Keywords
Economics; Mortality; Pancreas; Pancreaticoduodenectomy; Perioperative Care; Rehabilitation
INTRODUCTION
Since Whipple et al. popularised pancreaticoduodenectomy in 1935 [1], pancreatic resections are increasingly being performed for treatment of pancreatic tumours, especially during the last two decades [2]. In the United Kingdom, the annual number of pancreaticoduodenectomies has increased by 71% during the last 7 years [3]. Peri-operative morbidity and mortality rates are improving with increasing experience in large-volume tertiary centres [4]. Recently, however, parameters such as duration of hospital stay and length of patient recovery appear to attract increasing attention from both patients and health care providers, altering the standards and targets. “Enhanced recovery” or “fast-track” programmes have been introduced in the field of peri-operative care, representing multi-modal strategies that provide for optimal pain relief, stress reduction with regional anaesthesia, early enteral nutrition and patient mobilisation [5]. These regimes aim to restore the functional capacity of surgical patients to their premorbid state faster and more effectively than the conventional peri-operative approaches and their favourable effect has already been demonstrated in colorectal cancer surgery [6, 7]. In pancreatic surgery, the duration of hospital stay depends on post-operative surgical complications such as pancreatic leaks, intraabdominal collections, haemorrhage, delayed gastric emptying and general medical complications involving the cardiopulmonary systems. Therefore, peri-operative interventions aiming to minimise the above adverse events could potentially expedite patient recovery and improve outcomes.
Aims and Methods
This review aims to present the evidence underpinning the use of multi-modal fast-track pathways in pancreatic cancer surgery. Key elements of these protocols are presented, evaluating their feasibility, safety and efficacy in accelerating patient recovery. Bibliographic search in the MEDLINE®, (https://www. ncbi.nlm.nih.gov/pubmed/) EMBASE®, (https://www.embase.com/) CINAHL® (https://www.ebscohost.com/cinahl/) databases and the Cochrane Collaboration Library (https://www. cochrane.org/)was performed to retrieve all relevant publications in English language to date. The terms “clinical pathway”, “fast track”, “enhanced recovery”, “peri-operative”, “pancreas” and their derivatives such as “pancreatic”, “pancreaticoduodenectomy”, “Whipple’s”, “resection”, “surgery” and synonyms were used in various combinations. Backward referencing by manual search of bibliography was also performed to increase the yield of papers. Studies were included if they involved clinical pathways used in a hospital setting to facilitate the care of adults undergoing elective surgery for pancreatic malignancy. Studies with sufficient description of the content of the clinical pathway and reporting clinically relevant outcome measures, such as length of hospital stay, complication rate, 30-day re-admission rate and 30-day mortality rate, were included. Studies were excluded if they described single interventions in one parameter of perioperative care rather than a bundle of measures that constitute the “fast-track” or “enhanced recovery” programmes; the evidence that established each individual element as part of the pathway lies beyond the aim of this review.
Results
Enhanced-recovery programmes have only recently been introduced in gastrointestinal cancer surgery; hence the available evidence related to pancreatic
resections is limited. A total of six publications were retrieved during our search [8, 9, 10, 11, 12, 13], three of which were excluded from this analysis, because they did not provide sufficient details of the clinical pathway components [8, 9], or were concerned only with isolated elements of peri-operative care [10]. Three retrospective case-series satisfied the inclusion criteria, two of which had comparisons with historical controls.
