Keywords
Pancreatitis; Chronic
Abbreviations
RCT randomized controlled trials
INTRODUCTION
Chronic pancreatitis (CP) affects between 0.4% and
5% of the adult population throughout the world [1]. In
the United States, chronic pancreatitis results in more
than 122,000 outpatient visits and more than 56,000
hospitalizations per year [2]. The etiology of CP is often
related to excess chronic alcohol and tobacco consumption
and in western countries, CP is typically observed in
young men between 36 and 55 years of age [3, 4]. The
pathogenesis of chronic pancreatitis is not well understood
and it is thought that chronic pancreatitis is due to
multiple predisposing factors including – toxic metabolic,
idiopathic, genetic and autoimmune - and therefore CP
is a difficult condition to manage. It is characterized by
progressive inflammation of the pancreas leading to
destruction of pancreatic parenchyma and pancreatic
ducts with subsequent development of fibrosis of the
main pancreatic duct [5]. The morphologic changes in the
pancreas are best visualized by endoscopic retrograde
cholangiopancreatography (ERCP) and Endoscopic
Ultrasound (EUS) [5]. However, with improvements in
the sensitivity and specificity of noninvasive imaging
modalities including CT and MRI, these modalities are
increasingly being used to make the diagnosis.
Clinically, the most common symptom associated with
chronic pancreatitis is recurrent or continuous pain. Pain is believed to be associated with increased pancreatic
duct pressure secondary to proximal ductal stenosis
with distal duct dilatation [6]. Other theories believed to
associate with the pain in chronic pancreatitis include
pancreatic ischemia, fibrosis, pseudocyst formation, and
inflammation [6]. Pancreatic duct stones contribute to
ductal hypertension by impeding pancreatic juice outflow,
and thus leading to continual pain.
Treatment modalities for chronic pancreatitis include
conservative therapy with analgesia, lifestyle and dietary
modifications, endotherapy, and surgery. Pain management
using analgesia is the mainstay of treatment for chronic
pancreatitis and can be combined with other treatment
modalities. Recently, published data suggests that early
surgical treatment for intractable pain in patients with
chronic pancreatitis helps preserve endocrine function and
improve pain control [7]. Alternative therapies including
celiac plexus block have also been used to alleviate pain
with limited success [8].
Endoscopic therapy and specifically endotherapy
(combined medical and endoscopic therapy) is a
treatment modality that utilizes ERCP with pancreatic
sphincterotomy, followed by extraction of stones with or
without the use of extracorporeal shockwave lithotripsy
(ESWL), placement of a pancreatic duct stent, and dilation
of pancreatic duct strictures [9]. Endotherapy works by
reducing intraductal hypertension, bypassing obstructed
stones, restoring lumen patency in symptomatic strictures,
and sealing main pancreatic duct disruption [9]. The aim
of endotherapy is to decompress the main pancreatic duct
(MPD) by performing complete stone clearance and ductal
drainage, leading to MPD diameter reduction.
Several studies have reported on the efficacy of
endotherapy as a first line treatment for CP pain but to
date there are limited well-controlled studies. The results
of the studies published on the use of endotherapy for
chronic pancreatitis pain report variable long-term pain
relief ranging between 32-92% [10, 11]. The wide range of
reported long term pain relief is likely due to a lack of welldesigned
studies and the heterogeneity of reported data.
The purpose of this systematic review and meta-analysis
is to evaluate the utility of endotherapy in the management
of pain associated with chronic pancreatitis. Specifically, we
seek to elucidate and determine effect of endotherapy on pain
relief associated with CP both immediately after treatment
and on long-term follow-up. We then compare the results to
published literature that evaluates the efficacy of alternative
treatment modalities such as surgery. We hope that this
systematic review and meta-analysis will help physicians
develop a better treatment algorithm that can be used to treat
patients suffering from persistent pain secondary to chronic
pancreatitis.
METHODS
A literature search of Medline with the PubMed
interface from January 1988 to December 2014 and EMBASE from 1980 to December 2014 with the Ovid
technologies interface was performed. Studies were
then analyzed for the use of endotherapy for pain relief
in chronic pancreatitis. We searched reference lists and
published abstracts from conference proceedings to
identify relevant trials.
