Keywords
Mammography; Breast cancer; Screening; False-positive; Anxiolytic drugs; Antidepressant drugs; Hormone therapy
Introduction
The purpose of mammography screening is to reduce breast cancer mortality [1]. However, screening comes along with some controversial side effects. A major concern is falsepositive results (i.e., positive screening results in women without breast cancer). In Denmark, the risk of a false-positive result over 10 screens has been estimated to be 7-16% [2], while this rate can be much higher in other countries such as the United States where it was estimated to be 63% [3,4].
False-positive screening results have been found to pose negative psychological effects [5,6]. A recent study from Denmark showed that women with a false-positive screening result were more likely to experience psychological distress for up to 3 years as compared to women with a negative screening result [7]. In Denmark, where access to the general practitioners (GPs) is free of charge, about one third of all contacts to GPs concerns psychological disorders [8], and the GPs are entitled to prescribe anxiolytic- and antidepressant drugs. It is therefore reasonable to expect an increase in the use of these drugs if a false-positive screening result causes anxiety. To test this hypothesis, we undertook a populationbased register study in Denmark covering the period 1997-2006 [8]. We found that women with a false positive screening result had a higher consumption of anxiolytic- and antidepressant drugs after this screen than they had before. But the same change over time was seen in women with negative screening results. Our study did therefore not support a causal association between a false-positive screening result and increased use of anxiolytic- and antidepressant drugs.
However, over the two years prior to the screen, there were significantly more users of anxiolytic- and antidepressant drugs among women with a later false-positive than among women with a later negative screening result. This could indicate selection. Hormone therapy has been widely prescribed to women with menopausal syndromes [9]. But data concerning negative side-effects such as increased risk of breast [10] and ovarian cancer [11], dementia and mild cognitive impairment [12] started to be published in the summer of 2002. Therefore, the European Agency for Evaluation of Medicinal Products (EMEA) in December 2003 issued a recommendation on appropriate, restricted use of hormone therapy [13], and the use decreased [14]. Non-hormonal alternatives for treatment of menopausal hot flashes have been searched for, and suggested alternatives include antidepressants and drugs used for a variety of neurologic and psychiatric disorders [15].
On this basis, we re-analyzed our previous study, dividing the observations into the years prior to and after the new EMEA recommendation [13]. Our hypothesis was that antidepressant use to some extent had replaced hormone use, and that this change in particular had affected women at risk of later becoming false-positive in mammography screening.
Methods
The study followed the difference-in-differences methodology. The data included: Women recorded in the Copenhagen screening mammography register 1997-2006, and their prescribed drugs recorded in the Danish National Prescription Registry (DNPR) 1995-2008.
In the Copenhagen mammography screening program women aged 50-69 years are personally invited on a biennial basis. Information on screening date and outcome is recorded in the mammography screening register, with each woman identified by her unique personal number. All women who experienced a false-positive result during the study period were included in the false-positive group at their first falsepositive screening result in the study period. For each falsepositive woman, five women with the same age, the same screening date, and with a negative screening result were selected at random, using a computerized system, from the mammography register to form a comparison group. Once a woman had experienced a false-positive screening result, she would not be included in the comparison group. The study period for each woman started two years before the screen, ranging from 1995 to 2006, and ended two years after the screen, ranging from 1997 to 2008. Women not present in Denmark during their entire four years of observation were excluded, leaving 11,436 women in the study.
In the DNPR, prescribed drugs are registered by the unique personal number. Consumption is measured in Defined Daily Doses (DDDs) defined as “the assumed average maintenance dose per day for a drug used for its main indication in adults” [16] (WHO, 2009). We investigated the drug consumption in two major categories: genitourinary system and sex hormones drugs (G) including G03C estrogens, G03D progestogens, and G03F a combination of estrogens and progestogens (in the following referred to as hormone therapy), and nervous system drugs (N) including N02 analgesics, N05 psycholeptics, N06 psychoanaleptics, and N07 other nervous system drugs (in the following referred to as anxiolytic- and antidepressant).
