Keywords
Coronary artery bypass graft; Syntax score; Hybrid revascularization
Abbreviations
CABG: Coronary Artery Bypass Graft; DVQ: Distal Vessel Quality; IQR: Inter Quartilic Range; LAD: Left Anterior Descending; LIMA: Left Internal Mammary Artery; QCA: Quantitative Coronary Analysis; SD: Standard Deviation; SVG: Saphenous Vein Graft
Introduction
Prevalence of multi-vessel coronary artery disease is high, affecting between 41% and 67% of the patients with coronary stenosis [1,2]. In USA more than half of these cases are treated with coronary artery bypass grafting (CABG) procedures [1]. It has been well demonstrated that the use of the left internal mammary artery (LIMA) to graft the left anterior descending (LAD) artery has significant benefits compared to saphenous vein grafts (SVG) [3,4]. Nevertheless, as a whole, SVG are still the most frequently type of graft used during CABG. Several studies have evaluated the patency of SVG in short and long-term follow-up, reporting up to 13% occlusion rate at 1-year [5,6], and over 20% at fiveyear (6). Clinical and anatomical predictors of graft occlusion after CABG include lipoprotein levels, and burden of atherosclerotic disease in SVG [7-9]. Also, quality and diameter of the target vessel have been previously associated with rate of occlusion or dysfunction of arterial and vein grafts [10]. Although Syntax score represents a useful tool to determine the best strategy [11], it is mainly focused on criteria that underscore percutaneous intervention (as tortuosity or presence of bifurcations) and not in specific anatomical predictors of durability of bypass grafts.
Heart team consensus based on several risk models has become the recommended approach for the decision making process but no risk score alone can be used to guide the appropriate strategy of revascularization [12]. In the evidence-based era, subjective factors seem to weight still too much when balancing the pros and cons of coronary revascularization surgery in individual patients. Specially, if we take into consideration the growing range of alternatives in this field (i.e. hybrid interventions, percutaneous treatment of chronic total coronary occlusions, external stenting of SVG, etc).
Therefore, we aimed to develop a new angiographic score that may allow predicting early- and mid-term patency troubles of coronary bypass grafts as a new tool for the decision making process in the field of coronary revascularization.
Methods
A total of 254 consecutive patients who underwent CABG, with previous coronary angiography, were retrospectively included and a mean follow-up of 6-years was obtained. Five patients were excluded from the analysis due to low-quality angiographic records precluding from correct analysis (incomplete/limited angiographic exam with one or more vessel/graft not injected selectively), leading to a final study population of 249 patients.
Angiographic evaluation and score calculation
Angiographic images were analyzed at baseline and at the time of any clinical event requiring angiographic evaluation at follow up. All significant stenosis were described and classified as moderate (50 to 70%), severe (70-99%), or occlusion (100%), and vessel diameters were determined through quantitative coronary analysis (QCA) in an independent core lab (www.icicorelab.es). Also, Syntax score was determined as previously described [11].
Distal Vessel Quality (DVQ) score was calculated for each grafted vessel by assignment of a value from 0 to 3 to each one of the three following items: 1/vessel visibility, 2/vessel diameter, and 3/size of the vessel-dependent myocardial territory (named as “distribution”) as angiographically evaluated for each vessel. Final score for each vessel was the result of the addition of the score for each item (“single-vessel DVQ score”). The Mean DVQ score for each patient was the result of the cumulative score for all grafted vessels divided by the number of vessels (“mean global DVQ score”). Criteria to determine this score have been summarized in Table 1 and several representative examples are depicted in Figure 1. All analysis were performed by two interventional cardiologists with experience in angiographic analysis, blinded to outcomes of the grafts at the time of baseline images analysis, and interobserver variability was assessed.