We included large prospective studies, randomized
controlled trials (RCT) and retrospective analyses. We
included studied that reported immediate as well as longterm
benefits associated with endotherapy and its role
in pain management. Via a hand search, we also included
abstracts or unpublished data if sufficient information on
study design, characteristics of participants, interventions
and outcomes were available and if full information, as
well as final results, could be confirmed by contacting the
first author. The search was performed using keywords:
"Endotherapy in Chronic Pancreatitis Pain" [MeSH],
"Stent Therapy in Chronic Pancreatitis Pain" [MeSH],
and "Endoscopic Treatment in Chronic Pancreatitis Pain"
[MeSH]. The search results including the title and abstract
and all abstracts and manuscripts were reviewed by two
independent investigators (MJ, and JS).
Exclusion criteria in our analysis included studies not
written in the English language, small studies with less than
10 patients, and case series/case reports. Additionally,
studies that simultaneously enrolled patients in multiple
modalities of treatment such as endotherapy as well as
subsequent surgery or celiac plexus neurolysis were
also excluded. Each study was then carefully evaluated
for appropriate randomization, number of patients
enrolled, and method of diagnosis used to assess chronic
pancreatitis.
STATISTICAL ANALYSIS
Exact binomial confidence intervals were calculated
individually for each endpoint within each study. Forest
plots were constructed for each endpoint. We employed a
random-effects model meta-analysis in order to calculate a
pooled estimate of the proportion of patients experiencing
short-term and long-term pain relief following endoscopic
intervention. Heterogeneity was measured using I2
estimates. Funnel plots were also constructed in order to
assess for the possibility of publication bias. The statistical
analysis software used was Stata (version 12.0 College
Station, TX: StataCorp LP).
Overview of Included Studies and Details
Our initial search produced 420 potential articles. After
extensive review, 16 articles met our study criteria and
were selected (Figure 1). Of these 16 studies, eleven were
prospective and 4 were retrospective studies. Two studies
were randomized controlled trials comparing surgery
with endotherapy, while the remaining studies included
observational analyses.
Figure 1. Flow chart for search results. 420 studies met initial search
criteria and only 16 met inclusion criteria.
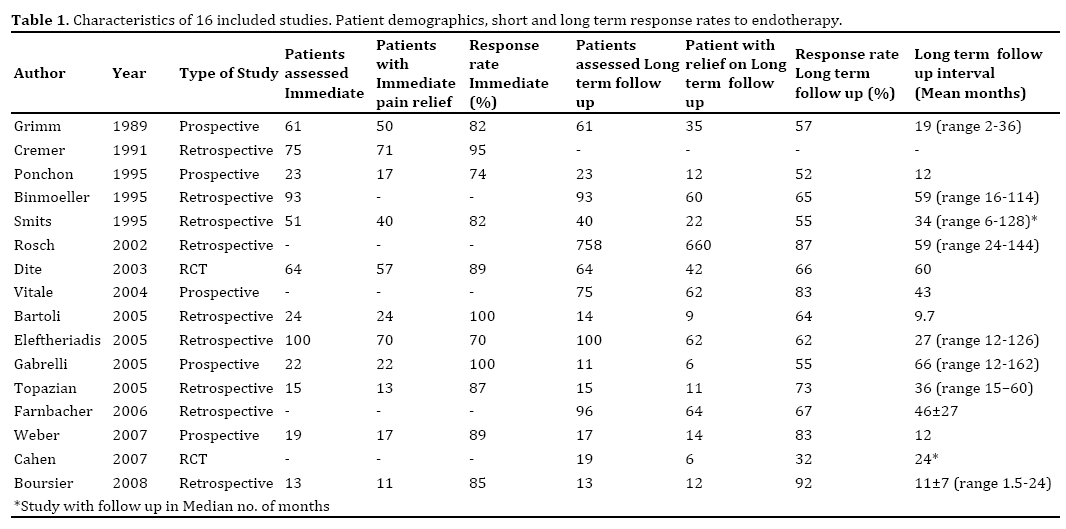
Our final data set included sixteen studies with a total
of 1498 patients (Table 1). This data was pooled and
aggregated. The primary endpoint assessed was pain relief immediately after endotherapy and pain relief at variable
long-term follow-up periods (range 1.5-162 months). The
most common scales used to assess pain included visual
analogue scale, Melzack and the Izbicki pain scale [10, 12].
Two studies used secondary endpoints, which included
weight gain and decreased use of narcotics, to gauge
therapeutic success [6, 11].
The procedural methods and materials used in
endotherapy were similar across the selected studies
(Table 2). Endotherapeutic procedures utilized in the
studies included pancreatic duct cannulation after which
a guide wire was maneuvered across the stricture. A
pancreatic sphincterotomy was frequently performed
to allow better drainage and easier instrumentation
and stent placement. There was variation in the type
of sphincterotomy performed, with some endoscopists
using the standard pull type and other using the needle
knife sphincterotomy and this was not reported in many
of the studies. Stricture dilatation with a graduated
dilating catheter or balloon dilator was utilized as needed.
