Keywords
Endoscopy; Esophageal and Gastric Varices; Neoplasm Invasiveness; Pancreatic Neoplasms; Ulcer
Abbreviations
NSAID: nonsteroidal anti-inflammatory drug
INTRODUCTION
Pancreatic cancer is often complicated with upper gastrointestinal lesions. Lethal outcomes are sometimes encountered in daily practice. Upper gastrointestinal lesions related to pancreatic cancer have been reported in the English language literature [1, 2, 3, 4, 5, 6, 7, 8, 9]. However, there have been few reports of endoscopic studies in pancreatic cancer patients [2, 5, 9]. In addition, although the endoscopic findings at diagnosis have been reported previously [9], endoscopic upper gastrointestinal lesions that developed during the clinical course of pancreatic cancer have not been reported previously.
We investigated the upper gastrointestinal lesions in patients with pancreatic cancer who underwent upper gastrointestinal endoscopy.
METHODS
Patients
We encountered 112 patients with pancreatic cancer between 2003 and 2010. We retrospectively reviewed the upper gastrointestinal lesions in 75 patients who underwent upper gastrointestinal endoscopy. Patients consisted of 50 men and 25 women ranging in age from 29 to 89 (median 64) years. The tumor locations of the pancreatic cancer were the pancreatic head in 39 cases and the body and/or tail in 37 cases because one patient had two tumors, one in the pancreatic head and one in the body/tail. Clinical staging at diagnosis was Stage IB in 1 case (1.3%), Stage IIA in 2 cases (2.7%), Stage IIB in 3 cases (4.0%), Stage III in 24 cases (32.0%), and Stage IV in 45 cases (60.0%) according to the TNM classification, 6th edition [10]. Five patients (6.7%) with pancreatic cancer underwent pancreaticoduodenectomy or distal pancreatectomy. Sixty-nine patients (92.0%) were treated with chemotherapy by gemcitabine and/or S-1. Eighteen patients (24.0%) received radiotherapy combined with chemotherapy (gemcitabine and/or S-1) before or after chemotherapy.
Endoscopic Findings
We examined the incidence of upper gastrointestinal lesions, such as gastroduodenal invasion, ulcers, esophagogastric varices, radiation-induced gastroduodenal mucosal lesions, and portal hypertensive gastropathy. Gastroduodenal invasion was judged as erosion, ulcers, or stricture due to direct invasion of pancreatic cancer. In this study, extrinsic compression was excluded because the findings were indefinite between endoscopists and seldom susceptible to bleeding. Gastroduodenal ulcers were defined as ulcerative lesions except for direct invasion of pancreatic cancer. Esophagogastric varices and portal hypertensive gastropathy were diagnosed according to the General Rules for Recording Endoscopic Findings of Esophagogastric Varices (2nd edition) [11]. Radiation-induced gastroduodenal ulcers and gastritis were defined as ulcerative and reddish or erosive lesions post-radiotherapy, respectively. In this study, these conditions were termed radiation-induced gastroduodenal mucosal lesions.
The symptoms associated with gastrointestinal bleeding were defined as hematemesis, melena, and/or progression of anemia due to upper gastrointestinal lesions. The symptoms related to upper gastrointestinal lesions were defined as abdominal pain, nausea vomiting, and/or appetite loss in addition to the symptoms of gastrointestinal bleeding.
Upper gastrointestinal lesions were independently reviewed and verified by two experienced investigators. If the opinions were different between the two investigators, a consensus was reached by further discussion.
ETHICS
The written informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the “World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects” adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964 and amended by the 59th WMA General Assembly, Seoul, South Korea, October 2008, as reflected in a priori approval by our institutional review committee.
STATISTICS
Frequencies were used as descriptive statistics and the Pearson chi-square and the Fisher’s exact tests were applied. Statistical analyses were made by means of the Stat Mate (version IV, ATMS, Tokyo, Japan) statistical software. Two-tailed P values less than 0.05 were considered significant.