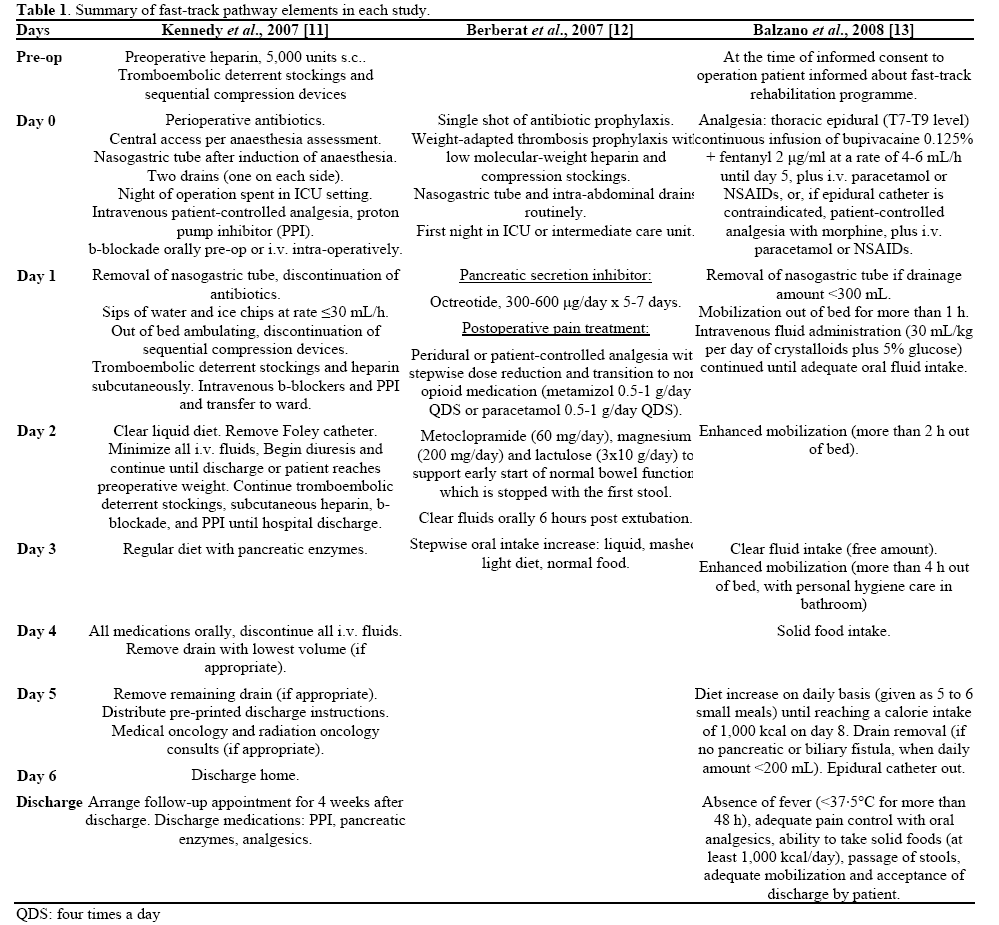
Kennedy et al. [11] retrospectively reviewed the outcomes of 135 consecutive pancreaticoduodenectomies, classified in two groups; a “post-pathway group” of 91 patients, who underwent pancreaticoduodenectomy after implementation of a clinical pathway (Table 1), compared to a “pre-pathway” group of 44 patients. Both groups were similar regarding demographic data (age, gender and race) and underlying pathology (percentage of malignant cases). During the postpathway period higher volume of operations was undertaken (mean 7.6 cases/month) comparing to the previous period (2 cases/month), which reflected a centralization of pancreatic services in this hospital. Significantly shorter operation times (mean±SE, 379±12 min vs. 435±14 min for the pre-pathway patients, P<0.0001) and pre-procedure anaesthetic times (76±2 min vs. 95±4 min of the pre-pathway patients, P<0.0001), were noted during the same postpathway period.
There was no significant difference in the overall perioperative complication rate before (44%) and after (37%) implementation of the pathway. Similar rates were noted between pre-pathway and post-pathway groups with regard to the incidence of pancreatic fistula (9% versus 2%, respectively), delayed gastric emptying (7% versus 8%, respectively), wound infection (9% versus 13%, respectively) and less common complications, such as cardiovascular events, pneumonia, intra-abdominal abscesses requiring drainage, small bowel obstruction and deep venous thrombosis (total morbidity rates: 25% versus 20%, respectively). There was a significant decrease in the post-operative length of hospital stay in the postpathway group (median 7 days) compared to the prepathway cohort (13 days, P<0.0001), with a parallel reduction in total hospital charges (mean±SE, $240,242±32,490 for the pre-pathway patients vs. $126,566±4,883 for post-pathway patients, P<0.0001). This decrease length of hospital stay did not come at the expense of higher 30-day re-admission rate (7.0% for pre-pathway patients and 7.7% for post-pathway ones).
