Keywords
Pancreatitis, Chronic; Endosonography; Cholangiopancreatography, Magnetic Resonance; Camostat; Pancrelipase
Abbreviations
CM camostat mesilate; FD functional dyspepsia; MPD main pancreatic duct; NAECP non-alcoholic early chronic pancreatitis; PBM pancreaticobiliary maljunction; PD pancreatic divisum
INTRODUCTION
Chronic pancreatitis (CP) is considered an irreversible
progressive chronic inflammatory disease. In addition
to pain, patients subsequently develop exocrine and
endocrine insufficiencies.
Major risk factors predisposing to CP have been
categorized using the TIGAR-O classification as (1) toxicmetabolic
(e.g. alcohol consumption, hypercalcemia, and
dyslipidemia), (2) idiopathic, (3) genetic, (4) autoimmune,
(5) recurrent and severe acute pancreatitis, and (6) obstructive (e.g. pancreatic divisum (PD) and sphincter
of Oddi disorders) [1]. Main etiology of non-alcoholic CP
includes idiopathic, genetic, and obstructive. In Japan, alcohol
consumption (69.7%) was the most frequent cause of CP,
followed by idiopathic CP (21.0%), although the latter is the
most frequent cause of CP in Japanese females [2].
Although advanced stage CP can be diagnosed easily,
the clinical diagnosis of early stage CP remains difficult.
The concept of early chronic pancreatitis (ECP) was
initially defined in the 2009 Japanese diagnostic criteria
for CP [3]. These criteria include the use of endoscopic
ultrasonography (EUS) as the diagnostic modality to
detect ECP. Early diagnosis and therapeutic intervention
may improve the long-term prognosis of CP patients. The
criteria include: (i) characteristic imaging findings, (ii)
characteristic histological findings, (iii) repeated upper
abdominal pain, (iv) abnormal levels of pancreatic enzymes
in serum and/or urine, (v) abnormal pancreatic exocrine
function, and (vi) continuous heavy drinking of alcohol
equivalent to ≥80 g/day pure alcohol [3]. Imaging findings
diagnostic of ECP on EUS included more than two of the
following seven features, with at least one of features 1–4:
(1) lobularity with honeycombing, (2) lobularity without
honeycombing, (3) hyperechoic foci without shadowing, (4) strands, (5) cysts, (6) dilated side branches, and (7)
hyperechoic main pancreatic duct (MPD) margin, or
irregular dilatation of more than three duct branches on
endoscopic retrograde cholangiopancreatography (ERCP).
ECP was diagnosed in patients with more than two of
items iii–vi, above, along with imaging findings, and was
suspected in patients with item iii or iv, along with imaging
findings, but only after ruling out other pancreatic diseases.
CT shows stones in the pancreatic ducts, pancreatic
calcification, MPD dilatation, and parenchymal atrophy
in patients with advanced stage CP [3, 4, 5], suggesting
that CT is useful for the diagnosis of advanced stage CP
[4, 5]. MRI has been reported to be more sensitive than
CT for the assessment of CP because MRI detects not
only morphological changes but the presence of fibrosis
[6, 7]. The Cambridge classification, in which CP was
graded by pancreatography, was proposed in 1984 [8].
ERCP classifications include side-branch pathology not
previously noted on CT, an earlier feature of the disease
[9]. However, pancreatography has been reported to
provide poor diagnostic accuracy in patients with mild CP
as compared with EUS [10, 11].
EUS has been reported useful for the diagnosis of CP
[11, 12, 13, 14, 15]. According to traditional criteria, CP was
graded by the number of EUS findings and compared with
the Cambridge classification of pancreatography results
[11, 13, 14]. However, discrepancies in diagnosing CP were
observed because of the differences in severity of EUS
findings, such as calcification and strands. New EUS-based
criteria for the diagnosis of CP (Rosemont classification)
were proposed in 2009, in which CP was graded by the
severity of EUS findings [10]. Based on the Rosemont
classification, ECP was newly defined in the 2009 Japanese
diagnostic criteria for CP [3].
