Keywords
Biopsy, Fine-Needle; Cysts; Endosonography; Pancreas
Introduction
Although the exact prevalence of cystic pancreatic lesions is unknown, it is estimated to be around 1% of the general population based on large scale observational imaging studies [1]. While cystic pancreatic lesions are increasingly diagnosed due to the widespread use of cross-sectional imaging modalities like computed tomography (CT) and magnetic resonance imaging (MRI), it is not known if this reflects a true increase in incidence [1]. Inflammatory pseudocysts constitute about 75% of pancreatic cysts but are not classified as true cystic pancreatic lesions since they are non-epithelial inflammatory fluid collections associated with acute or chronic pancreatitis [2]. About 15% of cystic pancreatic lesions can be classified as cystic neoplasms that require further evaluation and monitoring due to risk of progression to malignancy [1, 3]. Based on surgical pathology, cystic pancreatic lesions are classified by the type of epithelium lining the cyst. These include serous cystadenomas, intraductal papillary mucinous neoplasms (IPMN), mucinous cystadenomas, mucinous cystadenocarcinomas, solid pseudopapillary tumors and few other rare types [4].
Despite being the most common modality to identify cystic pancreatic lesions, cross-sectional imaging plays a variable role in characterizing these lesions. Endoscopic ultrasound (EUS) provides real-time high resolution images of cystic pancreatic lesions with morphological details. The combination of fine-needle aspiration (FNA) cytology with the other recently available diagnostic markers has further increased its diagnostic accuracy. In this review, we describe the role of EUS in the diagnosis of commonly encountered cystic pancreatic lesions and review the management options for practicing clinicians.
Radiological Imaging for the Diagnosis of Cystic Pancreatic Lesions
Studies describing the role of non-invasive imaging like CT and MRI in the diagnosis of Cystic pancreatic lesions have been mostly small and retrospective in nature. Relying on radiologic imaging characteristics alone in cystic pancreatic lesions has been shown to be misleading, with up to 40% of serous and mucinous lesions being misdiagnosed as pseudocysts [2, 5]. Reported overall diagnostic accuracy for these lesions has been highly variable ranging between 20% and 83% [6, 7, 8]. In a large multi-center study of 398 patients with cystic pancreatic lesions who underwent surgical resection, an accurate preoperative diagnosis of tumor type was predicted in only 20% of those with serous cystadenoma, 30% of those with mucinous cystadenoma, and 29% of those with mucinous cystadenocarcinoma, most commonly misdiagnosed as pseudocysts [7]. In a more recent study of 18 patients undergoing surgery for cystic pancreatic lesions, CT scan accuracy of preoperative diagnosis was 82% [9]. Few studies used a head-to-head comparison of imaging modalities such as CT and MRI for the diagnosis of cystic pancreatic lesions. In one small study of 12 patients with serous cystadenomas or mucinous cystadenomas, MRI was equal or slightly superior to CT in diagnosing cystic pancreatic lesions, except in its limited ability to demonstrate calcifications of the tumor wall and septa [10]. For IPMN, magnetic resonance cholangiopancreatography (MRCP) has been reportedly superior to endoscopic retrograde cholangiopancreatography (ERCP) for detecting cysts communicating with the main pancreatic duct, but the two modalities were similar in assessing for cyst septations or nodules [11]. Similar results were reported in a study of 18 patients with IPMN, where MRCP was found to be superior to CT in defining pancreatic ductal anatomy [12].
EUS allows close and high resolution imaging of cystic pancreatic lesion morphology. Diagnostic accuracy of EUS imaging alone for detecting malignant or premalignant lesions is reportedly 82% to 96% [13, 14, 15, 16, 17, 18]. In earlier literature, several EUS features of cystic pancreatic lesions were found to be associated with increased malignancy risk including thick wall, presence of septations, and presence of nodule or mass [13, 14]. More recent studies uncovered the limitations of EUS alone in differentiating benign from malignant cystic pancreatic lesions. In one study, blinded experienced endosonographers reviewed EUS videotapes of 31 consecutive cases of pathologically confirmed cystic pancreatic lesions [16]. The interobserver agreement was moderately good in detecting solid component, but only fair for detecting pancreatic duct abnormalities and septations. The agreement for individual types of lesions was moderately good for serous cystadenomas but only fair for the remainder of the lesions. The agreement for diagnosis of neoplastic vs. non-neoplastic lesions was fair, and the overall accuracy rates ranged from 40% to 93% [16]. A large prospective multi-center ultrasound study found that the accuracy of EUS morphology alone for differentiating mucinous from non-mucinous cystic lesions was only 51% [18]. Based on the above studies findings, EUS morphology alone is generally considered insufficient for further characterization of cystic pancreatic lesions and their malignant potential.