RESULTS
Total Findings
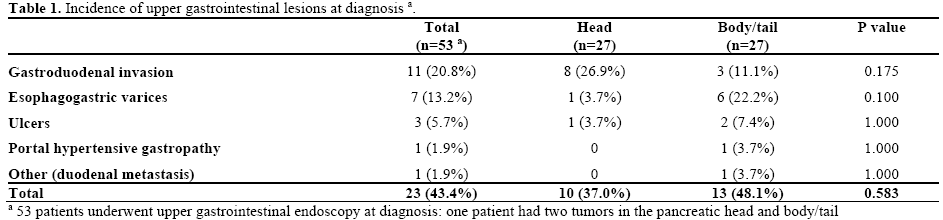
Of the 75 patients with pancreatic cancer, 53 (70.7%) underwent upper gastrointestinal endoscopy at diagnosis. In these 53 patients (54 tumors), 23 upper gastrointestinal lesions were observed in 20 patients (37.7%) (Table 1). Gastroduodenal invasion was observed in 11 (20.8%), esophagogastric varices in 7 (13.2%), and gastroduodenal ulcers in 3 (5.7%). Portal hypertensive gastropathy and duodenal metastasis were identified in one case each (1.9%).
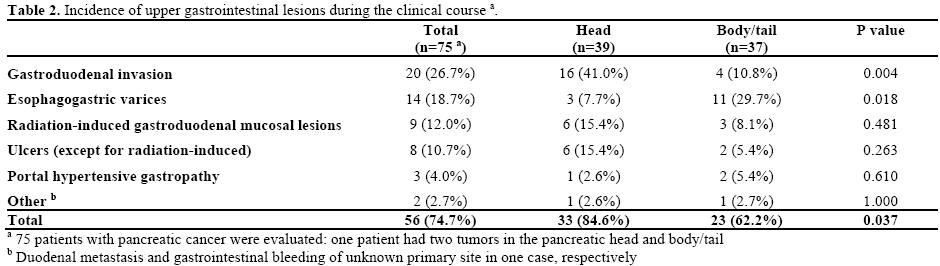
On the other hand, during the clinical course of pancreatic cancer in the 75 patients (76 tumors) with pancreatic cancer, 56 upper gastrointestinal lesions were observed in 46 patients (61.3%) (Table 2). Gastroduodenal invasion was observed in 20 patients (26.7%), esophagogastric varices in 14 (18.7%), radiation-induced gastroduodenal mucosal lesions in 9 (12.0%), gastroduodenal ulcers (except radiationinduced ulcers) in 8 (10.7%), and portal hypertensive gastropathy in 3 (4.0%). Duodenal metastasis and gastrointestinal bleeding of unknown primary site were identified in one patient each (1.3%).
Gastroduodenal Invasion
Gastroduodenal invasion was observed in the cases with lesions located in the pancreatic head significantly more frequently than in those located in the body and/or tail: 16 of 39 cases (41.0%) vs. 4 of 37 (10.8%) during the clinical course (P=0.004, Fisher’s exact test), although significant difference was not recognized at diagnosis (Tables 1 and 2; Figure 1). The involved organs were as follows: the stomach in 2 cases (10.0%), in which all tumors were located in the pancreatic body and/or tail; duodenal bulb in 2 cases (10.0%), in which all tumors were located in the pancreatic head; descending part of the duodenum in 13 cases (65.0%), in which all tumors were located in the pancreatic head; and horizontal part of the duodenum in 3 cases (15.0%), in which 1 and 2 tumors were located in the pancreatic head and body, respectively. Malignant cells were confirmed in 9 (52.9%) of 17 patients in whom endoscopic biopsy was performed. Although gastrointestinal bleeding has not been identified in patients with gastric invasion, that developed in 4 out of 18 patients with duodenal invasion (22.2%). One of these 4 patients died of repeated gastrointestinal bleeding.
Figure 1. Case of pancreatic head cancer with duodenal invasion.