Evidence-based 2015 clinical practice guidelines for
CP have indicated that the priority in the compensated
phase should be to prevent repeated relapses and pain
[16]. This includes dietary therapy to prevent excessive
stimulation of the pancreas and pharmacotherapy,
primarily with protease inhibitors. Elemental diets were
also recommended for pain management in patients with
CP [16, 17].
The clinical features of non-alcoholic ECP (NAECP) have
not been sufficiently known. This study retrospectively
investigated clinical features of NAECP.
PATIENTS AND METHODS
Among the 818 patients who underwent EUS between
2007 and 2015 in our hospital and were not heavy drinkers,
five (i.e. Patients 1, 5, 6, 11 and 13) were diagnosed with
NAECP and eight (i.e. Patients 2, 3, 4, 7, 8, 9, 10 and 12)
were suspected of having NAECP in the 2009 Japanese
diagnostic criteria for CP [3] (Table 1).

The clinical features of these 13 patients were
retrospectively reviewed. Baseline factors evaluated
included symptoms (upper abdominal pain and back pain); serum levels of pancreatic enzymes (amylase
(normal range, 40-113 IU/L), lipase (normal range, 11-
53 IU/L), and Elastase-I (normal range, <300 ng/dL));
imaging findings on EUS, computed tomography (CT), and
magnetic resonance imaging (MRI)/magnetic resonance
cholangiopancreatography (MRCP). Treatment-associated
factors included changes in symptoms, serum levels of
pancreatic enzymes and EUS results.
ETHICS
The written informed consent was obtained from
each patient and the study protocol conforms to the
ethical guidelines of the “World Medical Association
Declaration of Helsinki - Ethical Principles for Medical
Research Involving Human Subjects” adopted by the 18th
WMA General Assembly, Helsinki, Finland, June 1964 and
amended by the 59th WMA General Assembly, Seoul, South
Korea, October 2008, as reflected in a priori approval by
our institutional review committee.
RESULTS
The 13 patients included two men and 11 women,
of mean age 50.5 years (range, 26–75 years), with five
being <40 years old. All 13 patients denied being heavy
consumers of alcohol. The mother of Patient 10 had
recurrent pancreatitis, suggesting that Patient 10 had
familial pancreatitis, although genetic examination was not
performed. MRCP and ERCP diagnosed pancreaticobiliary
maljunction (PBM) in Patient 1 and PD in Patient 11
as described below. Etiologically, these factors were
regarded as responsible for CP in Patients 1, 10, and 11.
In contrast, the remaining 10 patients were suspected of
having idiopathic CP (Table 1).
Twelve (92%) patients presented with upper
abdominal pain, including 10 (77%) with accompanying
back pain. These symptoms were exacerbated by fat diet
and overeating. Eleven patients (i.e. all but Patients 2 and
13) presented at the hospital because of upper abdominal
and/or back pain. None of the 13 patients presented with
steatorrhea due to pancreatic exocrine insufficiency.
Concentrations of three pancreatic enzymes (amylase,
lipase, and Elastase-I) were measured in patient serum
as listed in Table 1. At least one enzyme was elevated in
seven (54%) patients. None of these 13 patients, however,
showed decreased pancreatic enzymes in serum, and
none underwent test of pancreatic exocrine function,
para-aminobenzoic acid (BT-PABA) test. None of these 13
patients was diagnosed with diabetes mellitus.
EUS findings of normal pancreas, calcified alcoholic
pancreatitis, and ECP are shown in Figure 1, respectively.
EUS showed lobularity with honeycombing in one patient
(8%), lobularity without honeycombing in seven (54%),
hyperechoic foci without shadowing in 10 (77%), strands
in 13 (100%), and hyperechoic MPD margin in 11 (85%) of
13 patients with ECP in this study. Three patients each had
two findings of these EUS criteria, four each had three, and six
each had four, respectively. None of these patients had cysts, side branches, hyperechoic foci with shadowing, MPD calculi,
irregular MPD contours, or MPD dilatation (Table 2).