Techniques of EUS-FNA: Tips for Endosonographers
EUS-FNA has been widely practiced in the last decade. Numerous studies have prospectively evaluated the safety of EUS-FNA and its complication rate has been confirmed in recent literature to be around 1% or less [19, 20, 21].
EUS-FNA for cystic pancreatic lesions is performed using the linear array echoendoscope under moderate or deep sedation [22]. The ultrasound transducer on the distal tip of the echoendoscope permits needle advancement into the lesion under real-time guidance. Commercially available FNA needles are available and range in size between 19 and 25 gauge. Doppler use is recommended to examine the projected path of the needle to avoid puncturing intervening blood vessels. Once the gut wall is punctured and the needle enters the cyst, the stylet is withdrawn and suction is applied (Video 1). Complete cyst aspiration using only one pass is recommended whenever possible to reduce the risk of infection in the residual fluid. The needle is then withdrawn back into the sheath and then removed. The material retrieved from aspiration is then expressed on two glass slides: one slide is air-dried for immediate staining and on-site review, while the other slide is alcohol-fixed for later cytologic exam. The presence of on-site cytopathology for rapid interpretation is recommended and has been shown to improve the diagnostic yield [23]. The risk of infection from EUSFNA of pancreatic cysts was reported to be as high as 14% in earlier studies [24]. Therefore, routine administration of i.v. antibiotics became the standard of care, best given prior to or immediately after EUSFNA followed by oral antibiotics for 3-5 days. According to recent literature, the complication rate of EUS-FNA of cystic pancreatic lesions is than 3% [21]. Other sampling techniques such as use of Trucut biopsies have also been proposed to enhance tissue yield. Levy et al. [25] performed Trucut biopsies in 10 patients with suspected cystic pancreatic lesions and found it to be diagnostic in 6 patients, partially diagnostic in one patient, and non-diagnostic in 3 patients. Until further randomized prospective trials become available, EUS-FNA remains the mainstay of sampling cystic pancreatic lesions for cytology and tumor markers.
Video 1. Standard approach to fine needle aspiration in a patient with
a 2 cm pancreas body cyst suggestive of a side branch IPMN.
A recently developed cytobrush device (Echobrush®, Cook Medical Inc., Winston-Salem, NC, USA) has been approved for use with a 19-gauge EUS-FNA needle [26, 27, 28]. Cystic pancreatic lesions suitable for cytobrush use must be at least 2 cm in diameter and located in the neck, body or tail of the pancreas. A main limitation is experienced when using the relatively stiff 19-gauge needle to sample cystic pancreatic lesions within the head of the pancreas or the uncinate process. Once the needle is in the cyst, the stylet is withdrawn and the brush is advanced through the sheath under ultrasound guidance. The brush is moved back and forth several times to ensure adequate tangential contact with the cyst wall and any mural nodules or septations. Patients on anti-coagulation are usually excluded due to higher risk of bleeding as shown in recent studies [26]. Prophylactic antibiotics are administered as described above.