Pancreatic stents were advanced over a guidewire
across the stricture using currently accepted methods.
Extracorporeal shockwave lithotripsy (ESWL) was variably
performed if large pancreatic stones were detected, via
externally-applied, focused, high-intensity acoustic pulse to
breakdown stones (Table 2) [9, 11, 12, 13, 14, 15, 16, 17].
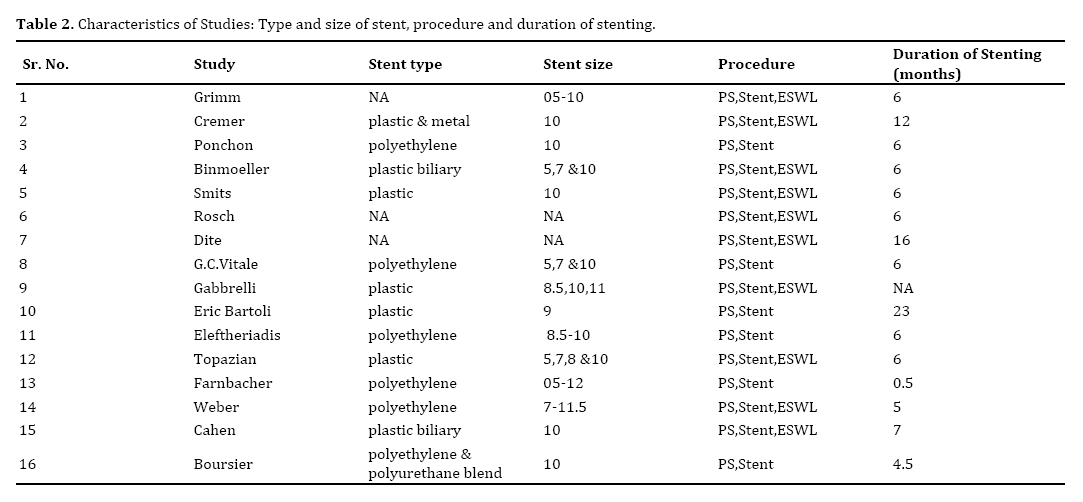
The characteristics of the stent used in the included
studies depended on the size and location of the pancreatic
duct stricture. The width of the stent placed varied across studies. If the pancreatic duct was small, typically a 4-7 Fr
stent was used, whereas if the pancreatic duct was dilated
a 10-11.5 Fr stent was used. Types of stents used included
Teflon [10, 12], polyethylene [6, 11, 13, 14, 15, 16, 17, 18, 19, 20, 21] and metallic stents [11] (Table 2).
The exchange schedule utilized included an on-demand
stent exchange schedule [13, 17, 20] and fixed exchange
schedule [4, 7, 8, 9, 18, 21, 22]. The on-demand stent
exchanges were based on symptomatic assessment of the
patients and stents were exchanged at the initial onset
of pain. While the fixed exchange schedule followed a
fixed, pre-determined interval, irrespective of symptoms.
Data regarding the number of stents placed during each
procedure was not included in the majority of the included
studies. The data regarding use of ERCP, EUS or both, was
lacking in the individual studies.
RESULTS
In this meta-analysis, the pooled estimate of the
proportion of subjects experiencing immediate pain relief
was 88% (95% CI [81.0%, 94.0%]) and the pooled estimate
of those with long-term relief was 67% (95% NT CI [58%,
76%]) (Figure 2). In the subgroup analysis of patients
with pancreatic duct strictures, we included nine studies,
comprising 536 patients. Seven studies included data
for immediate pain relief and eight studies reported
data evaluating sustained pain relief on follow-up. The
compiled results for the efficacy in immediate pain relief
is 74.7 % (95 NT CI [62.4%, 84.0%] while the results
for sustained pain relief is 67.5% (95 NT CI [51.5%,
80.2%]).
Figure 2. Forest plot showing pain relief at variable long-term follow when using endotherapy to treat CP pain.
Additionally, the compiled complication rate for
endotherapy in this review was 7.85% per ERCP/
endotherapeutic procedure and the most common
complications were acute pancreatitis, stent occlusion and
stent migration (Table 3).