Figure 1: Endoscopic ultrasonographic (EUS) findings in pancreatic body/tail. Normal pancreas, showing (a). homogenous and finely reticular pattern in parenchyma, (b). no dilatation of main pancreatic duct (MPD) (arrow) and side branches, and no hyperechoic MPD margin. Calcified alcoholic pancreatitis, showing (c). pancreatic stones (arrowheads) and lobular out gland margin (arrows). Early chronic pancreatitis (ECP), showing (d). lobularity without honeycombing (circle), (e). hyperechoic foci without shadowing (arrows), (f). strands (arrows), and (g). hyperechoic MPD margin (arrows).

None of these 13 patients showed definitive
abnormalities in the pancreatic parenchyma and
pancreatic ducts on contrast-enhanced CT. Eight patients
underwent MRI, which showed normal signal intensity
in the pancreas on fat-suppressed T1 and T2-weighted
images and uniform enhancement on the capillary phase.
Although MRCP showed no irregular dilatation of MPD
and side branches, it presented with findings indicative of
PBM (Patient 1) and PD (Patient 11) in one patient each,
respectively (Figure 2a, b). PBM was confirmed by ERCP
in Patient 1 (Figure 2c), who underwent prophylactic
cholecystectomy for the risk of gallbladder cancer.
Figure 2: (a). Magnetic resonance cholangiopancreatography (MRCP), showing a pancreaticobiliary maljunction (PBM) (arrow). (b). MRCP showing pancreatic divisum. Also observed was a dominant dorsal pancreatic duct (Santorini duct) crossing the lower bile duct (arrow). (c). Endoscopic retrograde cholangiopancreatography (ERCP) showing abnormal union between the pancreatic and bile ducts (common bile duct flowing to main pancreatic duct),
suggesting PBM (arrow).
Twelve patients were initially treated with the
protease inhibitor, camostat mesilate (CM; 300~600 mg/
day). Eight patients were secondarily administered the
antispasmolytic agent flopropion (120~240 mg/day), but
four patients discontinued due to lack of efficacy or adverse
events, such as thirst or constipation. Six patients received
conventional pancreatic enzymes secondarily; due to lack
of efficacy, four patients were switched to the high titer
pancreatic enzyme pancrelipase, and two patients were
treated with pancrelipase de novo. After medication, numbers
of numerical rating scale (NRS) as an indicator of pain
(ranging from 0–10) decreased, and upper abdominal and/
or back pain were relieved in nine (82%) of the 11 patients
with NAECP who suffered from them (Table 3). Pain relief
was observed within 3 months in almost these 11 patients.

Serum levels of pancreatic enzymes were not altered in the
six patients with normal levels before treatment. In contrast,
of the seven patients with elevated serum levels of pancreatic
enzymes, four showed reductions to normal ranges.
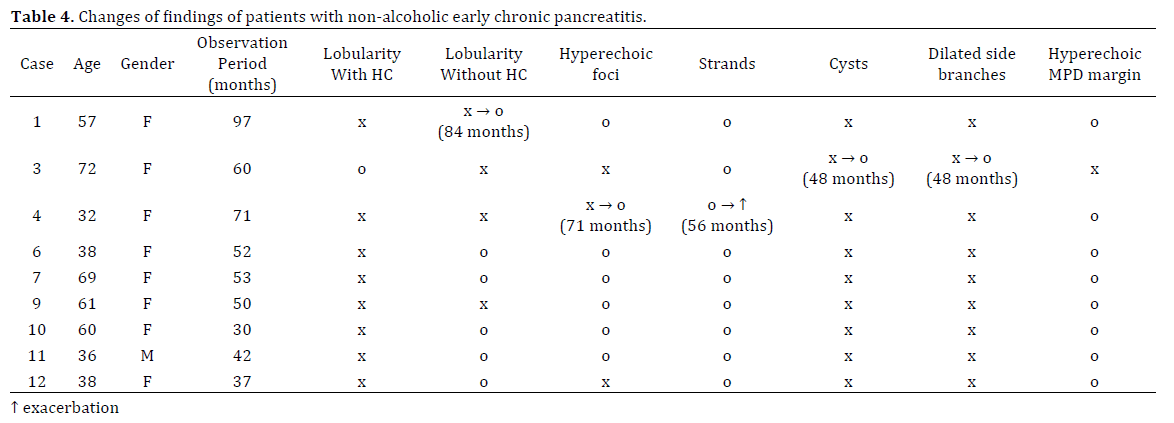
Nine (69%) of the 13 patients were followed-up by EUS
for 2 to 8 years. Over this time period, Patient 1 developed
lobularity without honeycombing, Patient 3 developed cysts and dilated side branches, and Patient 4 developed
hyperechoic foci, as well as strands deterioration. These
EUS findings emerged after more than 4 years. Follow-up
EUS findings after two or more years showed exacerbation
of NAECP in these three patients, equivalent to initial EUS
findings in six patients. Improvements in EUS findings
were not observed. However, all patients in this study
fulfilled the criteria for neither definite nor probable CP
during the clinical courses of their disease (Table 4).