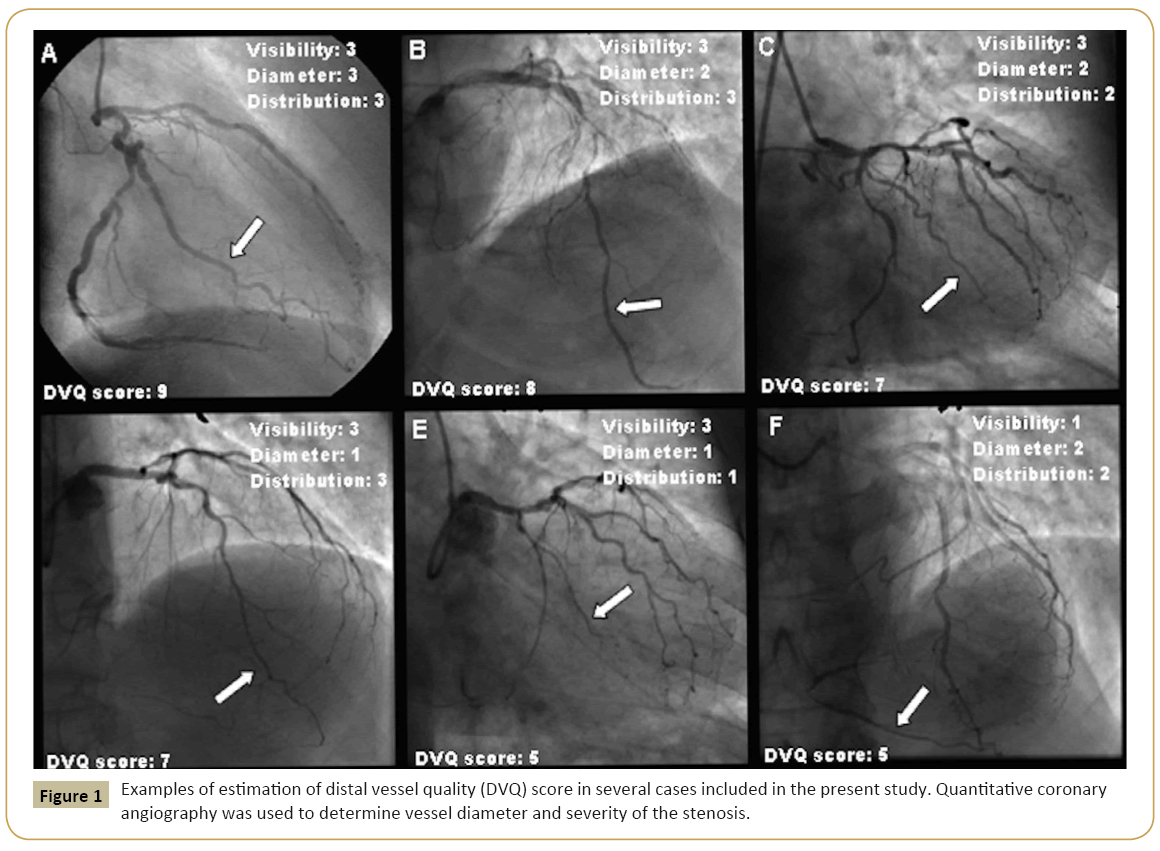
Figure 1: Examples of estimation of distal vessel quality (DVQ) score in several cases included in the present study. Quantitative coronary angiography was used to determine vessel diameter and severity of the stenosis.
| Visibility |
0 |
Occluded, suboptimally visualized |
| 1 |
Occluded, well visualized |
| 2 |
Not occluded, suboptimally visualized |
| 3 |
Not occluded, well visualized |
| Diameter |
0 |
Very small diameter: <1.5 mm |
| 1 |
Small diameter: 1.5-2 mm |
| 2 |
Medium diameter: 2-2.5 mm |
| 3 |
Large diameter: >2.5 mm |
| Distribution |
0 |
Impossible to evaluate |
| 1 |
Small distribution (non-dominant) |
| 2 |
Medium distribution (co-dominant) |
| 3 |
Large distribution (dominant) |
Table 1: Criteria to determine distal vessel quality (DVQ) score. It was calculated for each grafted vessel by assignment of a value from 0 to 3 to each one of the three following items: 1/vessel visibility, 2/vessel diameter, and 3/size of the vessel-dependent myocardial territory (named as “distribution”) as angiographically evaluated for each vessel.
Follow up of the study population
Clinical follow up was available for all patients. Also, coronary angiography if performed at follow up was evaluated through QCA to determine the presence of new significant coronary artery or grafts stenosis.
Statistical analysis
The data are expressed as absolute rate and percentage in case of qualitative variables. Quantitative variables are described as mean (SD) or median (25th-75th interquartile range [IQR]) depending on variable distribution. Group comparisons were analysed using Student’s t-test or its non-parametric equivalent, Mann-Whitney U-test for continuous variables, and Chi-square test or Fisher’s exact test for categorical variables. Statistical significance was defined as p-value <0.05. The variables associated with patency troubles of the bypass grafts were determined by univariate analysis. The univariate normality assumptions were verified with the Kolmogorov-Smirnov tests. Independent predictors of this main event were determined through logistic regression analysis including in the model the variables exhibiting a P value <0.10 in the univariate analysis. All hypothesis testing were two-sided with a significance level of 0.05.
Interobserver variability was assessed by Kappa-coefficient for the DVQ and the severity and number of coronary stenosis at baseline. The value of the DVQ score with the best sensitivity and specificity to determine graft patency was estimated by receiver operator curve (ROC) analysis. Also, Kaplan-Meier analysis to determine patency of the grafts in the follow up according to DVQ score was performed. Finally, syntax and DVQ scores were compared through correlation analysis test.
All analyses were conducted using the statistical package SPSS, version 18.0 (SPSS, Inc.; Chicago, Illinois, USA).
Results
Study population
A total of 249 consecutive patients who underwent single CABG between 2007 and 2010 with previous coronary angiography in our center were evaluated. The mean follow-up was of 6.5 ± 0.3 years (available for all patients, all with at least 5 years of follow-up). Mean age was 66.3 ± 9.7 years and 82.7% were males. Risk factors included hypertension in 53.4%, diabetes mellitus in 30.5%, and dyslipidemia in 49.8%. Other comorbidities have been summarized in Table 2 leading to a mean log Euro SCORE of 14% [13].
