Keywords
audiology, direct referral, ENT, general practitioner, hearing aid, wax
How this fits in with quality in primary care
What do we know?
Direct referral audiology clinics were introduced for the assessment and provision of hearing aids in those over 60 years of age to reduce outpatient waiting times and demand on ENT appointments.
What does this paper add?
Direct referral audiology clinics appear to continue to provide a cost-benefit to the NHS, reducing demand on ENT appointments.
Introduction
In England and Wales it is estimated that 2.8 million people have a hearing impairment causing a degree of disability appropriate for referral and assessment for a hearing aid.[1–2] With increasing age patients are less likely to acknowledge their hearing loss, resulting in a substantial delay in seeking medical attention and hence treatment.[3] GPs rarely identify hearing loss opportunistically,[4] making patients’ recognition of the problem key to appropriate referral and treatment. Hearing loss in people over the age of 60 years is treatable in most cases.[5] Currently in England and Wales 3.4% of the adult population have been provided with hearing aids, but a further7%might benefit from an aid and demand will continue to rise as the population ages.[1]
Direct referral audiology clinics (DRACs) for the assessment and provision of hearing aids in those over 60 years of age were initially introduced as a method to decrease outpatient waiting times and reduce ENT appointments.[2] With the introduction of theNHS 18- week waiting targets (no patient should wait for more than 18 weeks from the point of referral to the start of treatment) this may no longer be the case. The DRAC at the Norfolk and Norwich University Hospital provides hearing aids following investigation with pure tone audiogram and completion of the Glasgow Hearing Aid Benefit Profile.[6] Referral to DRAC is via a patient’s GP, using criteria based on those specified by the liaison group for Technicians, Therapists and Scientists in Audiology (TTSA) in 1988.[7] All patients meeting these criteria should be over the age of 60 years, have long-standing hearing loss (roughly equal in both ears) and have no associated vertigo, otalgia or unilateral tinnitus (Box 1). This screening tool effectively identifies those patients in whom underlying pathology may be the cause for their hearing loss, and for whom investigation is warranted. Additional written information is provided to GPs on alternative referral pathways, directing those patients failing to meet DRAC criteria to ENT in the first instance. A patient pathway is demonstrated in Figure 1. Formal audiological screening tests in the community are not required for DRAC. Referrals not meeting the age criteria or patients already using an NHS hearing aid are redirected at the point of referral to alternative ENT or audiology clinics. The audiology and ENT departments are located adjacent to one another, with close communication. Where audiologists are concerned about underlying pathology they can discuss the patient with an ENT specialist, refer directly to ENT or refer back to the patient’s GP. Waiting times at the time of the study were 11 weeks from referral to fitting of a hearing aid and five weeks for a new patient ENT appointment.
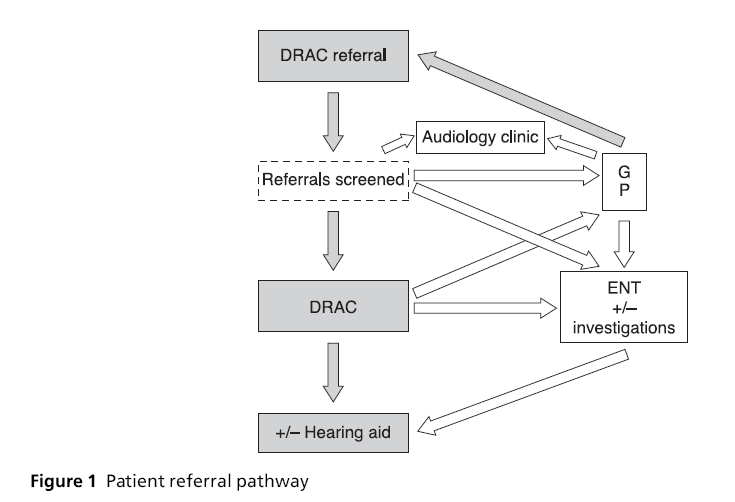
Figure 1: Patient referral pathway
The aim of this study was to review direct GP referrals based upon the DRAC criteria to determine the benefits of continuing a DRAC referral system.
Materials and methods
The electronic data (AuditBase©) of all patients attending the DRAC over a four-month period were reviewed. AuditBase© contains both audiological data and free text entries by audiologists on the appropriateness of DRAC referral and any subsequent intervention required by the patient. Patient administrative records were not studied.
Using the electronic audiogram records, the hearing loss at 2 kHz and 4 kHz were obtained and the mean value of these readings calculated. Whilst arbitrary, a mean hearing loss obtained via this method of ≥ 40 dB was deemed a significant level to gain benefit from a hearing aid; this was a level already in use in the department, albeit with further assessment and determination of patient demands. In addition to the audiogram, the number of patients with asymmetrical hearing loss, excessive wax, vertigo and tinnitus, plus those referred to ENT, were reviewed to determine those patients failing to meet the referral criteria.