Cyst Fluid Evaluation
Cytology
The use of FNA for cytology and fluid analysis of cystic pancreatic lesions has been extensively evaluated due to the above mentioned shortcomings of EUS alone. EUS-FNA cytology provides excellent specificity for the diagnosis of cystic pancreatic lesions exceeding 90% in most published studies [17, 18, 29]. However, the sensitivity of EUS-FNA remains widely variable with most studies reporting sensitivity under 50% [17, 18, 27, 28]. Brandwein et al. [29] reported an EUS-FNA sensitivity, specificity and accuracy of 50%, 100% and 89%, respectively for the diagnosis of malignancy in patients with different types of cystic pancreatic lesions. In another report of 18 patients with surgical pathology correlation, Sedlack et al. [30] reported a sensitivity, specificity and accuracy of 27%, 100% and 55%, respectively; however, in this study FNA was only performed when there was diagnostic uncertainty. Frossard et al. [17] reported that EUSFNA correctly identified 97% cystic pancreatic lesions when a dedicated on-site pathologist reviewed all cytologic preparations in 67 cysts. In another study of 48 patients, the sensitivity, specificity and frequency of cases correctly identified of EUS-FNA cytology for the diagnosis of mucinous cystic neoplasms were 12.5%, 90.6% and 64.6%, respectively [31]. The largest prospective multicenter study to date included 341 patients undergoing EUS-FNA of cystic pancreatic lesions, out of whom 112 patients underwent surgical resection providing a histologic diagnosis of the cystic lesion [18]. The sensitivity and specificity of cytology for diagnosing a mucinous cyst were 35% and 83%, respectively. The sensitivity of cytology for diagnosing malignancy in malignant mucinous lesions was only 22%. From the above studies we conclude that EUSFNA has low sensitivity for the diagnosis of mucinous cysts in general and malignancy within mucinous lesions in particular, which fueled the search for additional sampling techniques and diagnostic studies to overcome this deficiency.
In a pilot study, brush cytology specimens (Video 2) obtained from 10 patients with cystic pancreatic lesions at the time of EUS were superior to conventional FNA because of the higher yield of epithelial cells [26]. Similar findings were detected in a small case series of 12 patients with cystic pancreatic lesions [27]. A recent prospective blinded study, compared the cytology yield of mucinous epithelium from brushing with FNA in 37 patients with 39 suspected mucinous cystic pancreatic lesions. Cytobrushings were more likely to detect intracellular mucin than the EUS-FNA method (P=0.001), including two cases of high grade dysplasia seen exclusively on cytobrushing [28]. The study highlighted the potential complication rate of 8% including post brushing bleeding and pancreatitis.
Video 2. The recommended technique for brushing a large 4 cm
pancreas tail cyst. After initial puncture, part of the cyst fluid is
aspirated prior to introducing the echobrush, which is then moved
back and forth within the cyst cavity with emphasis on tangential
brushing of the cyst wall. After 30-45 seconds of brushing the brush
is pulled inside the needle and the whole needle and brush are
removed as one unit. The cyst then is re-punctured to complete the
aspiration.
Tumor Markers
Several tumor markers have been studied to improve the diagnostic accuracy of EUS-FNA in cystic
pancreatic lesions. These include carcinoembryonic antigen (CEA), carbonic anhydrase (CA) 19-9, CA 72- 4, and CA 125. CEA is currently considered the most reliable for the diagnosis of mucinous cystic pancreatic lesions. CEA is typically elevated in mucinous lesions, but is lower in pseudocysts and non-mucinous tumors [32]. A CEA level below 5 ng/mL was found to provide 100% sensitivity and 86% specificity for distinguishing mucinous neoplasms from other cystic lesions [33]. CEA level greater than 400 ng/mL offers a sensitivity and specificity levels of 13% and 75%, respectively to distinguish mucinous from nonmucinous cystic lesions according to another study [17]. The same study also reported that a CA 19-9 level greater than 50,000 U/mL had 15% sensitivity and 81% specificity in differentiating mucinous from other cystic lesions.
In clinical practice, the most frequently utilized cyst fluid marker is CEA, based on the results of a large prospective study [18]. This study determined that a cut-off of cyst fluid CEA of 192 ng/mL provided a sensitivity of 73% and specificity of 84% for differentiating mucinous from non-mucinous cystic pancreatic lesions in 112 patients who underwent surgery (Cyst Cooperative Study). Cyst fluid CA 19-9 level of 2,900 ng/mL offered a sensitivity of 68% and specificity of 62% for differentiating mucinous from non-mucinous tumors [18].