| Variables |
Global population n=249 |
Patients with events n=42 |
Patients without events n=207 |
p-value |
| |
Total grafts n=741 |
Occluded graft n=67 (9.1 %) |
Non-occluded graft n=674 (90.9 %) |
| Age (years) |
66.3 ± 9.7 |
64.7 ± 9 |
66 ± 9.9 |
0.317 |
| Gender (Male) |
206 (82.7%) |
53 (79.1%) |
570 (84.9%) |
0.209 |
| Hypertension |
133 (53.4%) |
49 (73.1%) |
346 (51.6%) |
0.001 |
| Diabetes Mellitus |
76 (30.5%) |
19 (28.4%) |
198 (29.5%) |
0.844 |
| Dyslipidemia |
124 (49.8%) |
37 (55.2%) |
337 (50.2%) |
0.435 |
| LDL-Cholesterol (mg/dL) |
181 ± 12 |
197 ± 10 |
178 ± 15 |
0.793 |
| Stroke |
6 (2.4%) |
1 (1.5%) |
17 (2.5%) |
0.999 |
| Peripheral artery disease |
9 (3.6%) |
4 (6.0%) |
20 (3.0%) |
0.264 |
| Chronic obstructive pulmonary disease |
1 (0.4%) |
0 (0%) |
4 (0.6%) |
0.999 |
| Chronic kidney disease |
2 (0.8%) |
0 (0%) |
7 (1%) |
0.999 |
| Previous Pacemaker |
1 (0.4%) |
1 (1.5%) |
1 (0.1%) |
0.173 |
| Obesity |
1 (0.4%) |
0 (0%) |
3 (0.4%) |
0.999 |
| Aspirin use |
201 (80.7) |
51 (76.1) |
579 (85.9) |
|
| Clopidogrel use |
22 (8.8) |
12 (17.9) |
57 (8.4) |
0.999 |
| Oral anticoagulation use |
57 (22.2) |
17 (25.4) |
108 (16.0) |
|
| Graft type |
| Mammary artery |
287 (38.7%) |
20 (29.9%) |
267 (39.8%) |
0.098 |
| Saphenous vein graft |
453 (61.1%) |
47 (70.1%) |
404 (60.2%) |
|
| Off-pump intervention |
24 (9.2) |
8 (11.9) |
61 (9.0) |
0.999 |
| Grafts |
| LIMA-LAD |
246 (33%) |
226 (33.7%) |
20 (2.9%) |
- |
| LIMA-RI |
19 (2.5%) |
1 (0.15%) |
18 (2.7%) |
| LIMA-DX |
70 (9.4%) |
3 (0.8%) |
67 (10.0%) |
| SVG-OM |
200 (27%) |
25 (3.7%) |
175 (26.1%) |
| SVG-RCA |
47 (6.3%) |
5 (0.7%) |
42 (6.2%) |
| SVG-PDA |
110 (14.8%) |
7 (1.0%) |
103 (15.3%) |
| SVG-PLA |
46 (6.2%) |
6 (0.9 %) |
40 (6.0 %) |
| Visibility |
| Occluded, bad visualized |
8 (1.1%) |
2 (3%) |
6 (0.9%) |
0.119 |
| Occluded, well visualized |
91 (12.3%) |
5 (7.5%) |
86 (12.8%) |
| Not occluded, regularvisualized |
17 (2.3%) |
0 (0%) |
17 (2.5%) |
| Not occluded, well visualized |
622 (84.3%) |
60 (89.6%) |
562 (83.8%) |
| Diameter |
| Small diameter: 1.5-2 mm |
38 (5.1%) |
5 (7.5%) |
33 (4.9%) |
|
| Medium diameter: 2-2.5 mm |
176 (23.8%) |
22 (32.8%) |
154 (23%) |
| Large diameter: > 2.5 mm |
522 (70.7%) |
40 (59.7%) |
482 (71.8%) |
| Distribution |
|
|
|
|
| Small distribution |
26 (3.5%) |
0 (0%) |
26 (3.9%) |
0.011 |
| Medium distribution |
95 (12.9%) |
17 (25.4%) |
78 (11.6%) |
| Large distribution |
615 (83.3%) |
50 (74.6%) |
565 (84.2%) |
| Syntax score |
32 [30-33] |
32 [29-33] |
32 [30-33] |
0.142 |
| Single Vessel DVQ score = 9 |
426 (61.6%) |
34 (50.7%) |
423 (63%) |
0.048 |
DX: diagonal; LAD: left anterior descending; LDL: Low-density lipoproteins; LIMA: Left internal mammary artery; OM: Obtusemarginal; PDA: posterior descending artery; PLA: posterior lateral artery; RCA: Right coronary artery; RI: Ramus intermedius. SVG:Saphenous vein graft.
Table 2: Comparison of main baseline clinical and anatomical characteristics for patients with or without occluded coronary grafts suffering from coronary events at 5 years follow-up.
Angiographic and anatomical characterization: DVQ score
Anatomical information (visibility, diameter and distribution) of the distal vessels of the affected coronary arteries were evaluated, as described in Table 1, by two interventional cardiologists with experience in QCA, from the coronary angiography performed before CABG surgery. Mean single-vessel DVQ score for visibility, diameter, and distribution was 8.13 ± 1.38. Interobserver variability for the determination of DVQ score was estimated showing a ponder Kappa of 0.9854, 95% CI (0.9679-1), p=0.0089. Also, a mean Syntax score of 31.13 ± 3.07 was calculated.
Each patient received a mean of 2.9 bypass grafts, up to a total of 741 grafts to the following target vessels: LAD artery (33.2%), obtuse marginal artery (27.3%); posterior descending artery (PDA) (14.8%), diagonal branch (DX) (9.4%), right coronary artery (RCA) (6.5%), posterolateral artery (PLA) (6.2%), and ramus intermedius (RI) (2.6%). Distribution of grafts and events related to them, according to the single-vessel DVQ score, has been summarized in Figure 2. A 61.3% (453) were venous grafts and 38.7% (287) were arterial grafts, most of them (85.2%) from the left internal mammary artery.