Costs were calculated using the NHS (2007–2008) tariffs from the Department of Health. Would a saving of £63 per patient attending a DRAC appointment (£50) rather than a new patient ENT appointment (£113) indicate a significant cost-benefit or a false economy?
Results
Over the four-month study period 353 patients attended DRAC (178 females, 175 males) with a mean age of 77� 8.6 years (range 60–96 years).
The mean hearing loss at 2 kHz was 47�17 dB and at 4 kHz 64�17 dB. The hearing loss at 2 kHz and 4 kHz were combined to produce a mean value for each ear. The mean hearing loss for the right ear was 55�15 dB (range 15–105) and 56�16 dB for the left (range 13–120).
Of the 353 patients referred to DRAC (Figure 2), 91% (n=320) ultimately were offered and accepted a hearing aid (right sided n=123; left sided n=92; bilateral aids n=105). For the remaining 9% (n=33) not receiving an aid, 18 patients were offered but declined an aid and 15 patients had a hearing loss which was not significant enough to warrant aiding.
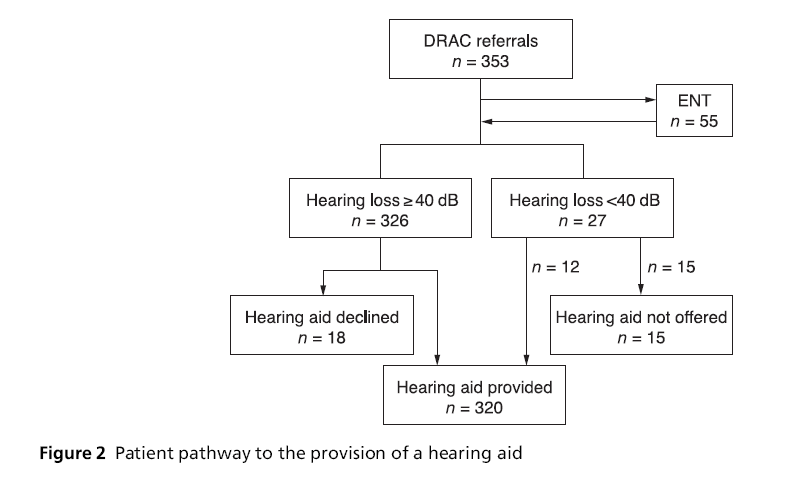
Figure 2: Patient pathway to the provision of a hearing aid
Using a threshold of 40 dB as evidence of potential benefit from aiding, 8% (n=27) of patients had a hearing loss below this level, and the potential benefit of an aid was debatable. Despite this, 12 of these patients were provided with at least one aid (left sided n=6; right sided n=5; bilateral n=1).
Asymmetrical hearing loss, defined as a discrepancy of 20 dB in the mean hearing loss (2 kHz and 4 kHz) between ears, was identified in 9% of patients (n=33). Of these, 19 patients were referred for ENT opinion, with the remaining patients being already known to ENT, with unchanged audiograms.
In total, 10% (n=36) of patients were noted to have significant wax, which impacted upon their management. After microsuctioning, three patients had a hearing loss of below the 40 dB threshold. The remaining 33 patients were suitable for aiding, but two patients experienced such marked improvement in their hearing that they declined an aid. The identification and management of wax in the community for these five patients, would have resulted in a cost saving of £250, based upon a DRAC referral cost of £50 per new patient.
A further 10% (n=36) of patients required ENT opinion (Figure 3), excluding those seen simply for microsuctioning of wax. Of these, 14 were for conductive hearing loss, five for tinnitus, four for vertigo, six for otalgia, two for otitis externa, two for auditory canal pathology, two for tympanic perforation and one because of co-existing mental health problems requiring assistance with assessment. Despite referral to ENT, all but five of these patients subsequently went on to be aided.
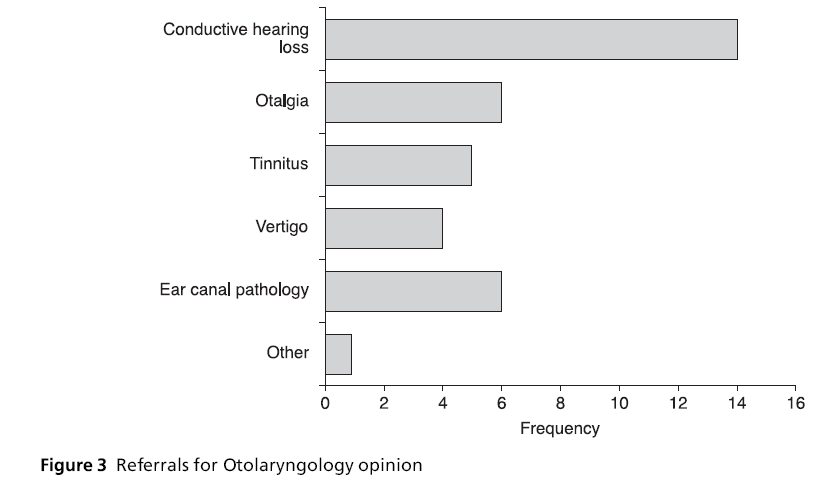
Figure 3: Referrals for Otolaryngology opinion
Despite attendance atDRAC,5%(n=18) of patients did not want a hearing aid, despite seven of these having significant hearing loss. It is unclear why these patients were referred.