We calculated the proportion of drug users and mean DDDs per user in the false-positive group and in the negative comparison group in the two years before and in the two years after the screening event. The analysis was made for screening events in 1997-2006; 1997-2003 (prior to EMEA recommendation); and 2004-2006 (following EMEA recommendation). Risk ratios (RRs) including 95% confidence intervals (CIs) were used for comparison between two proportions, e.g., proportion of drug users in 2004-2006 with that in 1997-2003 in the false-positive group after the screening event. Ratios of risk ratios (RRRs) including 95% CIs were used for comparison between four proportions, e.g., proportion of drug users in 1997-2006 in the false-positive group after the screening event compared with that before the screening event and divided by the same ratio for the negative group. Ratios of means, and ratios of ratios of means were used for comparison and mean DDDs per user. Statistical analyses were carried out with SAS 9.1. and Vassar Stats© Richard Lowry 1998–2015. Ratios of means with 95% CI were calculated in GraphPad, ©2016 GraphPad Software, Inc.
Results
Among the 11,436 women included in the study, 1906 were in the false-positive group and 9530 in the negative group. The data for the entire study population distributed by before and after screening event, drug use and screening result are reported in Figure 1. These data are later divided into the time periods before and after the EMEA recommendations.
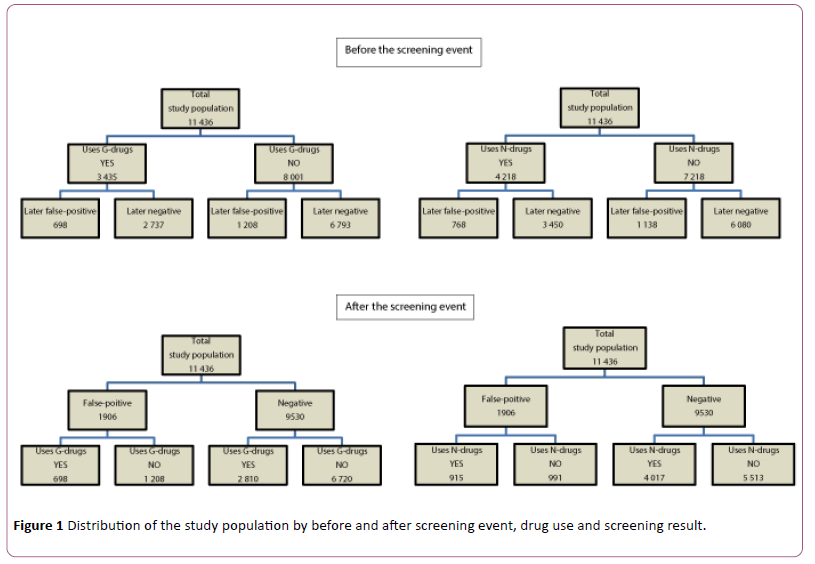
Figure 1: Distribution of the study population by before and after screening event, drug use and screening result.
In the entire period 1997-2006, the RRR (for false-positives in relation to negatives and after versus before screening event) for hormone therapy was 0.97 (95% CI 0.87-1.10), with similar patterns for 1997-2003 (RRR 0.99, 95% CI 0.93-1.06) and for 2004-2006 (RRR 0.93, 95% CI 0.71-1.22). For the mean DDD of hormone therapy, these RRRs were 0.92 (95% CI 0.78-1.09), 0.92 (95% CI 0.78-1.13), and 0.90 (95% CI 0.75-1.13), respectively. In the case of progesterone, the figures concerning the mean DDD were RRR 0.80 (95% CI, 0.66.0.97), 0.18 (95% CI, 0.14-0.24) and 0.70 (95% CI, 0.58-0.85), Table 1.