DISCUSSION
Although the clinical diagnosis of advanced stage CP
is easy, diagnosis of early stage CP remains difficult. The
concept of ECP was first established to improve long-term
prognosis in the 2009 Japanese diagnostic criteria for CP
[3]. Because the clinical features of ECP have remained
unclear, this study retrospectively investigated the clinical
features of NAECP.
CT has been reported superior to ERCP in detecting
parenchymal changes associated with advanced stage CP
[9]. However, CT has insufficient diagnostic ability in early
stage CP [5, 18, 19], showing no definitive abnormalities in
the pancreas of all 13 patients diagnosed with NAECP by
EUS in this study.
Most pancreatologists have considered ERCP the gold
standard for morphological diagnosis and staging of CP in
the absence of histopathology. ERCP findings were found
to correlate with histopathology in 23 (74%) of 31 patients
[20]. Pancreatography has been reported to provide poor
diagnostic accuracy in patients with mild CP, although it
was more accurate in those with moderate and severe
CP [10, 11]. Pancreatography alone would be insufficient
for diagnosis of CP. In addition, the incidence rates of
post ERCP complications (e.g. pancreatitis, bleeding, and
infection) have been reported to be 6–7% [21].
EUS has been reported useful for the diagnosis of
CP [11, 12, 13, 14, 15]. Rosemont classification was proposed in 2009 [10], and ECP was newly defined in
the 2009 Japanese diagnostic criteria for CP [3] based on
the classification. These criteria include the use of EUS
as the diagnostic modality to detect ECP. EUS findings in
ECP are consistent with indeterminate CP according to
the Rosemont classification. Excellent agreement was observed between EUS and ERCP in the diagnosis of CP,
except for mild changes on EUS [11, 13]. However, this
study could not compare the sensitivity of ERCP and EUS
in diagnosing ECP, because ERCP was seldom performed.
In this study, EUS findings frequently observed included
strands (100%), hyperechoic MPD margin (85%), hyperechoic foci without shadowing (77%), and lobularity
without honeycombing (54%). Hyperechoic foci have
been reported to correspond to focal fibrosis, strands
to bridging fibrosis, lobularity to interlobular fibrosis,
and hyperechoic MPD margins to periductal fibrosis
[22, 23]. These EUS findings are thought to be crucial for
diagnosis of ECP, with correlations between EUS findings
and histopathology reported in patients with CP [24, 25]. Parenchymal changes are thought to precede ductal
changes in CP [26]. Based on their abilities to diagnose ECP
and complication rates, EUS should be recommended over
ERCP in the diagnosis of ECP.
MRI in patients with CP shows diminished signal
intensity on fat-suppressed T1-weighted images,
suggesting loss of aqueous proteins within the pancreatic
acini. In addition, MRI shows diminished parenchymal
enhancement on capillary phase images, suggesting
disruption of the normal capillary bed and increased
chronic inflammation and fibrosis [6, 7, 27, 28]. However,
none of the eight patients with NAECP diagnosed by the
2009 Japanese clinical diagnostic criteria for CP showed
definitive abnormalities in the pancreas. These findings
indicate that EUS is more sensitive than CT or MRI for the
diagnosis of ECP.