Other markers such as amylase and lipase may be important in the evaluation of cystic pancreatic lesions. Amylase is usually elevated in inflammatory cysts like pseudocysts but also in IPMN due to communication with the pancreatic duct. Analysis from 12 studies evaluating amylase levels in various cystic pancreatic lesions adopted a concentration level less than 250 U/L favored a diagnosis of serous cystadenoma, mucinous cystadenoma, or mucinous cystadenocarcinoma (sensitivity 44%, specificity 98%) but unlikely to be pseudocysts [34]. The same analysis concluded that CEA level less than 5 ng/mL strongly suggested a serous cystadenoma or pseudocyst and a CEA greater than 800 ng/mL strongly suggested mucinous cystic neoplasm.
We recommend evaluation of cyst fluid from EUSFNA for CEA, cytology and amylase tests whenever sufficient fluid is obtained. Most labs nowadays require at 0.5-1.0 mL of fluid for CEA testing. If less fluid is obtained, we recommend sending a specimen for cytology first. Other cyst fluid tumor markers such as CA 19-9 although remain available, are of little clinical value and their use is not routinely recommended.
Genetic Markers
Due to the revolution in translational science, molecular markers are aggressively sought as a more reliable alternative diagnostic marker for many malignancies. Specific genetic markers are increasingly identified and utilized to gauge the risk of malignancy in cystic pancreatic lesions. IPMNs are believed to follow a transformation process similar to the adenoma-carcinoma sequence in colon cancer, where lesions progress from hyperplasia to dysplasia and carcinoma [35]. K-ras gene mutation has been well studied and appears to occur early in the transformation sequence [35]. As in other cancers, multiple steps are believed to be required for the progression of precancerous cystic tumors to malignancy. In IPMN, this is reported to be a result of tumor suppressor gene inactivation, which is represented by loss of heterozygosity at p16 and p53 genes [36]. The same markers have been evaluated in non-IPMN lesions by Kim et al. [37] who found that K-ras mutations were present in one-third of mucinous cystic neoplasm, but not in serous cystadenoma.
Clinical applications of the above markers are becoming increasingly available. Pancreatic juice containing K-ras mutations in frequency up to 60% was found in patients with IPMN [38, 39]. Similar to pancreatic juice, cystic pancreatic lesion fluid contains DNA shed from the epithelial lining [40]. In a multicenter, prospective study, Khalid et al. [41] evaluated the role of DNA analysis in 113 patients undergoing EUS-FNA with malignant cytology or later confirmed surgical pathology. This study found that an elevated quantity of good quality DNA and high amplitude mutations were associated with malignant cystic neoplasms. Mutational sequence of K-ras followed by allelic loss was very specific for malignant cysts. The presence of K-ras mutation was also indicative of a mucinous cyst [41]. A recent study though revealed the limitations of relying on molecular analysis only [42]. In 100 patients with suspected mucinous cysts, poor agreement was found between CEA and molecular analysis for the classification of mucinous cysts (kappa=0.2). The combination of CEA and molecular analysis achieved 100% sensitivity for the diagnosis of mucinous cyst [42].
A commercially available genetic test (RedPath® Integrated Pathology, Inc., Pittsburgh, PA, USA) is available to identify the above genetic markers. We recommend obtaining such studies in cysts where cytopathology and CEA are not diagnostic and when there are no clear indications for surgical resection. The high cost of this analysis should also be further evaluated within cost-benefit analysis in comparison to the other lower cost biomarkers.
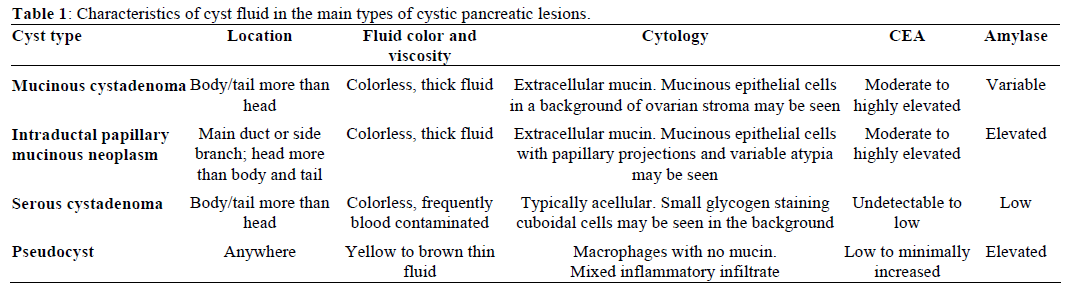
In the next part of the review, we will discuss the common types of cystic pancreatic lesions individually while focusing on the EUS features, cytology and tumor markers’ characteristics (Table 1).