With reference to the DRAC referral guidelines, it is apparent that 51 patients (14%) fell short of the defined criteria, when consideration is given to the lack of information regarding patients’ initial complaint to their GP or their perception of whether their hearing loss was bilaterally equal. Had criteria three, four and five (Box 1) been included within the study, a higher percentage is likely, particularly in view of the large number of patients identified as having asymmetrical hearing loss. Since referrals are screened at the point of receipt in the department, there were no patients outside of the defined age range, or already using an NHS hearing aid.
In total, the estimated cost for appointments and hearing aid provision for our cohort of patients was £63 430. The key areas for cost saving that could be implemented in the community include the identification and management of wax, questioning of patients regarding their willingness to accept an aid if offered and referral to ENT rather than DRAC in cases where patients have co-existing symptomatology.
Discussion
Of the patients referred to DRAC, 92% had a mean hearing loss of �40 dB (10% unilaterally) and would be deemed likely to gain significant benefit from a hearing aid. Our referring GPs do not currently use any formal audiological screening equipment and its introduction into the community would not result in significant benefit, reflecting the accuracy of GPs referring those with significant hearing loss. Yet this high accuracy of referrals inevitably means that there are a number of patients who are not referred for specialist opinion.We are unable to comment on those patients that attend their GP complaining of hearing loss but are not referred for audiological assessment.
Watson[8] concluded that the main cause of delay in treating impaired hearing is failure by patients to seek help promptly. Keay[9] found the mean duration of hearing difficulty was 3.1 years; other studies have found that this can be up to 15 years.[10,11] With significant delays in patients seeking medical attention, GPs are seeing only a small percentage of those patients who may benefit from the provision of a hearing aid.
Both Sindhusake et al[12] and Torre et al[13] found that the single question ‘Do you feel you have hearing loss?’ was sufficient to provide reasonable sensitivity and specificity. Patients presenting to their GP with hearing loss will therefore have self-selected themselves with high accuracy, both in their detection of their decreased hearing and with the significant delay between the onset of hearing loss and presentation.
In total, 91% of all patients referred to DRAC were subsequently provided with at least one hearing aid. It is likely that the pro forma(referral guideline) is highly selective for identifying the hearing aid priority group. GPs are provided with written guidance on the pro forma, defining the referral criteria and the appropriate alternative pathways for patients not meeting the criteria.
In 2009, the British Academy of Audiology[14] issued revised guidelines for referral to DRACs, adjusting the age criteria to include all patients over the age of 16 years. At our Trust we have recently reduced the lower age for referrals to 50 years, since the numbers of patients below 50 years without causative pathology for hearing loss in our patient population is particularly small. The initial screening of referrals to ensure patients meet with the age restrictions for referral to DRAC appear effective, with no patients identified in the study group below our initial criteria of 60 years.
Patients referred by their GP are highly likely to both require and take up a hearing aid when it is offered to them, since their hearing loss has become significant enough to prompt them to seek medical advice. Patients meeting the criterion for a hearing aid may decline an aid for many reasons: 5% of our study population did so, at a cost of £900 wasted DRAC appointments, but we did not take into account those patients who subsequently returned to the audiology department at a later date for a hearing aid. These patients may have simply been reassured that there was no sinister pathology as the cause of their hearing loss, or initially may have believed that alternative treatments to an aid were available.
Sixteen percent of patients were referred to the ENT department, most commonly due to asymmetrical audiograms which may not be detectable by clinical examination in a general practice setting. Ten percent of patients had excessive wax at the time they were seen in audiology. Two patients felt significant improvement in their hearing after microsuctioning and therefore declined an aid despite meeting the audiogram criteria, and four patients did not meet the criteria for a hearing aid after wax removal. These patients should have been identified and treated initially by their GPs.