Esophagogastric Varices
Unlike gastroduodenal invasion, esophagogastric varices were observed in the cases with lesions located in the pancreatic body and/or tail significantly more frequently than in those with lesions in the head (3 of 39 cases (7.7%) vs. 11 of 37 cases (29.7%) during the clinical course (P=0.018, Fisher’s exact test)), although significant difference was not recognized at diagnosis (Tables 1 and 2; Figure 2). The involved organs were as follows: the esophagus in 6 cases (42.9%), in which 2 tumors were located in the pancreatic head and 4 in the body and/or tail; stomach in 5 cases (35.7%), in which all tumors were located in the pancreatic body or tail; and both the esophagus and stomach in 3 cases (21.4%), in which 1 and 2 tumors were located in the pancreatic head and body, respectively. Gastric varices were found in 8 cases and were located in cardia in 1 case (12.5%), in fornix in 5 cases (62.5%), and both cardia and fornix in 2 cases (25.0%). Portal venous systems were invaded in all 14 patients with esophagogastric varices. The splenic vein was involved in all 11 patients with pancreatic body and/or tail cancer, but not in any of those with pancreatic head cancer. F1 varices were observed in 7 of the 14 patients (50.0%), and F2 varices in another 7 patients (50.0%), while no F3 varices were identified. The red color sign was detected in 5 of the 14 patients (35.7%). Only 2 patients with F2 varices and red color sign presented with bleeding from esophagogastric varices. Although 1 of these 2 patients received endoscopic injection sclerotherapy, he died of repeated gastrointestinal bleeding. The other patient did not receive endoscopic treatment because variceal bleeding was controlled conservatively. There were no patients in whom endoscopic treatment for esophagogastric varices without bleeding was performed.
Figure 2. Case of pancreatic head cancer with esophageal varices.
Radiation-Induced Gastroduodenal Mucosal Lesions
Thirteen (72.2%) of the 18 patients treated with radiotherapy underwent upper gastrointestinal endoscopy post-radiotherapy. Radiation-induced gastroduodenal ulcers developed in 5 (38.5%) of these patients (Figure 3). The involved organs were as follows: the stomach in 3 cases, in which 1 and 2 tumors were located in the pancreatic body and pancreatic head, respectively; duodenum in 1, in which the tumor was located in the pancreatic head; and both stomach and duodenum in 1, in which the tumor was located in the pancreatic head. In addition, radiationinduced gastritis developed in 4 patients (30.8%) in whom 2 tumors were located in the pancreatic head and 2 in the body. A total of 9 (50.0%) of the 18 patients suffered radiation-induced gastroduodenal mucosal lesions. All 9 patients with them received proton pump inhibitor (PPI; n=5) or histamine H2-receptor antagonist (H2 blocker; n=4) after radiotherapy. Upper gastrointestinal bleeding was observed in 3 (33.3%) out of these 9 patients (1 with gastric ulcer and 2 with gastritis). Upper gastrointestinal bleeding developed 3 weeks after radiotherapy in 1 patient with radiationinduced gastric ulcer, and 5 or 7 months after radiotherapy in 2 patients with radiation-induced gastritis. Argon plasma coagulation therapy was effective for hemostasis in 2 patients with radiationinduced gastritis (Figure 4ab). The other patient with radiation-induced ulcer did not receive endoscopic treatment because bleeding was controlled conservatively.
Figure 3. Case of pancreatic head cancer with radiation-induced
gastric ulcer.
Figure 4. a. Case of pancreatic head cancer with radiation-induced
gastritis. b. Argon plasma coagulation therapy was effective in this
case.
Gastroduodenal Ulcers
Of the 8 patients with gastroduodenal ulcers (except radiation-induced ulcers), the involved organs were as follows: the stomach in 4 cases (50.0%), in which 2 tumors were located in the pancreatic head and 2 in pancreatic body; and duodenum in 4 (50.0%), in which all tumors were located in the pancreatic head. Ulcers were induced by biliary drainage device in 3 cases (37.5%) (self-expandable metallic stent in 2, and endoscopic nasobiliary drainage in 1) and nonsteroidal anti-inflammatory drugs (NSAIDs) in 2 cases (25.0%); although 1 of the 2 patients with duodenal ulcer induced by NSAIDs was not treated with PPI or H2 blocker, the other patient received H2 blocker before the onset of ulcer. Helicobacter pylori infection was confirmed in 2 of the remaining 3 patients. Gastrointestinal bleeding was observed in 4 patients (50.0%) (1 by self-expandable metallic stent, 2 by NSAIDs, and 1 with Helicobacter pylori infection). Endoscopic clipping was effective for hemostasis in 1 patient with gastroduodenal ulcers (except radiation-induced ulcers). The other 3 patients did not receive endoscopic treatment because bleeding was controlled conservatively. In addition, 5 out of the 75 patients with pancreatic cancer had radiation-induced ulcers (6.7%); therefore, the total number of patients with gastroduodenal ulcers accounted to 13 cases (17.3%).