Mucinous Cystic Neoplasms
Mucinous cystic neoplasms are classified as either mucinous cystadenoma or mucinous cystadenocarcinoma. These tumors are usually associated with extracellular mucin production with variable cellular atypia. Females seem to be more frequently affected than males, particularly in their 5th and 6th decade [43, 44]. These lesions occur most commonly in the pancreatic body and tail. Currently, the presence of ovarian stroma is required for the diagnosis of this lesion [45]. Mucinous cystic neoplasms can be completely asymptomatic when incidentally noted on imaging studies, but large lesions may present with obstructive symptoms, pain, or weight loss. Jaundice is rarely a presenting symptom but could indicate underlying malignant transformation. There is typically no communication between the cystic lesion and the pancreatic ductal system, and main duct dilation should raise the suspicion of an alternative diagnosis like IPMN [44].
The EUS appearance of mucinous cystic neoplasm is variable. They are commonly associated with a visible wall and septations of variable thickness, and peripheral calcifications can be seen in some cases (Figures 1 and 2) [43]. Invasive malignancy has been associated with the presence of thick or irregular cyst wall, intramural nodules or solid components and larger cyst size (Figure 3) [14]. EUS-FNA cytology could reveal columnar epithelial cells in up to half of the patients in association with extracellular mucin [34, 46]. Mucin is frequently identified on EUS-FNA of mucinous cystic neoplasm and cyst fluid is typically clear with elevated CEA levels and low amylase. Mucinous cystic neoplasms are premalignant lesions but the risk of malignant degeneration is likely less than that of IPMN [45]. The risk of malignancy in these tumors described in a series of 163 patients was found to be 17.5% [47]. Therefore, surgical resection is recommended for all surgically fit patients. The prognosis after surgery for mucinous cystic neoplasm that have not undergone malignant transformation is excellent and the 5-year survival for mucinous cystadenocarcinomas post resection exceeds 60% [6, 48].
Figure 1. EUS findings in a 42-year-old female patient with a
mucinous cystic neoplasm in the body of the pancreas. A cyst wall is
present in addition to one tangential thin septum. The adjacent
parenchyma appears unremarkable. No FNA was performed in this
case and the patient was referred to surgery.
Figure 2. a. CT scan of the abdomen in a 56-year-old female with left upper quadrant pain demonstrates a unilocular pancreatic tail cyst. The cyst
wall has variable thickness but does not demonstrate any nodularity. No solid mass was noted. Pseudocyst was suggested in the differential diagnosis
of this lesion. b. EUS appearance of the same cyst in A. Thick mucoid cyst content appears granulated on ultrasound, but no visible septations or
solid lesions demonstrated. c. Gross surgical resection specimen for the same patient (distal pancreatectomy with splenectomy). No malignancy was
detected in this specimen. d. Photomicrograph of a mucinous cystadenoma (H&E, 400x). Columnar mucinous epithelial cells are seen overly ovarian
stroma, which is a hallmark of these tumors.
Figure 3. EUS findings in a middle age female patient with a
mucinous cystic neoplasm in the body of the pancreas. A thick wall
and a solid mass are features suggestive of malignancy. Surgical
resection confirmed mucinous cystadenocarcinomas.
Intraductal Papillary Mucinous Neoplasms (IPMNs)
IPMNs are premalignant mucinous cystic lesions affecting men and women equally in their 6th to 7th decade [49]. IPMNs arise from the main pancreatic duct, and or its side branches and are associated with intraductal papillary growth and mucin production, typically leading to main duct or side branch ectasia or both [50]. IPMN is classified histologically as adenoma, borderline, or carcinoma.
The natural history of IPMN is not clear, but an interval of approximately 5 years has been observed between adenoma and transformation to invasive carcinoma [49, 51]. The risk of malignancy being present at the time of diagnosis increases with older age, presence of symptoms, involvement of the main pancreatic duct, dilation of the main pancreatic duct over 10 mm, the presence of mural nodules, and size over 3 cm for side-branch IPMN [51, 52, 53].