In a retrospective review of 283 consecutive pancreatic resections, Berberat et al. [12] implemented the enhanced recovery pathway outlined in Table 1. Two thirds of the pancreatic resections were performed for pancreatic tumours and the remaining for benign diseases. The overall median operating time was 5 h and 45 min (range: 73 min to 10 h and 43 min). Median blood loss was 700 mL (range: 50-5,500 mL) and 26% of the patients needed blood transfusion therapy. A total 69% of patients were transferred to ICU with median stay of 1 day (range: 1-32 days), whereas 31% of patients were directly transferred from the recovery room to an intermediate care unit or even to the ward (22.4% and 8.4%, respectively). Overall, patients returned to the ward after a median of 2 days (range: 0- 38 days). The mean hospital stay was 10 days (range: 4-115 days) and the 30-day readmission rate was 3.5%. Nasogastric tubes were removed from most patients immediately after the end of the operation (80.4%) or during the first postoperative day (13.3%) but 11.4% needed re-insertion of the nasogastric tube later, with a median interval to reinsertion of 6 days (range: 1-13 days). Resumption of clear oral fluid intake was possible on day 1 (median: 1 day; range: 0-6 days) and of normal food on median day 5 (range: 1-24 days). The intra-abdominal drains were removed on median day 3 (range: 0-19 days). The bladder catheter was removed on median day 5 (range: 1-49 days). Finally, the central venous line was removed on median day 6 (range: 1-49 days). Gastrokinetic drugs did not expedite bowel movement and, in fact, use of metaclopramide was associated with delayed patient discharge (P<0.05). First mobilization (out of the bed) was achieved on median day 1 (range: 0-9 days), and on median day 3 (range: 1-46 days) patients were fully mobile.
A 30-day mortality rate of 2% was noted, caused by pancreatico-jejunostomy leak (n=2), pancreatic stump leak after distal pancreatectomy (n=1), jejuno-jejunal anastomotic failure (n=1), and unexplained sepsis with multi-organ failure in one case. Surgical morbidity mounted to 24.7%, caused by delayed gastric empting (7.8%), postoperative haemorrhage (7.5%), pancreatic fistulae (4.7%), and wound infection (4.7%). Overall, 9% of patients received a re-laparotomy. Multivariate analysis identified that significant independent factors of early successful discharge were age less than 60 years (odds ratio: 4.06; P<0.001), short operating time less than 6 hours (odds ratio: 1.99; P<0.05), and early extubation (odds ratio: 2.8; P<0.05).
Recently, Balzano et al. [13] evaluated the impact of a fast-track protocol (Table 1) of peri-operative care in the recovery of 252 consecutive patients undergoing pancreaticoduodenectomy (fast-track group), who were compared to an equal-sized historical control group of patients operated before the implementation of the pathway (control group). The two groups were adequately matched for demographic data and underlying disease. Analysis of post-operative outcomes showed that in the fast-track group, successful removal of nasogastric tube was achieved in 95.6% of patients by day 3, although it was reinserted in 15% of patients because of either vomiting or relaparotomy. All patients without a nasogastric tube commenced liquid intake on day 3 and oral food on day 4, although most patients failed to achieve the planned daily dietary calorie intake (1,000 kcal) during the first 8 days because of symptoms of food intolerance. There was no difference between the two groups regarding interval to first flatus (median day 3), but the first passage of stools occurred earlier in fasttrack patients than in the control group (median 5 versus 6 days, respectively; P<0.001). There was no difference in the overall peri-operative mortality rate (3.6% for the fast-track group versus 2.8% for the control), the incidence of pancreatic fistula or any other intra-abdominal complication. The patients in the fasttrack group had significantly lower incidence of delayed gastric emptying (3.9% versus 24.6% of the traditional group; P=0.004). The length of postoperative hospital stay was shorter in the fast-track group (median 13 days; range: 7-102 days) compared to control (median 15 days; range: 7-110 days; P<0.001). There was no significant difference in readmission rates, with 7.1% for fast-track patients and 6.3% for patients in the control group.