A Subgroup analysis for 5 prospective studies and 2
randomized trials was also conducted. The prospective
studies showed a weighted mean for immediate pain relief
of 84.76% (95% NT CI [77%, 90%]) and weighted long term
pain relief of 68.9% (95% NT CI [61%, 74%]). The results
for the RCT subgroup revealed a weighted long term pain
relief of 58.2% (95% NT CI [47%, 68%]). Immediate pain
relief was not calculated in the RCT subgroup as there was
only one study that revealed this data.
The I² analysis was consistent with highly
heterogeneous data for both the immediate and long-term
follow-up intervals (I²=75.6% p<0.01, I²=88.1 p<0.01
respectively). In respect to the bias analysis, the Funnel
plot for pain relief on immediate follow-up (Figure 3)
does not demonstrate any obvious publication bias.
Figure 3. Funnel plot to assess for publication bias in immediate pain relief when using endotherapy for CPP.
The data for variable long term follow-up (Figure
4) does show evidence of some publication bias, with
the smaller studies showing less efficacy than the larger
studies.
Figure 4. Funnel plot to assess for publication bias in long-term pain relief when using endotherapy for CPP.
DISCUSSION
Chronic pancreatitis is characterized by an ongoing
inflammatory proves, leading to morphological changes
and pain within the pancreas. Although medical and
lifestyle modification is beneficial, including analgesics,
enzyme supplementation and antioxidant therapies, better
therapeutic approaches are needed to manage symptomatic
patients. Endotherapy is increasingly being used to manage
pain associated with chronic pancreatitis. It provides a less
invasive alternative to surgery. Endotherapy is becoming
an increasingly utilized option for the management of CPP.
This is in part due to technological advances and its less
invasive nature in comparison to alternate modalities of
treatment such as surgery.
According to the results in our systematic review and
meta-analysis, the compiled pain relief with endotherapy was 88% on immediate follow-up and 67% on long-term
follow-up. The results of our study shows that the pain
relief in our cohort is better than surgery, which has a
reported pain relief of 57-75% at long term follow-up [6, 7, 15, 16, 17]. Our results reinforce the use of endotherapy
as a viable first line therapeutic modality for CPP and our
pooled results are similar to that reported by other studies
[10, 12, 13, 14, 23, 24, 25, 26, 27, 28].
Endotherapy is becoming an increasingly utilized
option for the management of CPP. This is in part due to
technological advances and its less invasive nature in
comparison to alternate modalities of treatment such as
surgery.
pooled complication rate for endotherapy is 7.85%
which is lower than that reported for surgical management.
It has been reported that surgical intervention frequently has major complications associated with it, and these
complications requires further surgical intervention
in up to 10.9% of patients and that there are minor
complications in up to 28.3% of patients who undergo
surgery [22]. Because the high morbidity and mortality and
complication rate associated with surgery, endotherapy
is a suitable alternative. Studies have also shown that
endotherapy is associated with decreased anxiety and
is better tolerated especially in patients with additional
comorbidities including older age that make them poor
surgical candidates and preclude them from surgery [28].
Limitations of this meta-analysis include the small
number of published studies and the heterogeneous nature of
the published data. There are few well-designed studies and
less than five published randomized control trials compare
surgery versus endotherapy. Furthermore, the majorities of
the published studies are observational in nature and vary
in their methodological design. Amongst these studies, there
is also variation in pain assessment, selection of patients/
subjects, and differences in the size and type of stents used.
In addition, the published RCTs in the literature do not
mention if the statistical analyses used an intention to treat
analysis to correct for non-compliant patients, such as those
who continued to consume alcohol or when there was a nonrandom
loss of study participants. Finally, the studies vary in their exchange rates for stent replacement (i.e. some studies
use an on-demand schedule vs planned exchange schedule),
which may offer some explanation for the range in pain relief
on long-term follow-up.
Due to the heterogeneous nature of published studies,
we suggest that future studies be conducted to evaluate the
utility of endotherapy. Based on our analysis, we suggest
that these studies use similar analgesic regimens and quantify the daily dose and specific the narcotic used by
individuals before and after procedures (e.g. mg/day), as
this is not clearly stated in the current literature. With the
appropriate documentation, equianalgesic doses could be
calculated to assess the amount of pain medication needed
for pain resolution and allow for a more objective means
of grading the severity of pain. Additionally, subsequent
studies should attempt to use one standard method to grade pain. The subjective nature of pain scales makes comparing
scales such as VAS and Izbicki pain scales difficult and this
is also a limitation of our analysis. Furthermore, secondary
parameters such as weight-gain, hospital visits, and
decreased analgesic use should be universally adopted
in future studies to help gather more objective data to
assess clinical improvement. Another consideration
that may be of benefit is intermittent ethanol levels and
continued counseling being incorporated into each study,
since the major cause of CP in this cohort is alcohol abuse.