MRCP findings in CP include biliary and pancreatic
ductal dilatation, strictures, irregularities in MPD,
sacculation, and ectasia of side branches [9]. MRCP in
patients with early stage CP often show a normal MPD
with dilated and irregular side branches [6, 9, 27, 29].
In this study, MRCP showed normal MPD and side duct
branches in all 8 patients with NAECP diagnosed by the
2009 Japanese diagnostic criteria. However, MRCP yielded
results suspicious for PBM and PD in one patient each. PD
is known to cause pancreatitis [2, 30, 31]. MRCP shows a
dominant dorsal pancreatic duct (Santorini duct) crossing
the lower bile duct and draining to the minor papilla, with
no communication between ventral and dorsal pancreatic
ducts, indicating PD. Furthermore, PBM has been reported
to be the cause of pancreatitis [32, 33, 34]. MRCP was
found to show an anomalous union between the common
bile duct and the pancreatic duct, as well as the presence of
a long common channel [34, 35, 36]. In the cases suspicious
of having NAECP, MRCP may be recommended to detect
the etiology of ECP.
In evidence-based 2015 clinical practice guidelines
for CP, dietary therapy and pharmacotherapy, primarily
with protease inhibitors in addition to elemental diets
were also recommended for pain management in patients
with CP [16, 17]. CM has been reported to attenuate dibutyltin dichloride-induced pancreatic fibrosis in rats
by inhibiting the activity of monocytes and pancreatic
stellate cells [37]. CM was also found to be effective against
dyspepsia associated with non-alcoholic mild pancreatic
disease [38]. Based on these findings, our patients with
NAECP were initially treated with CM; however, CM alone
had an insufficient effect on pain relief in most patients.
Subsequently, these patients were treated with flopropion
and/or pancreatic enzymes. Flopropion was discontinued
due to insufficient efficacy or adverse effects in 50% of
patients treated with this agent. Although pancreatic
enzyme replacement therapy has been reported effective
for pain relief in patients with CP [39, 40], conventional
pancreatic enzymes were ineffective in 50% of patients
treated with these agents.
Pancrelipase is an enteric-coated, delayed-release
pancreatic enzyme, with 6-to 9-fold greater enzymatic
activity than conventional pancreatic enzymes.
Pancrelipase is used to treat patients with CP and those
who have undergone pancreatic surgery [41, 42]. In this
study, pancrelipase was effective in reducing pain in
almost all patients treated with this agent. These findings
suggest that combinations of pancrelipase and CM may be
recommended for pain reduction in patients with NAECP.
Although medication was effective for pain relief,
EUS findings were unchanged or worsened in all nine
patients with NAECP followed up by EUS for several
years. In all three patients with exacerbated EUS findings,
they emerged after more than 4 years. Abstinence from
alcohol is expected to be effective for both pain relief and
improvement of EUS findings in patients with alcoholic
ECP. Our findings showed that medication alone may not
improve EUS findings in patients with NAECP, although
the small population of NAECP was investigated. Further
investigations are necessary to elucidate the cause of
dissociation of EUS findings from pain relief, and to identify
methods to prevent the progression of NAECP.
Rome III diagnostic criteria for functional
gastrointestinal disorders (FGID), including functional
dyspepsia (FD), were formulated in 2006 [43]. CM has
been reported more effective than famotidine in patients
diagnosed with FD [44]. In addition, CP may not be
completely excluded in patients with FD [45]. ECP may be
misdiagnosed as FGID if EUS is not performed. Indeed, 12
(92%) of the 13 patients with NAECP in this study fulfilled
the diagnostic criteria of FD, if CP diagnosed by EUS is
not considered an organic disease. Early stage CP is not
readily diagnosed by CT and MRI, making EUS essential for
diagnosing ECP. First-line diagnostic evaluation of patients
with upper abdominal pain should include EUS plus upper
endoscopy, primarily to detect CP [46]. Patients with upper
abdominal pain accompanied by back pain, and abnormal
pancreatic enzyme levels in serum or urine should be
evaluated by EUS to detect ECP.