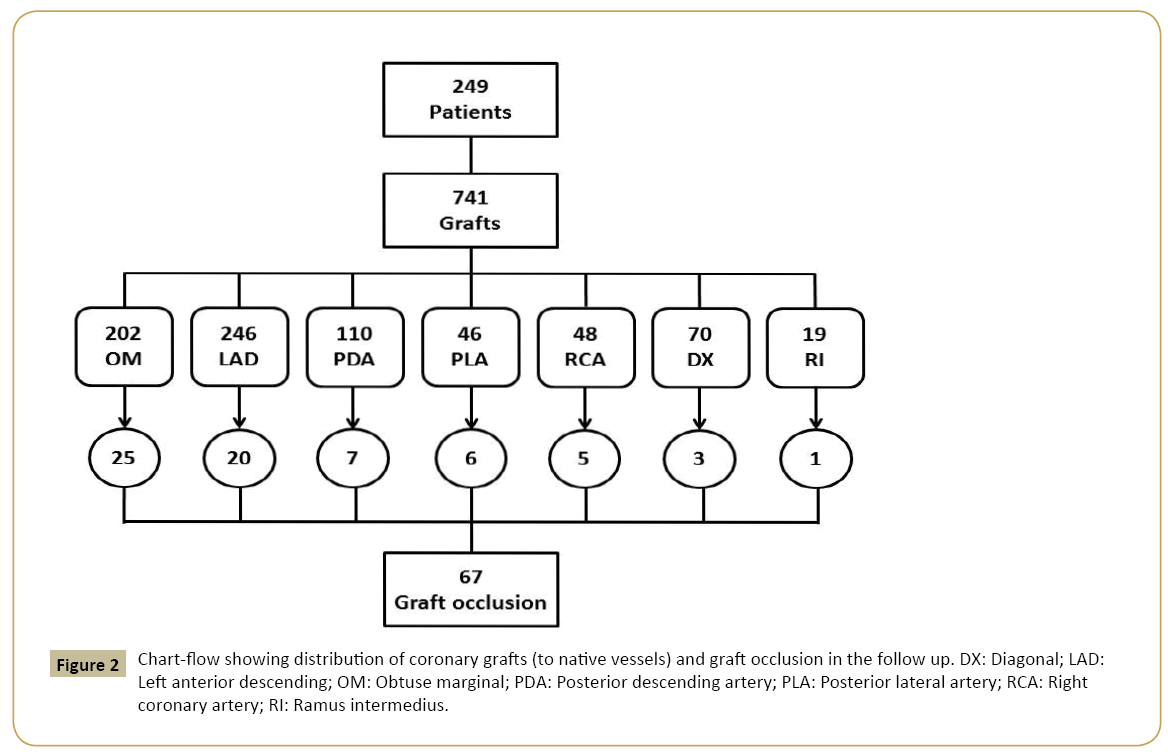
Figure 2: Chart-flow showing distribution of coronary grafts (to native vessels) and graft occlusion in the follow up. DX: Diagonal; LAD: Left anterior descending; OM: Obtuse marginal; PDA: Posterior descending artery; PLA: Posterior lateral artery; RCA: Right coronary artery; RI: Ramus intermedius.
Clinical events and angiographical outcomes
At follow-up, 44 patients (17.7%) required new admission due to cardiac events and all of them underwent new angiographic evaluation. Of them, 42 patients (16.8% from global population, and 95.4% from those with clinical events) presented new bypass graft occlusion. Main individual characteristics of these patients have been summarized in Table 3. Reasons for re-admission included ST-elevation myocardial infarction (STEMI) (2.4%), Non- ST-elevation myocardial infarction (NSTEMI) (11.9%), unstable angina (50%), stable angina (31%), or others (4.7%). Occlusion of 67 (9.1%) grafts was angiographically demonstrated at a median time from surgery of 511 days [IQR: 168-606], specially affecting those sutured to the PLA (6/46, 13%) followed by those sutured to obtuse marginal (25/202, 12.4%) and the LAD (20/246, 8.1%). Distribution of events according to the affected graft has been summarized in Figure 2 and time distribution in Figure 3. Comparison of patients who developed bypass graft occlusion and those who did not has been summarized in Table 2. To remark, no differences in terms of dyslipidemia severity or technical issues (as type of graft, off pump intervention, use of sequential grafts, or operators) were found. Bypass dysfunction affected more frequently patients with arterial hypertension (73.1% vs. 51.6%, p=0.001) without any other significant difference concerning other cardiovascular risk factors or LDL-cholesterol levels. Venous grafts were 2.5 times more frequently occluded than arterial grafts (p=0.098). A mean DVQ score of 7.6 predicted with the best sensitivity (64%) and specificity (59%) the development of clinical events (STEMI, NSTEMI, progressive/new angina, or cardiac mortality) in the follow up with an area under the curve of 0.592 (CI 95% [0.507-0.677]). In particular, a single-vessel DVQ score of 9 was associated to a rate of graft patency at follow up of 93% as opposed to 88% when DVQ score was <9, p=0.048. The combination of a single-vessel DVQ score <9 (n=282 grafts) and the use of a SVG (69% of them) was associated to a rate of graft occlusion of 14.3% as opposed to 7.4% in those with DVQ score=9 and SVG (55.8%), p=0.020. No differences were found in the Syntax score between patients who presented graft occlusion 32 and those who did not 32 p=0.142. The use of arterial grafts (OR=0.217, 95% CI [0.064-0.737], p=0.014) and higher values of single vessel DVQ score (OR=0.555, 95% CI [0.370-0.832], p=0.004) were independent predictors of bypass graft patency at 5-year follow-up.