This would help assess if failed treatment was due to
procedural failure or a lack of lifestyle modifications on the
part of the patient. Furthermore, stent type and duration
of placement are all confounding variables that can be
resolved in subsequent studies by using the same type and
size (Fr) of stent if possible (polyethylene vs. metal) as well
as following the same exchange schedule (on-demand vs.
scheduled). Assessment of efficacy vis-a-vis pain relief at
long-term follow-up should be consistent. The range at
which patients were followed up varied across the studies
with a mean range from 9.7 months to 66 months. For
long-term studies, more frequent follow-up intervals can
be used to analyze intermediate-term efficacy [29, 30].
In conclusion, endotherapy is a safe and effective
therapeutic modality for the treatment of CPP. Its utility
appears to be best in the immediate period, but is reduced
on long-term follow up. It is less invasive and has fewer
complications, as compared to surgery which makes it
a viable primary treatment of choice. In patients who
have persistent CPP, endotherapy may act as a bridge to
surgery as it does not preclude any further interventions.
The significance of endotherapy is highlighted in patients
who respond initially to treatment and are saved from
undergoing unnecessary invasive procedures. This
may result in preserved endocrine function and lower
morbidity for the patient and ultimately reduce the overall
burden of expense on the healthcare system.
Conflict of Interest
The authors declare that they have no conflict of
interest.
References
- Kocher HM, Kadaba R. Chronic pancreatitis. BMJ Clin Evid 2011; 0417. [PMID: 22189345]
- Cecil R, Goldman L. Goldman's Cecil medicine (24th edtn). Philadelphia: Elsevier/Saunders 2012; 941.
- Durbec JP, Sarles H. Multicenter survey of the etiology of pancreatic diseases. Relationship between the relative risk of developing chronic pancreatitis and alcohol, protein and lipid consumption. Digestion 1978; 18:337-350. [PMID: 750261]
- Bartoli E, Delcenserie R, Yzet T, Brazier F, Geslin G, Regimbeau JM, Dupas JL. Endoscopic treatment of chronic pancreatitis. Gastroenterol Clin Biol 2005; 29:515-521. [PMID: 15980744]
- Axon AT, Classen M, Cotton PB, Cremer M, Freeny PC, Lees WR. Pancreatography in chronic pancreatitis: international definitions. Gut 1984; 25:1107-1112. [PMID: 6479687]
- Ponchon T, Bory RM, Hedelius F, Roubein LD, Paliard P, Napoleon B, Chavaillon A. Endoscopic stent placement for pain relief in chronic pancreatitis: results of a standardized protocol. Gastrointest Endosc 1995; 42:452-456. [PMID: 8566637]
- Sutherland DE, Radosevich DM, Bellin MD, Hering BJ, Beilman GJ, Dunn TB, Chinnakotla S, et al. Total pancreatectomy and islet transplantation for chronic pancreatitis. J AM Coll Surg 2012; 214:409-424. [PMID: 22397977]
- Kaufman M, Singh G, Das S, Concha-Parra R, Erber J, Micames C, Gress F. Efficacy of endoscopic ultrasound-guided celiac plexus block and celiac plexus neurolysis for managing abdominal pain associated with chronic pancreatitis and pancreatic cancer. J Clin Gastroenterol 2010; 44:127-134. [PMID: 19826273]
- Dumonceau JM, Devière J, Le Moine O, Delhaye M, Vandermeeren A, Baize M, Van Gansbeke D, et al. Endoscopic pancreatic drainage in chronic pancreatitis associated with ductal stones: long-term results. Gastrointest Endosc 1996; 43:547-555. [PMID: 8781931]
- Cahen DL, Gouma DJ, Nio Y, Rauws EA, Boermeester MA, Busch OR, Stoker J et al. Endoscopic versus surgical drainage of the pancreatic duct in chronic pancreatitis. N Engl J Med 2007; 356:676-684. [PMID: 17301298]