Discussion
Gastrointestinal cancer surgery involves major complex procedures requiring high level of surgical and peri-operative care and is associated with high morbidity and long hospital stay. The beneficial effect of implementation of multi-modal peri-operative pathways on outcomes of colorectal surgery (the Protocol of Enhanced Recovery After Surgery in Colorectal Surgery; ERAS protocol, https://clinicaltrials. gov/ct2/show/NCT00498290) has, expectedly, raised interest in other subspecialties of surgical oncology for potentially wider application [7]. Improved outcomes regarding length of patient hospital stay have also stimulated interest and support by health care providers because they could translate into financial benefits. Systematic review of the literature regarding perioperative care in pancreatic cancer surgery revealed a limited number of studies bearing low levels of evidence. Retrospective case-series and comparative case-control studies (“before-after”) using historical controls have only been retrieved knowing well the inherent disadvantages of comparing patient outcomes across different time periods. It is generally accepted that implementation of such multi-modal pathways constitutes complex interventions that cannot be easily studied in the context of randomised controlled trials, because of weaknesses in developing, identifying, documenting, and reproducing the intervention [14]. The studies analysed in this review were not devoid of such problems. In the study of Kennedy et al. [11] the introduction of a fast-track protocol coincided with the appointment of two new surgeons with interest in pancreatic surgery and bigger operation volume; these facts could have independently contributed to improved recovery outcomes. Their group of patients, as well as those studied by Berberat et al. [12], were highly heterogeneous with regards to age and contained a case-mix of Whipple’s and distal pancreatectomies, performed for both benign and malignant diseases, parameters that are proved to be independent determinants of outcome. Patient selection bias may also have been a potential weakness for the above comparative studies [11, 13], with allocation of healthier patients in the fast-track pathway groups, thus giving unfair advantage over the unfiltered controls.
Despite their potential weaknesses, the above studies have demonstrated that implementation of fast-track peri-operative care pathways is feasible in pancreatic surgery and can be associated with reduced length of stay, lower relevant hospital costs and no increase in morbidity, 30-day mortality or re-admission rates (Table 2). Balzano et al. [13] attributed the improved outcomes of the fast-track group to the initiation of early oral feeding, which resulted in lower incidence of delayed gastric emptying and earlier bowel activity in this group, compared to the traditional approach. Interestingly though, the noted reduction in length of hospital stay and related costs by Kennedy et al. [11] was not associated with proportionate decrease in the incidence of complications or mortality. It is therefore questionable whether the noted benefits resulted from improvements in physiological factors related to patient recovery or potentially from a more efficient discharge policy. It is also possible that patient, nurse, and physician participation in the clinical pathways may have influenced costs and outcomes independent of any intervention within the clinical pathway itself. Such a phenomenon, analogous to the placebo-effect observed in randomized clinical trials, termed as the “Hawthorne effect” [15] could still be considered as a benefit related to the use of fast-track pathways.

An area of potential concern was the high incidence of re-laparotomy noted in patients of the fast-track groups of around 9% [12, 13]. With the exception of Balzano et al.’s study (7.9%) [13], the rate of reoperation in these groups was significantly higher than relaparotomy rates reported in large series of pancreatic resections, ranging between 2.0% and 2.7% [2, 8, 9]. Aetiological analysis showed that in 60% of relaparotomies the indication was intra-abdominal haemorrhage, which was unlikely to be caused by implementation of fast-track pathway, and in 40% of cases the cause was pancreatic leak not amenable to radiological drainage [12]. This parameter warrants specific attention and should be a major end-point in future studies.
In summary, our systematic review concludes that the evidence underpinning the use of fast-track clinical pathways in the peri-operative care of patients undergoing pancreatic resection is limited. The preliminary results of a small number of retrospective studies have shown that the implementation of a fasttrack multi-modal peri-operative pathway is feasible and can achieve shorter length of hospital stay and reduced relevant costs, with no increase in readmission and mortality rates. The studies provide conflicting evidence on the physiological mechanisms that result in accelerated patient recovery and raise certain safety issues with regards to post-operative morbidity, which would require rigorous evaluation in the context of further, large-size, prospective randomised-controlled trials.