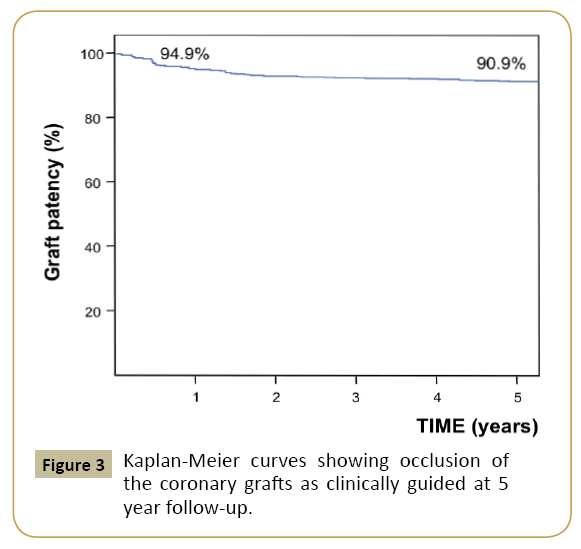
Figure 3: Kaplan-Meier curves showing occlusion of the coronary grafts as clinically guided at 5 year follow-up.
| Age |
Gender |
DM-2 |
Reason of admission |
Syntax score (%) |
Mean DVQ score |
Type of graft |
Occluded graft/single vessel DVQ score |
| 50 |
Male |
Yes |
Unstable angina |
35 |
8.71 |
Art+Ven |
LIMA-LAD/8,SVG-OM/9 |
| 45 |
Male |
No |
Unstable angina |
32 |
8.85 |
Ven |
SVG-OM/9 |
| 45 |
Male |
No |
Unstable angina |
33 |
7.85 |
Art |
LIMA-LAD/9 |
| 58 |
Male |
No |
Unstable angina |
29 |
8.28 |
Ven |
SVG-OM/8 |
| 75 |
Male |
No |
Unstable angina |
30 |
8.42 |
Ven |
SVG-LAD/8 |
| 75 |
Female |
No |
Unstable angina |
28 |
8.42 |
Ven+Ven |
SVG-LAD/9, SVG -OM/7 |
| 44 |
Female |
No |
Unstable angina |
29 |
8.42 |
Ven |
SVG-OM/9 |
| 73 |
Male |
Yes |
Unstable angina |
32 |
5.00 |
Ven |
SVG-LAD/9 |
| 72 |
Male |
No |
Unstable angina |
33 |
7.00 |
Ven+Ven+Ven |
SVG-LAD/7, SVG-OM/9, SVG-RCA/6 |
| 67 |
Male |
No |
Unstable angina |
33 |
7.28 |
Ven |
SVG-LAD/8 |
| 63 |
Male |
No |
Unstable angina |
26 |
8.57 |
Ven |
SVG-LAD/9 |
| 54 |
Male |
No |
Unstable angina |
36 |
9.00 |
Ven+Ven+Ven |
LIMA-LAD/9, SVG-OM/9, SVG-RCA/9 |
| 60 |
Female |
Yes |
Unstable angina |
30 |
7.42 |
Art+Art+Art+Ven |
LIMA-LAD/9, LIMA-OM/4Radial-PLA/8, SVG-PDA/7 |
| 82 |
Male |
No |
Unstable angina |
34 |
8.28 |
Art+Ven |
LIMA-LAD/9SVG-OM/9 |
| 65 |
Male |
No |
Unstable angina |
32 |
8.14 |
Art+Ven+Ven+Ven |
LIMA-LAD/8, SVG-OM/9, SVG-PDA/8, SVG-PLA/9 |
| 81 |
Male |
No |
Unstable angina |
33 |
9.00 |
Ven |
SVG-OM/9 |
| 62 |
Male |
No |
Unstable angina |
31 |
8.14 |
Art+Art+Ven+Ven |
LIMA-LAD/9, LIMA-OM/9, SVG-PDA/7, SVG-PLA/7 |
| 67 |
Male |
No |
Unstable angina |
37 |
8.42 |
Art+Art |
LIMA-LAD/9, LIMA-OM/9 |
| 52 |
Male |
No |
Unstable angina |
33 |
8.32 |
Ven |
SVG-RCA/9 |
| 58 |
Male |
Yes |
Unstable angina |
31 |
8.14 |
Ven |
SVG-OM/9 |
| 66 |
Male |
Yes |
Unstable angina |
36 |
8.28 |
Ven |
SVG-OM/9 |
| 69 |
Male |
No |
STEMI |
30 |
6.14 |
Art |
LIMA-LAD/7 |
| 59 |
Female |
No |
Stable angina |
30 |
7.71 |
Art+Ven+ Ven+Ven |
LIMA-LAD/9, SVG-OM/7, SVG-PDA/7, SVG-PLA/7 |
| 72 |
Male |
Yes |
Stable angina |
31 |
8.42 |
Ven |
SVG-OM/9 |
| 51 |
Male |
Yes |
Stable angina |
28 |
8.00 |
Ven |
SVG-OM/9 |
| 61 |
Male |
No |
Stable angina |
33 |
8.28 |
Ven |
SVG-OM/9 |
| 56 |
Male |
No |
Stable angina |
33 |
7.42 |
Ven |
SVG-OM/9 |
| 68 |
Male |
Yes |
Stable angina |
30 |
7.85 |
Art+Art+Art+Ven |
LIMA-LAD/9LIMA-RI/9Radial-OM/9SVG-PDA/6 |
| 76 |
Male |
No |
Stable angina |
34 |
8.14 |
Ven |
SVG-LAD/9 |
| 70 |
Male |
No |
Stable angina |
32 |
7.71 |
Art+Ven |
LIMA-LAD/9, SVG-OM/9 |
| 65 |
Female |
No |
Stable angina |
29 |
7.71 |
Ven |
SVG-PLA/3 |
| 67 |
Male |
No |
Stable angina |
32 |
8.71 |
Ven |
SVG-PLA/9 |
| 74 |
Male |
Yes |
Stable angina |
35 |
8.57 |
Ven |
SVG-DX/7 |
| 56 |
Male |
No |
Stable angina |
31 |
7.57 |
Ven |
SVG-RCA/8 |
| 78 |
Male |
No |
Stable angina |
32 |
7.42 |
Ven |
SVG-DX/6 |
| 80 |
Male |
No |
Other |
33 |
8.42 |
Ven |
SVG-PDA/7 |
| 66 |
Male |
Yes |
Other |
33 |
7.85 |
Ven |
SVG-RCA/7 |
| 54 |
Female |
Yes |
NSTEMI |
34 |
6.71 |
Ven |
SVG-OM/6 |
| 72 |
Male |
No |
NSTEMI |
33 |
7.14 |
Ven |
SVG-PDA/7 |
| 62 |
Male |
No |
NSTEMI |
24 |
5.57 |
Ven |
SVG-DX/9 |
| 60 |
Male |
No |
NSTEMI |
33 |
5.57 |
Art+Ven |
LIMA-LAD/9, SVG-OM/4 |
| 75 |
Male |
No |
NSTEMI |
30 |
7.85 |
Ven |
SVG-OM/7 |