Portal Hypertensive Gastropathy
Portal hypertensive gastropathy was observed in 3 patients (4.0%) in whom tumor locations were the pancreatic head (n=1) and body (n=2). All three patients with portal hypertensive gastropathy also suffered from esophagogastric varices. All esophagogastric varices complicated with portal hypertensive gastropathy presented with F2 varices and red color sign. Upper gastrointestinal bleeding developed in 1 patient with portal hypertensive gastropathy. Although gastrointestinal bleeding was uncontrollable by medication (beta-blocker), percutaneous portal vein stent (10x60 mm; Luminexx®, BARD, Murray Hill, NY, USA) was effective for hemostasis of gastrointestinal bleeding.
Other Findings
One patient with pancreatic tail cancer was accompanied with duodenal metastasis (1.3%). In this case, a flat elevated lesion with ulceration was observed in the duodenal bulb, and the presence of malignant cells was confirmed.
Gastrointestinal bleeding from unknown primary site was identified in 1 patient with pancreatic head cancer (1.3%). He died of sudden gastrointestinal bleeding.
Symptoms Related to Upper Gastrointestinal Lesions
The incidences of symptoms related to upper gastrointestinal lesions were examined. Twenty-nine of 56 lesions (51.8%) presented with symptoms related to the lesions. The symptoms were observed in 12 (60.0%) of 20 patients with gastroduodenal invasion, 2 (14.3%) of 14 with esophagogastric varices, 8 (88.9%) of 9 with radiation-induced gastroduodenal mucosal lesions, 5 (62.5%) of 8 with gastroduodenal ulcers (except radiation-induced ulcers), 1 (33.3%) of 3 with portal hypertensive gastropathy, and 1 out of 1 with gastrointestinal bleeding from unknown primary site. The remaining patient with duodenal metastasis had no symptoms. The incidences of symptoms related to gastroduodenal invasion (60.0%) and radiation-induced gastroduodenal mucosal lesions (88.9%) were significantly higher than in esophagogastric varices (14.3%) (P=0.013 and P<0.001, respectively; Fisher’s exact test). Fifteen of 56 lesions (26.8%) were accompanied by upper gastrointestinal bleeding. Most of these patients received endoscopic therapy and/or blood transfusion. Gastrointestinal bleeding was observed in 4 (20.0%) of 20 patients with gastroduodenal invasion, 2 (14.3%) of 14 with esophagogastric varices, 3 (33.3%) of 9 with radiationinduced gastroduodenal mucosal lesions, 4 (50.0%) of 8 with gastroduodenal ulcers (except radiation-induced ulcers), 1 (33.3%) of 3 with portal hypertensive gastropathy. In addition, one patient had gastrointestinal bleeding from unknown primary site, while the remaining patient with duodenal metastasis had no gastrointestinal bleeding. There were no significant differences in the incidence of gastrointestinal bleeding between different upper gastrointestinal lesions (P=1.000, P=0.343, P0.137, and P=0.465, respectively) in comparison with esophagogastric varices. Three of 15 patients in whom bleeding was confirmed endoscopically (1 patient with duodenal invasion, 1 with esophagogastric varices, and 1 of unknown primary site) died of upper gastrointestinal bleeding. In addition, 2 patients in whom upper gastrointestinal endoscopy was not performed at hematemesis (1 patient with duodenal invasion, 1 with unknown primary site) died of upper gastrointestinal bleeding. No significant endoscopic abnormalities were found at diagnosis in 2 patients with gastrointestinal bleeding from unknown primary site. A total of 5 (6.7%) of the 75 patients died of upper gastrointestinal bleeding.