| |
Ratio after/before for number of women, by time of screening event, using drugs |
Ratio after/before for mean dose (DDD/woman), by time of screening event |
| Type of mammography screen/ Drug type |
1997-03 |
2004-06 |
1997-06 |
1997-03 |
2004-06 |
1997-06 |
| G - drugs |
0.99
0.93-1.06
p=0.777 |
0.93
0.71-1.22
p=0.603 |
0.97
0.87-1.10
p=0.920 |
0.92
0.78-1.13
p=0.345 |
0.90
0.75-1.07
p=0.240 |
0.92
0.78-1.09
p=0.354 |
| Estrogen (G03C) |
0.93
0.75-1.15
p=0.507 |
0.93
0.79-1.17
p=0.689 |
0.95
0.81-1.10
p=0.480 |
0.93
0.77-1.13
p=0.493 |
0.83
0.67-1.03
p=0.097 |
0.91
0.75-1.11
p=0.377 |
| Progesterone (G03D) |
1.03
0.63-1.68
p=0.920 |
0.94
0.28-3.12
p=0.920 |
0.98
0.70-1.38
p=0.920 |
0.80
0.66-0.97
p=0.021 |
0.18
0.14-0.24
p<.0001 |
0.70
0.58-0.85
p=0.000 |
| Combination of Estrogen and Progesterone (G03F) |
1.01
0.85-1.20
p=0.920 |
0.96
0.62-1.48
p=0.841 |
1.01
0.86-1.18
p=0.920 |
0.91
0.78-1.06
p=0.215 |
1.01
0.87-1.17
p=0.887 |
0.92
0.79-1.07
p=0.265 |
| N – drugs |
1.04
0.92-1.17
p=0.543 |
0.97
0.78-1.21
p=0.806 |
1.02
0.92-1.14
p=0.671 |
1.05
088-1.26
p=0.572 |
0.97
0.84-1.13
p=0.689 |
1.02
0.86-1.21
p=0.806 |
| Analgetics (N02) |
1.04
0.82-1.32
p=0.764 |
0.91
0.58-1.43
p=0.689 |
1.03
0.91-1.18
p=0.639 |
0.91
0.67-1.26
p=0.584 |
1.11
0.80-1.53
p=0.549 |
0.94
0.69-1.30
p=0.718 |
| Psycholeptics (N05) |
1.08
0.90-1.30
p=0.390 |
0.91
0.64-1.28
p=0.578 |
1.03
0.91-1.17
p=0.663 |
0.98
0.79-1.22
p=0.887 |
0.97
0.79-1.19
p=0.764 |
0.97
0.79-1.21
p=0.806 |
| Psychoanaleptics (N06) |
0.93
0.72-1.20
p=0.578 |
1.09
0.74-1.61
p=0.645 |
0.97
0.80-1.18
p=0.777 |
1.19
1.05-1.35
p=0.007 |
0.84
0.76-0.94
p=0.003 |
1.03
0.94-1.20
p=0.351 |
| Other (N07) |
1.21
0.71-2.06
p=0.475 |
1.10
0.46-2.61
p=0.823 |
1.17
0.75-1.83
p=0.493 |
0.96
0.86-1.07
p=0.435 |
1.03
0.94-1.13
p=0.502 |
0.98
0.88-1.08
p=0.655 |
Table 1: Ratio of risk ratios for after versus before, 95% confidence intervals and p-values*. * Ratio of risk ratios for after versus before, 95% confidence intervals, and p-values in number of women using drugs and in mean dose (DDD/woman) by mammography outcome, time period in relation to the screening event, and time period in relation to recommendation for prescription of hormone therapy. G-Drug=Hormone therapy; N-Drug=anxiolytic-and antidepressant drugs; DDD=Daily Defined Doses.
Anxiolytic- and antidepressant drugs, summary results
A similar pattern was seen for use of anxiolytic-and antidepressant drugs. In 1997-2006, the RRR for these drugs was 1.02 (95% CI 0.92-1.14), with no change between 1997-2003 and 2004-2006, RRR 1.04 (0.92-1.17) and 0.97 (95% CI 0.78-1.21), respectively. Also, here a similar pattern was seen for mean DDD of anxiolytic-and antidepressant drugs, the RRRs were 1.02 (95% CI 0.86-1.21), 1.05 (95% CI 0.88-1.26) and 0.97 (95% CI 0.84-1.13), respectively, Table 1.
Hormone therapy use, before the screening event versus after screening event
In the period before the screening event, women who later experienced a false-positive screening result had a higher consumption of hormone therapy than women who later experienced a negative screening result. The RRs for the proportions were 1.28 (95% CI 1.19-1.36) for the entire period 1997-2006; 1.32 (95% CI 1.23-1.42) for 1997-2003, and 1.10 (95% CI 0.93-1.29) for 2004-2006. Smaller differences were seen between the two groups when it came to the mean DDD, where no difference was seen in 2004-2006, Figure 2.