Main duct IPMN is typically easy to differentiate on EUS and ERCP due the diffuse dilation of the pancreatic duct, mural tumor growth and occasionally intraductal filling defects due to mucin production (Figure 4). EUS imaging of branched duct IPMN usually demonstrates visible communication of the cyst with the main pancreatic duct. However, in the absence of duct communication, branched duct IPMNs may be morphologically indistinguishable from mucinous cystic neoplasms. Endoscopic visualization of mucin extruding from a patulous papilla (referred to as “fish mouth deformity”) supports the diagnosis. On EUS, any intraductal mass, mural nodule (Figure 5) or projections noted within the main duct or off a cyst wall should be sampled by FNA. If no visible lesions are noted, the main duct or branch can be punctured for cytology and tumor markers. Cytology usually reveals thick mucin but may be thin and completely acellular [54]. Occasionally, fragments of papillary mucinous epithelium can be seen on FNA or cytobrushings. Cyst fluid resembles that obtained from mucinous cystic neoplasm with a relatively elevated CEA; however, amylase tends to be higher due to the ductal communication.
Figure 4. Intraductal papillary mucinous neoplasm affecting the
main pancreatic duct (seen in the body/tail segment) in a male patient
with acute recurrent pancreatitis. EUS showed a dilated pancreatic
duct within the body of the pancreas.
Figure 5. EUS appearance of a cystic lesion in the body of the
pancreas communicating with the main duct via a small side branch.
The lesion has papillary projections and a solid mural nodule.
Despite its outstanding specificity, a major limitation of EUS-FNA in detecting invasive malignancy preoperatively is its low sensitivity, which has been reported to be as low as 44% in some studies [34, 55]. Pais et al. [51] reported an EUS sensitivity as high as 75% in detecting malignancy in patients with IPMN. This same study reported that cyst fluid CEA and CA 19-9 are of limited value in differentiating malignant from benign IPMNs. Wiesenauer et al. [56] showed that the combination of EUS and ERCP cytology samples had a 91% sensitivity for invasive IPMN carcinoma but only 40% for minimally invasive disease like carcinoma in situ or high grade dysplasia. Recently, studies have described the use of intraductal ultrasonography (IDUS) in the evaluation of IPMN. Hara et al. [57] reported IDUS sensitivity, specificity, and accuracy of 68%, 89%, and 78%, respectively for lesions protruding 4 mm or more within the duct. However, IDUS failed to reliably distinguish dysplastic from invasive lesions. This technology is confined to few referral centers and further prospective studies are needed to clarify its role in the initial evaluation and follow up of patients with IPMN.
The risk of malignancy in the main duct type has been reported to range from 57% to 92% [58, 59, 60, 61] and therefore surgery is recommended for these patients. The risk is less established for the side branch type but is probably less than 15% [52]. However, the inability to reliably diagnose IPMN with variable degrees of dysplasia pre-operatively appears to have a higher significance in small lesions (less than 3 cm in size) where the general recommendations have been to observe these lesions. In a recent study of 147 patients with branch duct IPMN, the malignancy rate was 12% in patients who underwent surgical resection [62]. In this same study, cyst size (greater than 3 cm) and presence of pancreas related symptoms had no effect on the risk of malignancy. Two other studies have shown that the risk of malignancy in side-branch lesions is 6% and 46%, respectively [63, 64] and that invasive cancer can be detected in lesions less than 3 cm in size [58, 59, 60]. Based on this finding, all suspected IPMN lesions that do not meet current resection criteria should be followed by imaging studies at least on annual basis.
Serous Cystic Neoplasms
Serous cystadenomas are usually considered to be benign neoplasms originating from centro-acinar cells of the pancreas. They occur mainly in females around seventh decade of life. They are typically asymptomatic, usually found incidentally on imaging studies. The site of the pancreas most frequently affected is controversial; some studies report higher incidence in the body and tail [61], while others report a higher incidence in the head and neck [65]. The classic endosonographic appearance of a microcystic serous cystadenoma is a complex lesion with multiple, small fluid filled cavities (typically less than 5 mm in size) separated by thin septa (Video 3). A central calcified scar gives it its “sunburst” appearance visible in up to a quarter of the patients [48]. The lesion is usually isolated from the pancreatic duct and presence of nodules, solid mass lesion, or cyst wall thickening are unusual features of serous cystadenomas and should raise suspicion about the classification of the lesion [14, 66].