New Upper Gastrointestinal Lesions
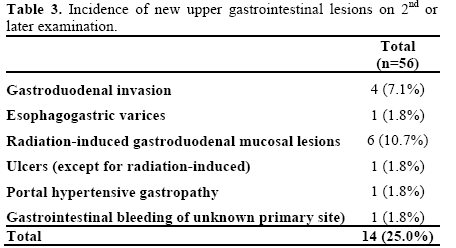
As shown in Table 3, new upper gastrointestinal lesions on second or later examinations were observed in 14 (25.0%) of the 56 upper gastrointestinal lesions during the clinical course of pancreatic cancer: 4 cases with gastroduodenal invasion, 1 with esophagogastric varices, 6 with radiation-induced gastroduodenal mucosal lesions, 1 with duodenal ulcer (except radiation-induced ulcers), 1 with portal hypertensive gastropathy, and 1 with gastrointestinal bleeding from an unknown primary site.
DISCUSSION
Upper gastrointestinal lesions related to pancreatic cancer have been reported in the English language literature [1, 2, 3, 4, 5, 6, 7, 8, 9]. However, there have been few endoscopic studies in pancreatic cancer patients [2, 5, 9]. In addition, although the endoscopic findings at diagnosis have been reported previously [9], endoscopic upper gastrointestinal lesions that developed during the clinical course of pancreatic cancer have not been reported previously. In the present study, we investigated the upper gastrointestinal lesions in patients with pancreatic cancer who underwent upper gastrointestinal endoscopy.
Gastroduodenal invasion complicated with pancreatic cancer has been reported [1, 2, 3, 4, 6]. In a previous study, gastric invasion was observed in 20 (27%) and duodenal invasion was observed in 30 (40%) of 75 patients with pancreatic cancer at autopsy [1]. In another autopsy report, gastric invasion was observed in 9 (7%) and duodenal invasion in 51 (37%) of 138 patients [4]. However, there have been few endoscopic reports regarding gastroduodenal invasion as a complication of pancreatic cancer [2, 6]. In the present study, gastroduodenal invasion was observed in 11 (21%) of 53 patients at diagnosis, and 20 (27%) of 75 patients during the clinical course of pancreatic cancer. The high incidence of gastroduodenal invasion at autopsy is assumed to be correlated with the progressive state of pancreatic cancer in most cases. In the present study, gastroduodenal invasion developed in patients with pancreatic cancer located in the pancreatic head at a significantly higher rate than in those with lesions in the pancreatic body and/or tail. It is assumed that pancreatic head cancer is prone to invade the duodenum, because the pancreas adjoins the duodenum and the duodenal wall is thinner than the gastric wall. It has been reported that patients with pancreatic cancer often develop gastrointestinal bleeding due to direct tumor invasion into the gastrointestinal tract [2, 3, 6]. In the present study, upper gastrointestinal bleeding developed in 4 patients with duodenal invasion. Gastrointestinal bleeding was uncontrollable in 1 of these 4 patients and resulted in death. Gastrointestinal bleeding due to direct tumor invasion is thought to be a critical complication in the patients with pancreatic cancer.
Esophagogastric varices as a complication of pancreatic diseases have been reported previously [5, 7, 8, 9]. The mechanism underlying the development of esophagogastric varices is assumed to entail involvement of the splenic vein by pancreatic disease, a manifestation called left-sided portal hypertension [12]. In endoscopic studies, it was reported that esophagogastric varices were observed by endoscopic ultrasonography in 16 patients (21%) with pancreatic diseases (pancreatic tumors in 12 and pancreatitis in 4) of 76 patients in whom gastroesophageal varices were detected endoscopically [5]. In another endoscopic study, esophagogastric varices were found in 25 (26%) patients with pancreatic cancer among 96 patients who underwent upper gastrointestinal endoscopy at diagnosis [9]. This previous study indicated that esophagogastric varices tended to be observed in patients with pancreatic body and/or tail cancer more frequently in those with pancreatic head cancer. In the present study, esophagogastric varices were observed in patients with pancreatic body and/or tail cancer at significantly higher rates than in those with pancreatic head cancer. It is assumed that the splenic vein is more susceptible to invasion by pancreatic body and/or tail cancer than pancreatic head cancer. In the present study, although the red color sign was observed in about one third of the patients with esophagogastric varices, no F3 varices were identified. In addition, upper gastrointestinal bleeding developed in only 2 (14.3%) of 14 patients, although 1 patient died of repeated GI bleeding. We speculated that segmental portal hypertension in patients with pancreatic cancer is reduced by flow from the short gastric or gastroepiploic vein to the portal vein (hepatopetal route) in contrast to liver cirrhosis (hepatofugal route). In this study, portal hypertensive gastropathy developed in 3 patients with pancreatic cancer. Portal hypertensive gastropathy related to pancreatic cancer has not been reported previously. Upper gastrointestinal bleeding developed in 1 patient with portal hypertensive gastropathy, resulting in hemostasis by percutaneous portal vein stent.