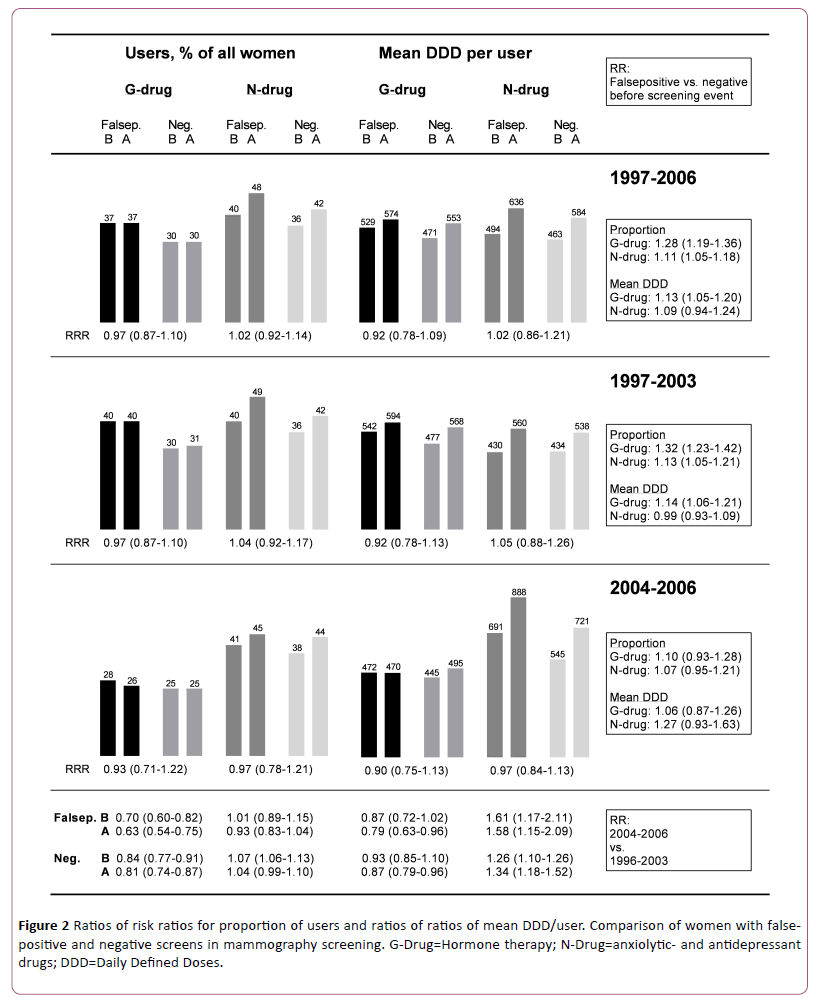
Figure 2: Ratios of risk ratios for proportion of users and ratios of ratios of mean DDD/user. Comparison of women with falsepositive and negative screens in mammography screening. G-Drug=Hormone therapy; N-Drug=anxiolytic- and antidepressant drugs; DDD=Daily Defined Doses.
Anxiolytic- and antidepressant drugs use, before the screening event versus after screening event
Women who later experienced a false-positive screening result also had a higher consumption of anxiolytic-and antidepressant drugs than women who later experienced a negative screening result; the RRs being 1.11 (95% CI 1.05-1.18) for the entire period 1997-2006, and 1.13 (95% CI 1.05-1.21) and 1.07 (95% CI 0.95-1.21) for 1997-2003 and 2004-2006, respectively. A difference in mean DDD derived exclusively from the late period with a RR of 1.27 (p=0.0594 for difference between means), Figure 2.