- Boursier J, Quentin V, Le Tallec V, Maurin A, Person B, O'Toole D, Boyer J. Endoscopic treatment of painful chronic pancreatitis: evaluation of a new flexible multiperforated plastic stent. Gastroenterol Clin Biol 2008; 32:801-805. [PMID: 18752911]
- Díte P, Ruzicka M, Zboril V, Novotný I. A prospective, randomized trial comparing endoscopic with surgical therapy for chronic pancreatitis. Endoscopy 2003; 35:553-538. [PMID: 12822088]
- Grimm H, Meyer WH, Nam VC, Soehendra N. New modalities for treating chronic pancreatitis, Endoscopy 1989; 21:70-74. [PMID: 2707174]
- Cremer M, Devière J, Delhaye M, Baize M, Vandermeeren A. Stenting in severe chronic pancreatitis: results of medium-term follow-up in 76 patients. Endoscopy 1991; 23:171-176. [PMID: 1860448]
- Binmoeller KF, Jue P, Seifert H, Nam WC, Izbicki J, Soehendra N. Endoscopic pancreatic stent drainage in chronic pancreatitis and a dominant stricture: long-term results. Endoscopy 1995; 27:638-644. [PMID: 8903975]
- Gabbrielli A, Pandolfi M, Mutignani M, Spada C, Perri V, Petruzziello L, Costamagna G. Efficacy of main pancreatic-duct endoscopic drainage in patients with chronic pancreatitis, continuous pain, and dilated duct. Gastrointest Endosc 2005; 61:576-581. [PMID: 15812411]
- Weber A, Schneider J, Neu B, Meining A, Born P, Schmid RM, Prinz C. Endoscopic stent therapy for patients with chronic pancreatitis: results from a prospective follow-up study. Pancreas 2007; 34:287-294. [PMID: 17414050]
- Eleftherladis N, Dinu F, Delhaye M, Le Moine O, Baize M, Vandermeeren A, Hookey Let al. Long-term outcome after pancreatic stenting in severe chronic pancreatitis. Endoscopy 2005; 37:223-230. [PMID: 18556820]
- Vitale GC, Cothron K, Vitale EA, Rangnekar N, Zavaleta CM, Larson GM, Binford J et al. Role of pancreatic duct stenting in the treatment of chronic pancreatitis. Surg Endosc 2004; 18:1431-1434. [PMID: 15791364]
- Topazian M, Aslanian H, Andersen D. Outcome following endoscopic stenting of pancreatic duct strictures in chronic pancreatitis. J Clin Gastroenterol 2005; 39:908-911. [PMID: 16208117]
- Farnbacher MJ, Mühldorfer S, Wehler M, Fischer B, Hahn EG, Schneider HT. Interventional endoscopic therapy in chronic pancreatitis including temporary stenting. Scand J Gastroenterol 2006; 41:111-117. [PMID: 16373284]
- Drake DH, Fry WJ. Ductal drainage for chronic pancreatitis. Surgery 1989; 105:131-140. [PMID: 2916177]
- Sarles JC, Nacchiero M, Garani F, Salasc B. Surgical Treatment of chronic pancreatitis. Am Journal of Surgery 1982; 144:317-321. [PMID: 7114369]
- Bradley EL 3rd. Long-term results of pancreatojejunostomy in patients with chronic pancreatitis. Am J Surg 1987; 153:207-213. [PMID: 3812895]
- Sandrasegaran K, Maglinte DD, Howard TJ, Lappas JC. Surgery for chronic pancreatitis: cross-sectional imaging of postoperative anatomy and complications. AJR Am J Roentgenol 2005; 184:1118-1127. [PMID: 15788582]
- Smits ME, Badiga SM, Rauws EA, Tytgat GN, Huibregtse K. Long-term results of pancreatic stents in chronic pancreatitis. Gastrointest Endosc 1995; 42:461-470. [PMID: 8566639]
- Elta GH. Is there a role for the endoscopic treatment of pain from chronic pancreatitis? N Engl J Med 2007; 356:727-729. [PMID: 17301304]
- Ammann RW, Muellhaupt B. The natural history of pain in alcoholic chronic pancreatitis. Gastroenterology 1999; 116:1132-1140. [PMID: 10220505]
- Rösch T, Daniel S, Scholz M, Huibregtse K, Smits M, Schneider T, Ell C, et al. Endoscopic treatment of chronic pancreatitis: a multicenter study 1000 patient with long-term follow-up. Endoscopy 2002; 34:765-771. [PMID: 12244496]
- Cahen DL, Gouma DJ, Laramée P, Nio Y, Rauws EA, Boermeester MA, Busch OR et al. Long-term outcomes of endoscopic vs surgical drainage of the pancreatic duct in patients with chronic pancreatitis. Gastroenterology 2011; 141:1690-1695. [PMID: 21843494]