In conclusions, EUS is useful in diagnosing NAECP,
as CT and MRI cannot detect abnormalities. Although medication was effective in relieving pain due to NAECP,
it had no effect on EUS findings. Further investigations are
necessary to clarify whether patients with NAECP progress
to definite or probable CP, and their risk of pancreatic
carcinogenesis, and to determine treatments effective in
preventing the progression of NAECP.
Conflict of Interest
The authors declare that there is no conflict of interests
regarding the publication of this paper.
References
- Etemad B, Whitcomb DC. Chronic pancreatitis: diagnosis, classification, and new genetic developments. Gastroenterology 2001; 120:682-707. [PMID: 11179244]
- Hirota M, Shimosegawa T, Masamune A, Kikuta K, Kume K, Hamada S, Kihara Y, et al. Research Committee of Intractable Pancreatic Diseases. The sixth nationwide epidemiological survey of chronic pancreatitis in Japan. Pancreatology 2012; 12:79-84. [PMID: 22487515]
- Shimosegawa T, Kataoka K, Kamisawa T, Miyakawa H, Ohara H, Ito T, Naruse S, et al. The revised Japanese clinical diagnostic criteria for chronic pancreatitis. J Gastroenterol 2010; 45:584-91. [PMID: 20422433]
- Luetmer PH, Stephens DH, Ward EM. Chronic pancreatitis: reassessment with current CT. Radiology 1989; 171:353-7. [PMID: 2704799]
- De Backer AI, Mortelé KJ, Ros PR, Vanbeckevoort D, Vanschoubroeck I, De Keulenaer B. Chronic pancreatitis: diagnostic role of computed tomography and magnetic resonance imaging. JBR-BTR 2002; 85:304-10. [PMID: 12553661]
- Balcı C. MRI assessment of chronic pancreatitis. DiagnInterv Radiol 2011; 17:249-54. [PMID: 20945291]
- Pamuklar E, Semelka RC. MR imaging of the pancreas. MagnReson Imaging Clin N Am 2005; 13:313-30. [PMID: 15935314]
- Axon ATR, Classen M, Cotton PB, Cremer M, Freeny PC, Lees WR. Pancreatography in chronic pancreatitis: international definitions. Gut 1984; 25:1107-12. [PMID: 6479687]
- Choueiri NE, Balci NC, Alkaade S, Burton FR. Advanced imaging of chronic pancreatitis. Curr Gastroenterol Rep 2010; 12:114-20. [PMID: 20424983]
- Catalano MF, Sahai A, Levy M, Romagnuolo J, Wiersema M, Brugge W, Freeman M, et al. EUS-based criteria for the diagnosis of chronic pancreatitis: the Rosemont classification. Gastrointest Endosc 2009; 69:1251-61. [PMID: 19243769]
- Catalano MF, Lahoti S, Geenen JE, Hogan WJ. Prospective evaluation of endoscopic ultrasonography, endoscopic retrograde pancreatography, and secretin test in the diagnosis of chronic pancreatitis. Gastrointest Endosc 1998; 48:11-7. [PMID: 9684658]
- Zuccaro G Jr, Sivak MV Jr. Endoscopic ultrasonography in the diagnosis of chronic pancreatitis. Endoscopy 1992; 24 Suppl 1:347-9. [PMID: 1633779]
- Sahai AV, Zimmerman M, Aabakken L, Tarnasky PR, Cunningham JT, van Velse A, Hawes RH, et al. Prospective assessment of the ability of endoscopic ultrasound to diagnose, exclude, or establish the severity of chronic pancreatitis found by endoscopic retrograde cholangiopancreatography. Gastrointest Endosc 1998; 48:18-25. [PMID: 9684659]
- Wiersema MJ, Hawes RH, Lehman GA, Kochman ML, Sherman S, Kopecky KK. Prospective evaluation of endoscopic ultrasonography and endoscopic retrograde cholangiopancreatography in patients with chronic abdominal pain of suspected pancreatic origin. Endoscopy 1993; 25:555-64. [PMID: 8119204]