Hormone therapy use by time period
The proportion of users of hormone therapy changed statistically significantly from 1997-2003 to 2004-2006. For women in the false-positive group, the RR was 0.70 (95% CI 0.60-0.82) before their screening event and RR 0.63 (95% CI 0.54-0.75) after their screening event. This decline from 1997-2003 to 2004-2006 was significantly smaller for women in the negative group (p<0.001); the “before screening event” RR being 0.84 (95% CI 0.77-0.91), and the “after screening event” RR being 0.81 (95% CI 0.74-0.87), Table 2.
| |
Before screening event |
After screening event |
1997-03 |
2004-08 |
1997-08 |
| Type of mammography screen/ Drug type |
1997
-03 |
2004
-06 |
(2004
-06/
1996-03
RR,CI,p) |
1997
-06 |
1997
-03 |
2004
-08 |
(2004
-08/
1996-03
RR,CI,p) |
1997-
06 |
(After/
(Before;
RR,CI,p) |
(After/
(Before
RR,CI,p) |
(After/
(Before
RR,CI,p) |
| False positive |
|
|
|
|
|
|
|
|
|
|
|
| G – drugs, current use (G03C estrogens, G03D progestogens, and G03F a combination of estrogens and progestogens). |
| yes |
570 |
128 |
|
698 |
580 |
118 |
|
698 |
|
|
|
| no |
873 |
335 |
|
1208 |
863 |
345 |
|
1208 |
|
|
|
| % yes |
39.5 |
27.6 |
0.70
(0.60-0.82
)<0.0001 |
36.6 |
40.2 |
25.5 |
0.63
(0.54-0.75)
<0.0001 |
36.6 |
1.02
(0.93-1.11)
0.7038 |
0.94
(0.96-1.17)
0.5842 |
1.0
(0.92-1.09)
1.000 |
| N – drugs, current use (N02 analgesics, N05 psycholeptics, N06 psychoanaleptics, and N07 other nervous system drugs). |
| Yes |
580 |
188 |
|
768 |
705 |
210 |
|
915 |
|
|
|
| No |
863 |
275 |
|
1138 |
738 |
253 |
|
991 |
|
|
|
| % yes |
40.2 |
40.6 |
1.01
(0.89-1.15), 0.875 |
40.3 |
48.9 |
45.4 |
0.93
(0.83-1.04)
0.198 |
48.0 |
1.22
(1.12-1.32)
<0.0001 |
1.12
(0.96-1.30)
0.145 |
1.19
(1.11-1.28)
<0.0001 |
| Negative |
|
|
|
|
|
|
|
|
|
|
|
| G – drugs, current use (G03C estrogens, G03D progestogens, and G03F a combination of estrogens and progestogens). |
| yes |
2155 |
582 |
|
2737 |
2233 |
577 |
|
2810 |
|
|
|
| no |
5060 |
1733 |
|
6793 |
4982 |
1738 |
|
6720 |
|
|
|
| % yes |
29.9 |
25.1 |
0.84
(0.77-0.91)
<0.0001 |
28.7 |
30.9 |
24.9 |
0.81
(0.74-0.87)
<0.0001 |
29.4 |
1.04
(0.99-1.09)
<0.0001 |
0.99
(0.90-1.10)
0.8653 |
1.03
(0.98-1.07)
0.2444 |
| N-drugs, current use (N02 analgesics, N05 psycholeptics, N06 psychoanaleptics, and N07 other nervous system drugs). |
| yes |
2571 |
879 |
|
3450 |
3009 |
1008 |
|
4017 |
|
|
|
| no |
4644 |
1436 |
|
6080 |
4206 |
1307 |
|
5513 |
|
|
|
| % yes |
35.6 |
38.0 |
1.07
(1.00-1.13)
0.040 |
36.2 |
41.7 |
43.5 |
1.04
(0.99-1.10)
0.116 |
42.2 |
1.17
(1.12-1.22)
<0.0001 |
1.15
(1.07-1.23)
0.0001 |
1.16
(1.12-1.21)
<0.0001 |
Table 2: Number of women using drugs by mammography outcome, screening event, and prescription recommendation*. *Number of women using drugs by mammography outcome, time period in relation to the screening event, and time period in relation to recommendation for prescription of hormone therapy; ratio of risk ratios, 95% confidence interval and p-value. G-Drug=Hormone therapy; N-Drug=anxiolytic-and antidepressant drugs; DDD=Daily Defined Doses.