Although radiation-induced gastroduodenal mucosal lesions with pancreatic cancer have been reported, the incidence is relatively low [13, 14]. However, a total of 9 (50%) of the 18 patients who were treated with radiotherapy suffered from radiation-induced mucosal lesions in this study. It was assumed that long-term follow-up and frequent upper gastrointestinal endoscopy at digestive symptoms may have influenced the high prevalence in this study. Although all 9 patients with radiation-induced gastroduodenal mucosal lesions have been treated with PPI or H2 blockers since radiotherapy, upper gastrointestinal bleeding developed in 2 patients with radiation-induced gastritis 5 or 7 months after radiotherapy, resulting in hemostasis by argon plasma coagulation therapy. Therefore, attention should be paid to late-onset upper gastrointestinal bleeding in patients treated with radiotherapy. It is assumed that PPI or H2 blockers would be insufficient to prevent radiation-induced mucosal lesions.
There have been few previous reports of studies regarding gastroduodenal ulcers complicated with pancreatic cancer. In the present study, a total of 8 cases with gastroduodenal ulcers (except radiationinduced ulcers) were observed. In addition to 5 patients with radiation-induced ulcers, a total of 13 cases of gastroduodenal ulcers were identified. Although 2 patients developed NSAID-induced gastroduodenal ulcers, they were not treated with PPI (1 patient was treated with H2 blocker). PPI may have prevented gastroduodenal ulcers in these patients. In this study, although gastroduodenal ulcers were observed in only 3 patients at diagnosis, 10 lesions were newly identified especially in patients treated with radiotherapy, biliary drainage, or NSAIDs. Therefore, gastroduodenal ulcers should be considered in patients with pancreatic cancer receiving these therapies during the clinical course.
In the present study, about half of the upper gastrointestinal lesions presented with symptoms related to upper gastrointestinal lesions especially in patients with gastroduodenal invasion, radiationinduced gastroduodenal mucosal lesions, and gastroduodenal ulcers (except radiation-induced ulcers). Upper gastrointestinal bleeding as a complication of pancreatic cancer has been reported previously [2, 3, 6, 7, 8]. In this study, 15 (27%) of 56 lesions were accompanied by upper gastrointestinal bleeding. Most of upper gastrointestinal bleeding was controlled by endoscopic or conservative treatment. However, 3 of 15 patients in whom bleeding was confirmed endoscopically died of upper gastrointestinal bleeding. In addition to 2 patients in whom upper gastrointestinal endoscopy was not performed at hematemesis, a total of 5 (7%) of 75 patients died of upper gastrointestinal bleeding. Therefore, attention must be paid regarding upper gastrointestinal bleeding in patients with pancreatic cancer. When upper gastrointestinal bleeding occurs or is suspected during follow-up of pancreatic cancer, upper gastrointestinal endoscopy should be performed promptly. Although progression of anemia often develops in patients with pancreatic cancer due to bone marrow suppression by chemotherapy or secondary anemia, upper gastrointestinal endoscopy is recommended for evaluation of upper gastrointestinal bleeding in cases in which anemia has developed.
In this study, 14 (25%) of 56 upper gastrointestinal lesions were observed on the second or later examination. In particular, gastroduodenal invasion and radiation-induced gastroduodenal mucosal lesions were predominant in these cases. Therefore, attention should be paid to patients in whom pancreatic tumors have enlarged or radiotherapy has been performed.
The survival period of patients with pancreatic cancer has been prolonged due to the development of gemcitabine [15] and S-1 [16]. Therefore, the appearance of upper gastrointestinal lesions during the clinical course of pancreatic cancer is predicted to increase. In addition, clinical symptoms related to upper gastrointestinal lesions would be often masked by NSAIDs or opioid in patients with pancreatic cancer. It is proposed that upper gastrointestinal endoscopy may be recommended in patients with pancreatic cancer at diagnosis and in whom pancreatic tumors have enlarged or radiotherapy has been performed, and should be performed in patients in whom upper gastrointestinal bleeding is suspected of.