Failure to take a thorough history and perform an otological examination resulted in a further 36 patients (10%) requiring ENT referral or return to their GP because of unilateral tinnitus, otalgia, vertigo, otitis externa, tympanic perforation or conductive hearing loss. In some cases of conductive hearing loss, there was additionally a sensorineural component to the loss which may have been difficult to interpret on Rinne’s and Weber’s tests in the community. Despite this, most of these patients after ENT review with or without investigation were subsequently fitted with a hearing aid.
Excluding the 55 patients requiring an ENT appointment, had the remainder of our patients been seen in an ENT clinic rather than a DRAC there would have been an additional cost of £18 774 for these 298 patients. Considering the small number of patients referred inappropriately to DRAC, the cost benefits of the clinic are immense.
Further improvements could be implemented in primary care, including greater attention to otoscopy (to remove wax and identify external ear disease and tympanic membrane perforation) and to the history (to identify tinnitus vertigo and otalgia).
The final decision for the provision of a hearing aid is multifactorial, with consideration of the patients’ perceptions and difficulties in addition to their audiogram results. Overriding patient demands are demonstrated where those failing to meet the audiogram criterion are nevertheless provided with a hearing aid. At a cost of £69 per hearing aid device, aiding needs to be of significant benefit to the patient. We are unable to comment on the number of patients who continued to use their aids despite having a hearing loss of below 40 dB. Smeeth et al[15] concluded that many people who own an aid do not use it regularly, and it is anticipated that where hearing improvement is minimal compliance will be significantly reduced.
Conclusion
Direct GP referral for the provision of hearing aids provides a suitable and timely assessment and hearing aid provision for the majority of patients.Most patients referred have a hearing loss suitable for aiding. Further attention within primary care to clearing wax and excluding patients with contraindications could decrease inappropriate referrals. Whilst DRACs were initially introduced to reduce ENT waiting times, with the introduction of NHS targets on outpatient clinics this is no longer the case, and 16% of patients encountered delay in obtaining diagnosis, with or without provision of an aid, by the need for ENT referral. Compared to the costing for anENToutpatient appointment DRAC provides a significant cost benefit for the NHS.
Acknowledgement
The authors wish to thank Mr Paul Q Montgomery, Consultant ENT Surgeon, Norfolk and Norwich University Hospital for his help with this project.
References
- National Institute for Health and Clinical Excellence. NHS Guidance on Hearing Aid Technology. London: NICE, 2000.
- Fox GC and Sharp JF. Direct hearing aid referral: the effect upon outpatient waiting times in a district general hospital. Journal of the Royal Society of Medicine 1994; 87:215–16.
- Merluzzi F and Hinchcliffe R. Threshold of subjective audiology handicap. Audiology 1973;12:65–9.
- Schneider JM, Gopinath B, McMahon CM et al. Role of general practitioners in managing age-related hearing loss. Medical Journal of Australia 2010;192:20–3.
- Sprinzl GM and Richelmann H. Current trends in treating hearing loss in elderly people: a review of the technology and treatment options – a mini-review. Gerontology 2010;56(3):351–8.
- Gatehouse S. The Glasgow Hearing Aid Benefit Profile: what it measures and how to use it. The Hearing Journal 2000;53:10–18.
- Bamford J. TTSA: guidelines for hearing aid direct referral. British Association of Audiological Scientists’ Newsletter 1988;13:16–17.
- Watson C and Crowther JA. Provision of hearing aids: does specialist assessment cause delay? BMJ 1989;299: 437–9.
- Keay DG. Referrals to a hearing aid clinic: scope for improvement. British Journal of General Practice 1990; 40:62–3.
- Wu HY, Chin JJ and Tong HMH. Screening for hearing impairment in a cohort of elderly patients attending a hospital geriatric medicine service. Singapore Medical Journal 2004;45:79–84.
- Stephens SD, Callaghan DE, Hogan S, Meredith R, Rayment A and Davis AC. Hearing disability in people aged 50–65: effectiveness and acceptability of rehabilitative intervention. BMJ 1990;300:508–11.
- Sindhusake D, Mitchell P, Smith W et al. Validation of self-reported hearing loss. The Blue Mountains Hearing Study. International Journal of Epidemiology 2001;30: 1371–8.
- Torre P, Moyer CJ and Haro NR. The accuracy of selfreported hearing loss in older Latino-American adults. International Journal of Audiology 2006;45:559–62.
- British Academy of Audiology. Guidelines for referral to audiology of adults with hearing difficulty. 2009. theloop.netplan.co.uk/~admin9/index.php?option= com_contentandtask=viewandid=312andItemid= 155
- Smeeth L, Fletcher AE, Ng E S-W et al. Reduced hearing, ownership, and use of hearing aids in elderly people in the UK – the MRC Trial of the Assessment and Management of Older People in the Community: a crosssectional survey. The Lancet 2002;359:1466–70.
Peer Review
Not commissioned; externally peer reviewed.
Conflicts of Interest
None.