The mean DDD of hormone therapy decreased less and was statistically significant only for the “after” RRs being 0.79 (95% CI 0.63-0.96) for the false-positive group, and 0.87 (95% CI 0.79-0.96) for the negative group, Table 3.
| |
Before screening event |
After screening event |
1997
-03 |
2004
-06 |
1997
-06 |
| Type of mammography screen/ Drug type |
1997
-03 |
2004
-06 |
(Before
RR,CI,p) |
1997
-06 |
1997
-03 |
2004
-06 |
(After
RR,CI,p) |
1997
-06 |
(After/
(Before
RR,CI,p) |
(After/
(Before RR,CI,p) |
(After/
(Before
RR,CI,p) |
| False positive |
|
|
|
|
|
|
|
|
|
|
|
| G - drugs |
542.92 |
472.34 |
0.87
(0.72-1.02) |
529.97 |
594.61 |
470.61 |
0.79
(0.63-0.96) |
573.69 |
1.10
(1.01-1.19) |
1.00
(0.76-1.28) |
1.08
(1.00-1.17) |
| N-drugs |
430.29 |
691.07 |
1.61
(1.17-2.11) |
494.13 |
560.91 |
888.32 |
1.58
(1.15-2.09) |
636.05 |
1.30
(1.06-1.60) |
1.28
(0.89-1.85) |
1.29
(1.07-1.55) |
| Negative |
|
|
|
|
|
|
|
|
|
|
|
| G-drugs |
477.64 |
445.60 |
0.93
(0.85-1.01) |
470.82 |
568.02 |
495.50 |
0.87
(0.79-0.96) |
553.13 |
1.19
(1.13-1.25) |
1.11
(0.98-1.25) |
1.17
(1.12-1.23) |
| N-drugs |
434.34 |
545.52 |
1.26
(1.10-1.42) |
462.67 |
538.36 |
721.73 |
1.34
(1.18-1.52) |
584.37 |
1.24
(1.13-1.36) |
1.32
(1.13-1.54) |
1.26
(1.17-1.37) |
Table 3: Mean dose (DDD/woman) of drugs used by mammography outcome, screening event and prescription recommendation*. *Mean dose (DDD/woman) of drugs used by mammography outcome, time period in relation to the screening event, and time period in relation to recommendations for prescription of hormone therapy; ratio of risk ratios, 95% confidence interval and p-value. G-Drug=Hormone therapy; N-Drug=anxiolytic-and antidepressant drugs; DDD=Daily Defined Doses.
Anxiolytic- and antidepressant drugs use by time period
The proportion of users of anxiolytic-and antidepressant drugs did not change from 1997-2003 to 2004-2006 for women in the false-positive group; the RR in the “before” period was 1.01 (95% CI 0.89-1.15), and it was 0.93 (95% CI 0.83-1.04) in the “after” period. The changes in women in the negative group were borderline statistically significant, RR 1.07 (95% CI 1.00-1.13) in the “before” period, and 1.04 (95% CI 0.99-1.10) in the “after” period, Table 2.
However, the mean DDD of anxiolytic-and antidepressant drugs increased statistically significantly from 1997-2003 to 2004-2006 both in the false-positive group and in the negative group. In the false-positive group, the RR was 1.61 (95% CI 1.17-2.11) in the “before” period and 1.58 (95% CI 1.15-2.09) in the “after” period. In the negative group the RRs were 1.26 (95% CI 1.10-1.42) and 1.34 (95% CI 1.18-1.52), respectively, Table 3.
Discussion
We found no impact of a false-positive screening result on the use of hormone therapy and anxiolytic-and antidepressant drugs neither prior to nor after the EMEA recommendation on restrictive use of hormone therapy. Our previous results were therefore not confounded by changes in the drug prescription pattern over time.
We also found that women who later experienced a falsepositive result constituted a selected group. Prior to the EMEA recommendation, use of hormone therapy was 32% more frequent and use of anxiolytic- and antidepressant drugs 13% more frequent in women who later experienced a falsepositive result than in other women. While there was no difference between the users in the two groups of women in mean dose of anxiolytic- and antidepressant drugs prior to the EMEA recommendation, this difference came up to 27% afterwards.