- Irisawa A, Katakura K, Ohira H, Sato A, Bhutani MS, Hernandez LV, Koizumi M. Usefulness of endoscopic ultrasound to diagnose the severity of chronic pancreatitis. J Gastroenterol 2007; 42 Suppl 17:90-4. [PMID: 17238035]
- Ito T, Ishiguro H, Ohara H, Kamisawa T, Sakagami J, Sata N, Takeyama Y, et al. Evidence-based clinical practice guidelines for chronic pancreatitis 2015. J Gastroenterol 2016; 51:85-92. [PMID: 26725837]
- Kataoka K, Sakagami J, Hirota M, Masamune A, Shimosegawa T. Effects of oral ingestion of the elemental diet in patients with painful chronic pancreatitis in the real-life setting in Japan. Pancreas 2014; 43:451-7. [PMID: 24622078]
- Bozkurt T, Braun U, Leferink S, Gilly G, Lux G. Comparison of pancreatic morphology and exocrine functional impairment in patients with chronic pancreatitis. Gut 1994; 35:1132-6. [PMID: 7523260]
- Remer EM, Baker ME. Imaging of chronic pancreatitis. Radiol Clin North Am 2002; 40:1229-42. [PMID: 12479708]
- Vitale GC, Davis BR, Zavaleta C, Vitale M, Fullerton JK. Endoscopic retrograde cholangiopancreatography and histopathology correlation for chronic pancreatitis. Am Surg 2009; 75:649-53. [PMID: 19725285]
- Andriulli A, Loperfido S, Napolitano G, NiroG, Valvano MR, Spirito F, Pilotto A, et al. Incidence rates of post-ERCP complications: a systematic survey of prospective studies. Am J Gastroenterol 2007; 102:1781-8. [PMID: 17509029]
- Wallace MB, Hawes RH. Endoscopic ultrasound in the evaluation and treatment of chronic pancreatitis. Pancreas 2001; 23:26-35. [PMID: 11451144]
- Raimondo M, Wallace MB. Diagnosis of early chronic pancreatitis by endoscopic ultrasound. Are we there yet? JOP 2004; 5:1-7. [PMID: 14730117]
- Varadarajulu S, Eltoum I, Tamhane A, Eloubeidi MA. Histopathologic correlates of noncalcific chronic pancreatitis by EUS: a prospective tissue characterization study. Gastrointest Endosc 2007; 66: 501-9. [PMID:17640639]
- Albashir S, Bronner MP, Parsi MA, Walsh RM, Stevens T. Endoscopic ultrasound, secretin endoscopic pancreatic function test, and histology: correlation in chronic pancreatitis. Am J Gastroenterol 2010; 105:2498-503. [PMID: 20606675]
- Balci NC, Alkaade S, Magas L, Momtahen AJ, Burton FR. Suspected chronic pancreatitis with normal MRCP: findings on MRI in correlation with secretin MRCP. J Magn Reson Imaging 2008; 27:125-31. [PMID: 18058927]
- Manikkavasakar S, AlObaidy M, Busireddy KK, Ramalho M, Nilmini V, Alagiyawanna M, Semelka RC. Magnetic resonance imaging of pancreatitis: an update. World J Gastroenterol 2014; 20:14760-77. [PMID: 25356038]
- Semelka RC, Shoenut JP, Kroeker MA, Micflikier AB. Chronic pancreatitis: MR imaging features before and after administration of gadopentetatedimeglumine. J Magn Reson Imaging 1993; 3:79-82. [PMID: 8428105]
- Sai JK, Suyama M, Kubokawa Y, Watanabe S. Diagnosis of mild chronic pancreatitis (Cambridge classification): comparative study using secretin injection-magnetic resonance cholangiopancreatography and endoscopic retrograde pancreatography. World J Gastroenterol 2008; 14:1218-21. [PMID: 18300347]
- Cotton PB. Congenital anomaly of pancreas divisum as cause of obstructive pain and pancreatitis. Gut 1980; 21:105-14. [PMID: 7380331]
