Case Blog - (2017) Volume 1, Issue 3
Elderly Male with Multiple Colonic Ulcers Diagnosed as Metronidazole Responsive Amebic Colitis
Nitin R Gaikwad*, Sudhir J Gupta and Amol R Samarth
Department of Gastroenterology, Government Medical College and Super Specialty Hospital, Nagpur, Maharashtra, India
*Corresponding Author:
Nitin R. Gaikwad
Department of Gastroenterology
Government Medical College and Super Specialty Hospital
Nagpur, Maharashtra
India
Tel: 91-0712-2750121
Fax : 091-0712-2746682
E-mail: nitin0217@yahoo.co.in
Received date: Aug 11, 2017; Accepted date: Sep 05, 2017; Published date: Sep 08, 2017
Citation: Gaikwad NR, Gupta SJ, Samarth AR (2017) Elderly Male with Multiple Colonic Ulcers Diagnosed as Metronidazole Responsive Amebic Colitis. J Clin Gastroenterol Hepatol Vol.1 No.3:24. doi: 10.21767/2575-7733.1000024
Abstract
A 72-year-old male presented with 1-month history of crampy abdominal pain, mild grade fever, loose stools without bleeding. There was no history of abdominal distension, vomiting, hematemesis, weight loss. Physical examination was unremarkable. Blood and stool investigations were within normal limits. Colonoscopy was done which showed multiple discrete round to oval ulcers of variable size ranging from 8 mm to 2 cm. distributed throughout the colon from anal verge up to the caecum. These ulcere were covered by yellowish white plaque.
Case Blog
A 72-year-old male presented with 1-month history of crampy abdominal pain, mild grade fever, loose stools without bleeding. There was no history of abdominal distension, vomiting, hematemesis, weight loss. Physical examination was unremarkable. Blood and stool investigations were within normal limits. Colonoscopy was done which showed multiple discrete round to oval ulcers of variable size ranging from 8 mm to 2 cm. distributed throughout the colon from anal verge up to the caecum. These ulcere were covered by yellowish white plaque (Figure 1).
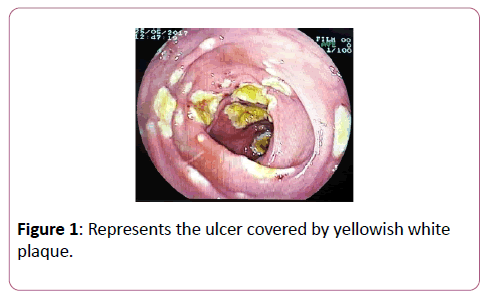
Figure 1: Represents the ulcer covered by yellowish white plaque.
Intermittent mucosa was normal and vascular pattern of the colonic mucosa was maintained. Biopsy from the ulcer (Figure 2) showed few bits of colonic mucosa with ulceration of lining epithelium. Lamina propria showed dense inflammatory infiltrate (Figure 3). And trophozoites of Entamoeba histolytica (Erythrophagocytosis) as shown by arrow in Figure 4. Patient was treated with Metronidazole for 2 weeks and repeat colonoscopy after one month showed complete healing of all the ulcers along with clinical improvement.
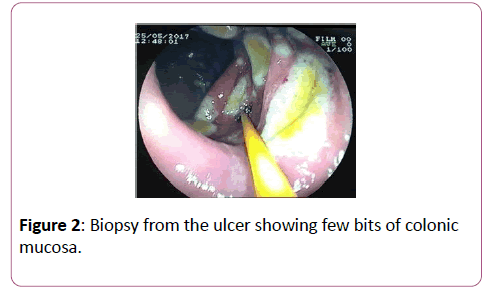
Figure 2: Biopsy from the ulcer showing few bits of colonic mucosa.
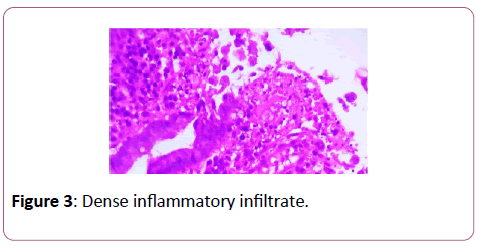
Figure 3: Dense inflammatory infiltrate.
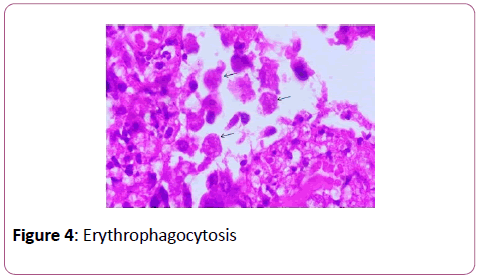
Figure 4: Erythrophagocytosis
This is a typical clinical presentation of amebic pancolitis. Differentials for whitish yellow plaque covered ulcers are NSAID enteropathy and pseudomembranous colitis [1]. The most reliable method for diagnosing intestinal amebiasis is the demonstration of the trophozoites on tissue biopsy [2] Treatment of choice is metronidazole or tinidazole [3]. The differential of amebic colitis should always be kept in mind when dealing with patients with diarrhea and typical colonoscopic findings especially in developing countries where prevalence of Amebiasis is more.
Conflict of Interest
None.
Consent
Informed consent was obtained from all the participants in this work.
Author contributions
Nitin Gaikwad did the colonoscopy and formulated the manuscript. Sudhir Gupta helped in literature search. Amol Samarth critically reviewed the manuscript.
References
- Nagata N, Shimbo T, Akiyama J, Nakashima R, Niikura R,et al. (2012) Predictive value of endoscopic findings in the diagnosis of active intestinal amebiasis. Endoscopy44:425–428.
- Tanuksel M, Petri WAJr. (2003) Laboratory diagnosis of amebiasis. ClinMicrobiol Rev16:713–729.
- Petri WA Jr., Singh U (1999) Diagnosis and management of amoebiasis. Clin Infect Dis 29:1117-1125.