Art: Arterial graft; DX: Diagonal; DVQ: Distal vessel quality (score); LAD: left anterior descending artery; LIMA: left internal mamary artery; NSTEMI: non-ST segment elevation myocardial infarction; OM: Obtuse marginal; PDA: Posterior descending artery; PLA: Posterolateral artery; RI: Ramus intermedius; STEMI: ST segment elevation myocardial infarction; SVG: saphenous vein graft; Ven: Venous graft.
Table 3: Individual clinical and anatomical profile of patient who underwent coronary bypass graft surgery and suffered from new coronary event in the follow up.
Discussion
Current American and European revascularization guidelines recommend CABG as first choice for patients with 3-vessel disease, 2-vessel disease affecting proximal LAD, and diseased left main [14,15]. Among 249 patients who underwent CABG following these indications, occlusion of the grafts was detected in 9.1% of the cases at a median time from surgery of 1.4 years. To remark, this finding followed clinically indicated angiography. Anatomical predictors of this event included the use of venous grafts (70.1%), single vessel and mean global DVQ scores, but not Syntax score. We found that the combination of venous grafts with DVQ score <9 were associated to poor outcomes and high rate of early graft unpatency. Many cardiologists and surgeons feel that primary clinical benefit of bypass comes from a LIMA to LAD graft given that over time most SVG become diseased or occluded. We believe that despite the opportunity of bypass all diseased vessels, the benefit of doing that in vessels with a DVQ of less than 9 present certain limitations. Therefore, this new score may help to improve the selection of the best revascularization strategy promoting hybrid approaches. Besides, the DVQ score is a new tool useful for comparison of results in future research in the field of CABG.
Decision tools to choose revascularization strategy for complex coronary artery disease
Risk stratification is an integral and increasingly important aspect of the assessment of patients with complex coronary artery disease. Heart team consensus based on several risk models has become the recommended approach for the decision making process [14,15]. Most common risk models take into consideration clinical variables (STS, Euroscore) [16,17] or anatomical variables (SYNTAX) [11]. The progressive development of anatomical-based risk scores culminating in the SYNTAX score II (that can better guide decision making between CABG and PCI than the original anatomical SYNTAX score) [18] has undoubtedly improved the performance of these risk models in terms of stratification for the individual patient. Nevertheless, Syntax lacks of accuracy to predict graft-related events as evidenced by the bad correlation with the DVQ score (Figure 4). The ideal score is far from these models and the effort to develop a model integrating anatomical and clinical data has sacrificed simplicity reducing its applicability in real practice. Visual assessment is more representative with the daily practice and real life at catheterization laboratories than quantitative assessment; likewise it is quicker and useful to make decisions about the best revascularization strategy. Frequently this decision is taken in the catheterization laboratory. According to our findings, the DVQ score may help to decide more objectively which cases could benefit from a percutaneous approach performed within the same index procedure, which patients may benefit more from surgical revascularization, or if hybrid strategies need to be further discussed.