Acknowledgements
This review was undertaken as part of a thesis submitted towards the first author’s MSc degree. (MSc in Peri-Operative Care and Advanced Surgical Practice, Cardiff University)
Conflicts of interest None
References
- Whipple AO, Parsons WB, Mullins CR. Treatment of carcinoma of the ampulla of Vater. Ann Surg 1935; 102:763-79. [PMID 17856666]
- Cameron JL, Riall TS, Coleman J, Belcher KA. One thousand consecutive pancreaticoduodenectomies. Ann Surg 2006; 244:10-5. [PMID 16794383]
- Ypsilantis E, Courtney ED, Warren H. Increase in annual number of pancreatic head resections does not affect mortality of pancreatic cancer in the United Kingdom. JOP. J Pancreas (Online) 2009; 10:462-3. [PMID 19581759]
- Gouma DJ, van Geenen RC, van Gulik TM, et al. Rates of complications and death after pancreaticoduodenectomy: risk factors and the impact of hospital volume. Ann Surg 2000; 232:786-95. [PMID 11088073]
- Fearon KC, Ljungqvist O, Von Meyenfeldt M, Revhaug A, Dejong CH, Lassen K, et al. Enhanced recovery after surgery: a consensus review of clinical care for patients undergoing colonic resection. ClinNutr 2005; 24:466-77. [PMID 15896435]
- Khoo CK, Vickery CJ, Forsyth N, et al. A prospective randomized controlled trial of multimodal perioperative management protocol in patients undergoing elective colorectal resection for cancer. Ann Surg 2007; 245:867-72. [PMID 17522511]
- Wind J, Polle SW, Fung Kon Jin PH, Dejong CH, von Meyenfeldt MF, Ubbink DT, et al. Systematic review of enhanced recovery programmes in colonic surgery. Br J Surg 2006; 93:800-9. [PMID 16775831]
- Balcom JH 4th, Rattner DW, Warshaw AL, Chang Y, Fernandez-del Castillo C. (2001). Ten-year experience with 733 pancreatic resections: changing indications, older patients, and decreasing length of hospitalization. Arch Surg 2001; 136:391-8. [PMID 11296108]
- Porter GA, Pisters PW, Mansyur C, et al. Cost and utilization impact of a clinical pathway for patients undergoing pancreaticoduodenectomy. Ann SurgOncol 2000; 7:484-9. [PMID 10947015]
- Akizuki E, Kimura Y, Nobuoka T, Imamura M, Nagayama M, Sonoda T, Hirata K. Reconsideration of postoperative oral intake tolerance after pancreaticoduodenectomy: prospective consecutive analysis of delayed gastric emptying according to the ISGPS definition and the amount of dietary intake. Ann Surg 2009; 249:986- 94. [PMID 19474680]
- Kennedy EP, Rosato EL, Sauter PK, Rosenberg LM, Doria C, Marino IR, et al. Initiation of a critical pathway for pancreaticoduodenectomy at an academic institution--the first step in multidisciplinary team building. J Am CollSurg 2007; 204:917-23. [PMID 17481510]
- Berberat PO, Ingold H, Gulbinas A, Kleeff J, Müller MW, Gutt C, et al. Fast track- different implications in pancreatic surgery. J GastrointestSurg 2007; 11:880-7. [PMID 17440787]
- Balzano G, Zerbi A, Braga M, Rocchetti S, Beneduce A, Di Carlo V. Fast-track recovery programme after pancreaticoduodenectomy reduces delayed gastric emptying. Br J Surg 2008; 95:1387-93. [PMID 18844251]
- Campbell M, Fitzpatrick R, Haines A, Kinmonth AL, Sandercock P, Spiegelhalter D, Tyrer P. Framework for design and evaluation of complex interventions to improve health. BMJ 2000; 321:694-6. [PMID 10987780]
- Becker EL, Landau SI, eds. International Dictionary of Medicine and Biology. Vol.1. New York: Wiley Medical Publications, 1986:905.