We found that the EMEA recommendation was associated with a decreased use of hormone therapy but with an increased use of anxiolytic-and antidepressant drugs. In women who later experienced a false-positive result, use of hormone therapy decreased by 30% and by 16% in other women. While the EMEA recommendation was not associated with change in use of anxiolytic- and antidepressant drugs in women who later experienced a false-positive result, it was associated with a 7% increase in other women, and the mean dose in users increased with 61% in the false-positive group and with 26% in other women.
Since this population study was register-based, recall bias was not a problem. It was a strength of the study that the drug prescription data in the DNPR are comprehensive and valid [17]. The longitudinal record keeping enabled us to track drug consumption for each woman throughout the specified time frame, two years before and two year after the screening event. Certainly, drug prescription is not equivalent to actual consumption, but it is a reasonably good indicator, and this limitation applied equally to women in the false-positive and in the negative groups.
Between 38% and 45% of women were recorded with at least one prescription of anxiolytic-and antidepressant drugs during the latest two-year period in the years 2004 to 2006. This proportion might seem high. However, according to national statistics in a one-year period 2011 about 15% of women in our studied age-group used antidepressant drugs, and an additional 2% of new users were recorded in a year [18]. In Denmark, the antidepressant drugs constitute about half of the total consumption of anxiolytic-and antidepressant drugs [18]. On this basis the recorded use in the present study is well in line with national statistics.
Use of hormone therapy increases breast density, and breast density increases the risk of a false-positive screening result [19]. The excess use of hormone therapy seen in the present study in the false-positive group before their screening event was therefore an expected finding.
The excess use of anxiolytic- and antidepressant drugs in the false-positive group before their screening event is more difficult to explain. However, a study from the populationbased Saskatchewan Health records from 1981-1998, thus from before published side-effects of hormone therapy, revealed that in healthy women aged 45 years and above, users of hormone therapy were more likely also to use central nervous system drugs than were non-users [20]. The increased use of anxiolytic-and antidepressant drugs, especially in terms of increased doses, after the EMEA recommendation on restrictive use of hormone therapy, was supported by data from Sweden. According to the Swedish Prescribed Drug Register, women who discontinued use of hormone therapy between July 2005 and June 2009 were more likely to take up use of antidepressant treatment than were women who continued use of hormone therapy, incidence rate ratio 1.24 (95% CI 1.11-1.38) [21].
Estradiol therapy has been suggested for treatment of depression among peri-and early postmenopausal women [22], indicating that hormone therapy and anxiolytic-and antidepressant drugs may to a certain extent replace each other in the treatment of menopausal symptoms. It is noteworthy in our data, however, that the observed increase in doses of anxiolytic-and antidepressant drugs from the pre- EMEA recommendation period to the post-period were considerably larger than the observed decreases in doses of hormone therapy. For the false-positive group, it was a 61% increase versus a 13% decrease, and for the negative group a 26% increase versus a 7% decrease. In the post-EMEA recommendation period, users of anxiolytic-and antidepressant drugs in the false-positive group used on average almost one DDD per day for the entire two years prior to their false-positive screening result; increasing to more than one DDD per day during the two years after their screening event.
While elevated mental distress has commonly been perceived as a major side-effect of false-positive screening results, our findings indicated that the observed anxiety could probably to some extent be explained by pre-screening selective differences. Two years before the screening, the women who later experienced a false-positive result probably already had more psychological distress than women who later received a negative result. Before 2004, hormone therapy was to a certain extent used to alleviate these symptoms, while from 2004 onwards this role was in part taken over by the anxiolytic-and antidepressant drugs.
Conclusion
We found no impact of a false-positive screening result on use of anxiolytic- and antidepressant drugs, but we found that women who later experienced a false-positive screening result to some extent constituted a selected group with more users of these drugs even before their false-positive screening event, and the doses they used increased after the new restrictive EMEA recommendation for use of hormone therapy.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of Interest Statement
All authors declare no conflict of interest.
Ethics
Use of screening data and medical information was approved by the Danish Data Inspection Agency (2001-41-6191).
References
- European Commission (2006) European guidelines for quality assurance in breast cancer screening and diagnosis, 4th edition.