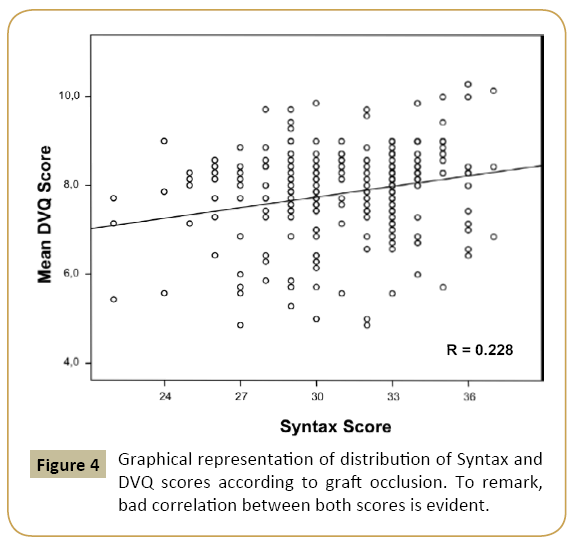
Figure 4: Graphical representation of distribution of Syntax and DVQ scores according to graft occlusion. To remark, bad correlation between both scores is evident.
Rate and predictors of dysfunction of CABG
Long-term patency of the coronary bypass grafts is one of the main determinants of outcomes after cardiac surgery [3]. In our study the graft occlusion was found in a 9.1% of the patients due to a clinical event, at a median time from surgery of 1.4 years, which is consistent with previous studies reporting a 1-year rate of occlusion of up to 13% [5,6] when angiography is systematically performed. Apart from clinical factors related to grafts’ outcomes (Table 2) and technical aspects of the surgery (including the use of arterial grafts) [3,4], there is scarce evidence on the influence of other anatomical factors [10]. Previous attempts to assess the distal vessels quality had been reported. Nevertheless, the complexity and invasiveness of these methods precluded from their use as therapeutic guiding [19]. As a matter of fact, in daily routine evaluation of the quality of the distal vessel is commonly performed under subjective criteria. To remark, the extended use of a consensus score to assess the quality of the distal vessel before grafting may be a useful tool for both, the clinical decisionmaking process and research as it may allow analysis of results under comparable criteria [20,21]. We elaborated a simple descriptive score that presented a clear association with bypass occlusion. Indeed, only optimal values of single-vessel DVQ score (=9) were related to adequate outcomes of SVG (98.7% of patency at 5-year) while DVQ scores <9 presented a rate of SVG occlusion of 59.6% (p=0.017).
Diameter of a grafted vessel has been previously associated with higher rate of occlusion or dysfunction of arterial and vein grafts [10]. Accordingly, a low DVQ score and a diameter under 2.5 mm (one of the items evaluated by this score) strongly suggested risk of graft unpatency at mid-term. Specifically, the proportion of native vessel lumen diameter under 2.5 mm among patients with graft occlusion (40.3%) was significantly higher than in patients free of events (with 30.2%, p=0.011).
To remark, predictability of graft occlusion with this new score was much better than with Syntax score (Table 2), which is somehow logical as the Syntax score was mainly based on predictors of failure for percutaneous interventions and not surgical outcomes [11]. Accordingly, a lack of correlation between both scores was detected (Figure 4).
Alternative strategies in the scenario of complex coronary artery disease
CABG continues to be the preferred strategy to treat threevessel disease. One of the main theoretical advantages of this approach is that it allows a complete revascularization with lower risk of events as compared to percutaneous revascularization [14,15]. Nevertheless, new generations drug-eluting stents have demonstrated low rate of target lesion revascularization [22,23] and some recent studies suggest that the use of everolimus eluting stents in patients with diabetes mellitus and multi-vessel disease, was associated with lower upfront risk of death compared with CABG surgery and a similar risk of death at long term [24]. In addition, the debate concerning the degree of revascularization (total if surgery vs. partial if PCI), is no longer binary given the current results of percutaneous techniques in the field of chronic total occlusions (up to 80-90% of success), that make them rise as a good alternative to achieve complete revascularization with low rates of complications [24]. Since comparison of these different strategies has not been performed taking into consideration the quality of the distal vessel, accurate conclusions cannot be obtained. Eventually, surgical revascularization is losing the status quo of the last decades and will need to incorporate imaginative alternatives to keep on offering better outcomes in complex coronary disease. This includes hybrid procedures that can combine the benefits of a minimal invasive surgery providing a LIMA graft to the LAD and stenting of the circumflex and/or the right coronary artery [21,24]. Also, newer approaches including the use of prosthetic conduits or external stenting for SVG [25] are under research. The use of the DVQ score for analysis of the outcomes may help to better understand the best alternatives to treat our patients.
Study Limitations
The study was conducted in a single high-volume tertiary center what may had conditioned the results of CABG. The cohort size could have been underpowered for analyses of outcomes and the influence of cardiovascular risk factors, but the strict follow up at 5-year increases the value of the results. Although interobserver variability was assessed, external validation under prospective analysis of this score will have to be performed. Also, angiographic characterization of the degree of atherosclerosis of the saphenous grafts will be needed as its impact could not be evaluated in the present study. Finally, the DVQ score could not be evaluated in the present study for alternative grafts different to SVG and LIMA.
Conclusion
The DVQ score is a new simple tool to predict outcomes of coronary artery bypass grafts. Lower values of this score, especially when vein grafts are used, suggest little benefit of grafting certain vessels. Therefore, this score could be useful to identify patients who may benefit from percutaneous revascularization or hybrid strategies.
References
- Mozaffarian D, Benjamin EJ, Go AS, Arnett DK, Blaha MJ, et al. (2015) Heart Disease and Stroke Statistics-2015 Update: A Report From the American Heart Association. Circulation 131: 29-322.
- Widimsky P, Holmes DR (2011) How to treat patients with ST-elevation acute myocardial infarction and multi-vessel disease? European Heart Journal 32:396-403.