In conclusion, the incidence of upper gastrointestinal lesions in patients with pancreatic cancer was relatively high. In addition, the incidence increased with the clinical course of pancreatic cancer. We should pay attention to upper gastrointestinal lesions in patients with pancreatic cancer. In particular, when the symptoms associated with upper gastrointestinal bleeding are observed, upper gastrointestinal endoscopy should be performed promptly.
Conflict of interest
The authors have no conflict of interest
References
- Cubilla A, Fitzgerald PJ. Pancreas cancer. I. Duct adenocarcinoma. A clinical-pathologic study of 380 patients. Pathol Annu 1978; 13 Pt 1: 241-89. [PMID 214741]
- Sharon P, Stalnikovicz R, Rachmilewitz D. Endoscopic diagnosis of duodenal neoplasms causing upper gastrointestinal bleeding. J Clin Gastroenterol 1982; 4: 35-8. [PMID 6978900]
- Lee P, Sutherland D, Feller ER. Massive gastrointestinal bleeding as the initial manifestation of pancreatic carcinoma. Int J Pancreatol 1994; 15: 223-7. [PMID 7930783]
- Mao C, Domenico DR, Kim K, Hanson DJ, Howard JM. Observations on the developmental patterns and the consequences of pancreatic exocrine adenocarcinoma. Findings of 154 autopsies. Arch Surg 1995; 130: 125-34. [PMID 7848081]
- Tio TL, Kimmings N, Rauws E, Jansen P, Tytgat G. Endosonography of gastroesophagealvarices: evaluation and followup of 76 cases. Gastrointest Endosc 1995; 42: 145-50. [PMID 7590050]
- Tomita H, Osada S, Matsuo M, Shimokawa K. Pancreatic cancer presenting with hematemesis from directly invading the duodenum: report of an unusual manifestation and review. Am Surg 2006; 72: 363-6. [PMID 16676866]
- Mullan FJ, McKelvey ST. Pancreatic carcinoma presenting as bleeding from segmental gastric varices: pitfalls in diagnosis. Postgrad Med J 1990; 66: 401-3. [PMID 2371194]
- Smith TA, Brand EJ. Pancreatic cancer presenting as bleeding gastric varices. J Clin Gastroenterol 2001; 32: 444-7. [PMID 11319321]
- Shirato I, Nakamura S, Mitsunaga A, Shiratori K. Clinical features of esophago-gastric varices caused by pancreatic cancer (in Japanese with English abstract). Nippon Shokakibyo Gakkai Zasshi (JJSG) 2008; 105: 1186-92. [PMID 18678994]
- Sobin LH, Christian W. UICC. TNM classification of malignant tumours. 6th ed. New York, Wiley-Liss, 2002.
- Tajiri T, Yoshida H, Obara K, et al. General rules for recording endoscopic findings of esophagogastricvarices (2nd edition). Dig Endosc 2010; 22: 1-9. [PMID 20078657]
- Turrill FL, Mikkelsen WP. ‘’Sinistral’’ (left-sided) extrahepatic portal hypertension. Arch Surg 1969; 99: 365-8. [PMID 5306330]
- Okusaka T, Ito Y, Ueno H, et al. Phase II study of radiotherapy combined with gemcitabine for locally advanced pancreatic cancer. Br J Cancer 2004; 91: 673-7. [PMID 15226765]
- Wilkowski R, Thoma M, Bruns C, Wagner A, Heinemann V. Chemoradiotherapy with gemcitabine and continuous 5-FU in patients with primary inoperable pancreatic cancer. JOP 2006; 7: 349-60. [PMID 16832132]
- Burris HA 3rd, Moore MJ, Andersen J, et al. Improvements in survival and clinical benefit with gemcitabine as first-line therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15: 2403-13. [PMID 9196156]
- Ueno H, Okusaka T, Ikeda M, Takezako Y, Morizane C. An early phase II study of S-1 in patients with metastatic pancreatic cancer. Oncology 2005; 68: 171-8. [PMID 16006754]