- Kemp, Jacobsen K, Abraham L, Buist DS, Hubbard RA, et al. (2015) Comparison of cumulative false-positive risk of screening mammography in the United States and Denmark. Cancer Epidemiol 39: 656-663.
- Hubbard RA, Miglioretti DL, Smith RA (2010) Modelling the cumulative risk of a false-positive screening test. Stat Methods Med Res 19: 429-449.
- Hubbard RA, Kerlikowske K, Flowers CI, Yankaskas BC, Zhu W, et al. (2011) Cumulative probability of false-positive recall or biopsy recommendation after 10 years of screening mammography: a cohort study. Annals of Internal Medicine 155: 481-492.
- Lauby-Secretan B, Scoccianti C, Loomis D, Benbrahim-Tallaa L, Bouvard V, et al. (2015) Breast-cancer screening—viewpoint of the IARC Working Group. New England Journal of Medicine 372: 2353-2358.
- Bond M, Pavey TG, Welch K, Cooper C, Garside Ret al. (2013) Systematic review of the psychological consequences of false-positive screening mammograms. Health Technol Assess 17: 1-169
- Brodersen J, Siersma VD (2013) Long-term psychosocial consequences of false-positive screening mammography. Ann Fam Med 11: 106-115.
- Davidsen A (2009) Mentalisering, narrativ og tid. En kvalitativ undersøgelse af psykologiske interventioner i almen praksis. Maanedsskrift for Praktisk Laegegerning 87: 124-131
- North American Menopause Society (2012) The 2012 hormone therapy position statement of the North American Menopause Society. Menopause (New York, NY) 19: 257.
- Writing Group for the Women's Health Initiative Investigators (2002) Risks and benefits of estrogen plus progestin in healthy postmenopausal women: principal results from the Women's Health Initiative randomized controlled trial. Jama 288: 321-333.
- Collaborative Group on Epidemiological Studies of Ovarian Cancer (2015) Menopausal hormone use and ovarian cancer risk: individual participant meta-analysis of 52 epidemiological studies. The Lancet 385: 1835-1842.
- Shumaker SA, Legault C, Kuller L, Rapp SR, Thal L, (2004) Conjugated equine estrogens and incidence of probable dementia and mild cognitive impairment in postmenopausal women: Women's Health Initiative Memory Study. Jama 291: 2947-2958.
- EMA (2003) EMEA public statement on recent publications regarding hormone replacement therapy. EMEA/33065/03
- Glass AG, Lacey JV Jr, Carreon JD, Hoover RN (2007) Breast cancer incidence, 1980-2006: combined roles of menopausal hormone therapy, screening mammography, and estrogen receptor status. J Natl Cancer Inst 99: 1152-1161
- Imai A, Matsunami K, Takagi H, Ichigo S (2013) New generation nonhormonal management for hot flashes. Gynecol Endocrinol 29: 63-66
- World Health Organization (2014) Definition and general considerations, Available from: https://www.whocc.no/ddd/definition_and_general_considera/ Accessed on March 10, 2014.
- Kildemoes HW, Sorensen HT, Hallas (2011) J. The Danish National Prescription Registry. Scand J Public Health 39(7 Suppl): 38-41.
- Medstat Denmark (2017) Medstat.dk, Available from: https://medstat.dk/ Accessed on April 14, 2015.
- Carney PA, Miglioretti DL, Yankaskas BC, Kerlikowske K, Rosenberg R, et al. (2003) Individual and combined effects of age, breast density, and hormone replacement therapy use on the accuracy of screening mammography. Ann Intern Med 138: 168-175.
- Csizmadi I, Collet JP, Boivin JF, Hanley JA, Benedetti A (2004) Health-related behavior and the use of hormone replacement therapy. Pharmacoepidemiol Drug Saf 13: 65-71.
- Citarella A, Andersen M, Sundstrom A, Bardage C, Hultman CM, et al. (2013) Initiating therapy with antidepressants after discontinuation of hormone therapy. Menopause 20: 146-151
- Soares CN, Almeida OP, Joffe H, Cohen LS (2001) Efficacy of estradiol for the treatment of depressive disorders in perimenopausal women: a double-blind, randomized, placebo-controlled trial. Arch Gen Psychiatry 58: 529-534.