- Boylan MJ, Lytle BW, Loop FD, Taylor PC, Borsh JA, et al. (1994) Surgical treatment of isolated left anterior descending coronary stenosis. Comparison of left internal mammary artery and venous autograft at 18 to 20 years of follow-up. J Thorac Cardiovasc Surg 107:657-662.
- Loop FD, Lytle BW, Cosgrove DM, Stewart RW, Goormastic M, et al. (1986) Influence of the internal-mammary-artery graft on 10-year survival and other cardiac events. N Engl J Med 314:1-6.
- Parang P, Arora R (2009) Coronary vein graft disease. Pathogenesis and prevention. Can J Cardiol 25: 57-62
- Desai ND, Cohen EA, Naylor CD, Fremes SE (2004) A randomized comparison of radial-artery and saphenous-vein coronary bypass grafts. N Engl J Med 351:2302-2309.
- Loop FD, Golding LR, MacMillan JP, Cosgrove DM, Lytle BW, et al. (1983) Coronary artery surgery in women compared with men: analyses of risks and long-term results. J Am Coll Cardiol1:383-390.
- Rodés-Cabau J, Facta A, Larose E, DeLarochellière R, Déry JP, et al. (2007) Predictors of Aorto-Saphenous Vein Bypass Narrowing Late After Coronary Artery Bypass Grafting. The American Journal of Cardiology. 100:640-645.
- Sabik JF, Lytle BW, Blackstone EH, Houghtaling PL, Crosgrove DM (2005) Comparison of saphenous vein and internal thoracic artery graft patency by coronary system. Ann Thorac Surg 79:544-551.
- Bourassa MG, Fisher LD, Campeau L, Gillespie MJ, McConney M, et al. (1985) Long-term fate of bypass grafts: the Coronary Artery Surgery Study (CASS) and Montreal Heart Institute experiences. Circulation 72:71-78.
- Sianos G, Morel MA, Kappetein AP, Morice MC, Colombo A, et al. (2005) The SYNTAX score: an angiographic tool grading the complexity of coronary artery disease. EuroIntervention1:219-227.
- Ngaage DL, Hashmi I, Griffin S (2010) To graft or not to graft? Do coronary artery characteristics influence early outcomes of coronary artery bypass surgery? Analysis of coronary anastomoses of 5171 patients. J Thorac Cardiovasc Surg 140:66-72.
- Sharma GV, Khuri SF, Folland ED, Barsamian EM, Parisi AF (1983) Prognosis for aorta-coronary graft patency. A comparison of preoperative and intraoperative assessments. J Thorac Cardiovasc Surg. 85:570-576
- Stettler C, Wandel S, Allemann S, Kastrati A, Morice MC, et al. (2007) Outcomes associated with drug-eluting and bare-metal stents: a collaborative network metaanalysis. Lancet 370:937-948.
- Garg S, Serruys P (2010) Coronary Stents. J Am Coll Cardiol 56:1-42.
- Park KW, Chae IH, Lim DS, Han KR, Yang HM, et al. (2011) Everolimus-eluting versus sirolimus-eluting stents in patients undergoing percutaneous coronary intervention: the EXCELLENT (Efficacy of Xience/Promus Versus Cypher to Reduce Late Loss After Stenting) randomized trial. J Am Coll Cardiol58:1844-1854.
- Pancholy SB, Boruah P, Ahmed I, Kwan T, Patel TM, et al. (2013) Meta-analysis of effect on mortality of percutaneous recanalization of coronary chronic total occlusions using a stent-based strategy. Am J Cardiol111:521-525.
- Patel VG, Brayton KM, Tamayo A, Mogabgab O, Michael TT, et al. (2013) Angiographic Success and Procedural Complications in Patients Undergoing Percutaneous Coronary Chronic Total Occlusion Intervention. A Weighted Meta-Analysis of 18,061 Patients From 65 Studies. J Am Coll CardiolIntv 6:128-136.
- Michel P, Roques F, Nashef SA (2003) Logistic or additive EuroSCORE for high-risk patients. Eur J Cardiothorac Surg 23: 684-687.
- Patel M (2012) Appropriate Use Criteria for Coronary Revascularization Focused Update. J Am Coll Cardiol59:857-881.
- Kolh P, Windecker S, Alfonso F (2014) ESC/EACTS Guidelines on myocardial revascularization. The Task Force on Myocardial Revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). European Heart Journal 31: 2501-2555.
- Geissler HJ, Hölzl P, Marohl S, Kuhn-Régnier F, Mehlhorn U, et al. (2000) Risk stratification in heart surgery: comparison of six score systems. Eur J Cardiothorac Surg 17: 400-406.
- Nam CW, Mangiacapra F, Entjes R, Chung IS, Sels JW, et al. (2011) Functional SYNTAX Score for Risk Assessment in Multivessel Coronary Artery Disease. J Am Coll Cardiol58:1211-1218.
- Bangalore S, Guo Y, Samadashvili Z, Blecker S, Xu J,et al. (2015) Everolimus Eluting Stents Versus Coronary Artery Bypass Graft Surgery for Patients With Diabetes Mellitus and Multivessel Disease.Circ Cardiovasc Interv8.
- Desai M, Seifalian AM, Hamilton G (2011) Role of prosthetic conduits in coronary artery by-pass grafting. Eur J Cardiothorac Surg 40:394-398.

