Lyche K, et al. Treatment of pancreatic pseudocysts with
percutaneous drainage and octreotide. Radiology1993; 187:685-688.
[PMID: 8497614]
- Beattie G, Hardman J, Redhead D, Siriwardena AK. Evidence for
central role of selective mesenteric angiography in the management
of the major vascular complications of pancreatitis. Am J Surg 2003;
185:96–102. [PMID: 12559436]
- Freeny PC, Hauptmann E, Althaus SJ, Traverso LW, Sinanan M.
Percutaneous CT-guided catheter drainage of infected acute necrotizing
pancreatitis: techniques and results. AJR Am J Roentgenol 1998; 170:969–
975. [PMID: 9530046]
- Walser EM, Nealon WH, Marroquin S, Raza S, Hernandez JA, Vasek
L. Sterile fluid collections in acute pancreatitis: catheter drainage versus
simple aspiration. Cardiovasc Intervent Radiol 2006; 29:102 -107. [PMID:
16283578]
- Segal D, Mortelé KJ, Banks PA, Silverman SG. Acute necrotizing
pancreatitis: role of CT-guided percutaneous catheter drainage. Abdom
Imaging 2007; 32:351 -361. [PMID: 17502982]
- Jain S, Mahapatra SJ, Gupta S, Garg PK. Infected Pancreatic Necrosis
due to Multidrug-Resistant Organisms and Persistent Organ failure
Predict Mortality in Acute Pancreatitis. Clin Transl Gastroenterol 2018;
9:190. [PMID: 30287818]
- Connor S, Ghaneh P, Raraty M, Sutton R, Rosso E, Garvey CJ, et al.
Minimally invasive retroperitoneal pancreatic necrosectomy. Dig Surg
2003; 20:270–7. [PMID: 12748429]
- Buchler MW, Gloor B, Müller CA, Friess H, Seiler CA, Uhl W. Acute
necrotizing pancreatitis: treatment strategy according to the status of
infection. Ann Surg 2000; 232:619–26. [PMID: 11066131]
- Gloor B, Müller C, Worni M, et al. Late mortality in patients with
severe acute pancreatitis. Br J Surg 2001; 88:975–9. [PMID: 11442530]
- Gmeinwieser J, Holstege A, Zirngibl H, Palitzsch KD, Hügl S, Strotzer
M, et al. Successful percutaneous treatment of infected necrosis of the
body of the pancreas associated with segmental disruption of the main
pancreatic duct. Gastrointest Endosc 2000; 52:413–15. [PMID: 10968863]
- Liu P, Song J, Ke HJ, Lv NH, Zhu Y, Zeng H, et al. Double-catheter
lavage combined with percutaneous flexible endoscopic debridement for
infected pancreatic necrosis failed to percutaneous catheter drainage.
BMC Gastroenterol 2017; 17:155. [PMID: 29221438]
- Rana SS, Sharma V, Sharma R, Gupta R, Bhasin DK. Endoscopic
ultrasound guided transmural drainage of walled off pancreatic necrosis
using a “step-up” approach: A single centre experience. Pancreatology
2017; 17:203-8. [PMID: 28202234]