- Bernard JP, Sahel J, Giovannini M, Sarles H. Pancreas divisum is a probable cause of acute pancreatitis: a report of 137 cases. Pancreas 1990; 5:248-54. [PMID: 2343039]
- Kamisawa T, Egawa N, Tsuruta K, Okamoto A, Mtsukawa M. Pancreatitis associated with congenital abnormalities of the pancreaticobiliary system. Hepatogastroenterology 2005; 52:223-9. [PMID: 15783036]
- Kamisawa T, Honda G, Kurata M, Tokura M, Tsuruta K. Pancreatobiliary disorders associated with pancreaticobiliary maljunction. Dig Surg 2010; 27:100-4. [PMID: 20551651]
- Kamisawa T, Ando H, Hamada Y, Fujii H, Koshinaga T, Urushihara N, Itoi T, et al. The Japanese Study Group on Pancreaticobiliary Maljunction. Diagnostic criteria for pancreaticobiliary maljunction 2013. J Hepatobiliary Pancreat Sci 2014; 21:159-61. [PMID: 24307541]
- Kamisawa T, Tu Y, Egawa N, Tsuruta K, Okamoto A, Kamata N. MRCP of congenital pancreaticobiliary malformation. Abdom Imaging 2007; 32:129-33. [PMID: 16680507]
- Wang CL, Ding HY, Dai Y, Xie TT, Li YB, Cheng L, Wang B, et al. Magnetic resonance cholangiopancreatography study of pancreaticobiliary maljunction and pancreaticobiliary diseases. World J Gastroenterol 2014; 20:7005-10. [PMID: 24944495]
- Gibo J, Ito T, Kawabe K, Hisano T, Inoue M, Fujimori N, Oono T, et al. Camostatmesilate attenuates pancreatic fibrosis via inhibition of monocytes and pancreatic stellate cells activity. Lab Invest 2005; 85:75-89. [PMID: 15531908]
- Sai JK, Suyama M, Kubokawa Y, Matsumura Y, Inami K, Watanabe S. Efficacy of camostatmesilate against dyspepsia associated with non-alcoholic mild pancreatic disease. J Gastroenterol 2010; 45:335-41. [PMID: 19876587]
- Isaksson G, Ihse I. Pain reduction by an oral pancreatic enzyme preparation in chronic pancreatitis. Dig Dis Sci 1983; 28:97-102. [PMID: 6825540]
- Slaff J, Jacobson D, Tillman CR, Curington C, Toskes P. Protease-specific suppression of pancreatic exocrine secretion. Gatroenterology 1984; 87:44-52. [PMID: 6202586]
- Whitcomb DC, Lehman GA, Vasileva G, Malecka-Panas E, Gubergrits N, Shen Y, Sander-Struckmeier S, et al. Pancrelipase delayed-release capsules (CREON) for exocrine pancreatic insufficiency due to chronic pancreatitis or pancreatic surgery: A double-blind randomized trial. Am J Gastroenterol 2010; 105:2276-86. [PMID: 20502447]
- Nakajima K, Oshida H, Muneyuki T, Kakei M. Pancrelipase: an evidence-based review of its use for treating pancreatic exocrine insufficiency. Core Evid 2012; 7:77-91. [PMID: 22936895]
- Tack J, Talley NJ, Camilleri M, Holtmann G, Hu P, Malagelada JR, Stanghellini V. Functional gastroduodenal disorders. Gastroenterology 2006; 130:1466-79. [PMID: 16678560]
- Ashizawa N, Hashimoto T, Miyake T, Shizuku T, Imaoka T, Kinoshita Y. Efficacy of camostatmesilate compared with famotidine for treatment of functional dyspepsia: is camostatmesilate effective? J Gastroenterol Hepatol 2006; 21:767-71. [PMID: 16677167]
- Miwa H, Kusano M, Arisawa T, Oshima T, Kato M, Joh T, Suzuki H, et al. Evidence-based clinical practice guidelines for functional dyspepsia. J Gastroenterol 2015; 50:125-39. [PMID: 25586651]
- Chang KJ, Erickson RA, Chak A, Lightdale C, Chen YK, Binmoeller KF, Albers GC, et al.US compared with endoscopy plus transabdominal US in the initial diagnostic evaluation of patients with upper abdominal pain. Gastrointest Endosc 2010; 72:967-74. [PMID: 20650452]