Video 3. Characteristic endoscopic ultrasound appearance of a
microcystic serous cystadenoma in the body of the pancreas in an
asymptomatic 72-year-old female patient. The lesion contains
multiple small cysts separated by thin septa. FNA from this lesion
was hypocellular.
EUS-FNA has a relatively low yield in serous cystadenoma due to the small size of the cystic compartments and the relatively vascular intercystic septa. The distinctive endosonographic appearance of microcystic serous cystadenoma makes cyst sampling generally unnecessary. If attempted, EUS-FNA should target the larger cystic compartments for fluid analysis. Fluid obtained is typically thin, transparent yellow and non-viscous. Although cellularity is usually very low, detection of small cuboidal epithelial cells in clusters with cytoplasm containing glycogen vacuoles facilitates the cytologic diagnosis but is seen only in up to half of the cases [67]. CEA levels are usually low (less than 20 ng/mL) [68]. A less often encountered variant is the macrocystic variant which has an appearance indistinguishable from mucinous cystic pancreatic lesions.
Expectant management is followed in small asymptomatic tumors, however resection of large serous cystadenoma is recommended regardless of the presence or absence of symptoms, because of the malignant potential [69, 70].
Other Rare Types of Cystic Pancreatic Lesions
Other rare tumors of the pancreas that could present as cystic lesions on imaging include solid pseudopapillary tumors of the pancreas. These are rare tumors that occur predominantly in young women and are usually found incidentally on abdominal imaging studies. If large enough, they can present with symptoms due to mass effect [71, 72, 73, 74, 75]. EUS appearance varies and ranges from a totally solid to a mixed solid and cystic mass (Figure 6). FNA usually shows branching papillae with myxoid stroma and is diagnostic in the majority of cases. A recent multicenter study reported that EUS-FNA with or without immunochemistry preoperatively diagnosed 75% of 28 patients [75]. On immunohistochemistry, the tumor cells show significant uptake for vimentin and therefore cellblock Other rare tumors of the pancreas that could present as cystic lesions on imaging include solid pseudopapillary tumors of the pancreas. These are rare tumors that occur predominantly in young women and are usually found incidentally on abdominal imaging studies. If large enough, they can present with symptoms due to mass effect [71, 72, 73, 74, 75]. EUS appearance varies and ranges from a totally solid to a mixed solid and cystic mass (Figure 6). FNA usually shows branching papillae with myxoid stroma and is diagnostic in the majority of cases. A recent multicenter study reported that EUS-FNA with or without immunochemistry preoperatively diagnosed 75% of 28 patients [75]. On immunohistochemistry, the tumor cells show significant uptake for vimentin and therefore cellblock preparation is recommended when suspected on EUS. Although generally indolent and slow growing, the risk of malignant transformation was reported in up to 15% of cases. Due to this and the relatively young age of bearers, surgical resection is recommended in all surgically fit patients. Prognosis remains very good after surgical resection although few cases with metastatic lesions have been reported [76].
Figure 6. EUS appearance of the solid pseudopapillary tumor in a
21-year-old asymptomatic female patient noted on CT scan
performed for another purpose. The tumor is mostly solid with a
single central small cystic space. The splenic artery runs between the
gastric wall and the lesion.
Neuroendocrine tumors of the pancreas may have a cystic component in a minority of cases [77]. Lesions vary in size and morphology and therefore FNA is recommended. Cytology shows a small homogenous but discohesive small cell population with round nuclei and positive stain for chromogranin and synaptophysin. Routine cell block preparation is therefore recommended in these patients. Other rare cystic pancreatic lesions include metastatic lesions with malignant degeneration [78], teratomas, choriocarcinomas, lymphoepithelial cysts [79] and lymphoceles [80].
Treatment of Cystic Pancreatic Lesions
Conservative Approach
Recent natural history studies support the observation of low risk cystic pancreatic lesions with benign morphology, negative FNA and low tumor markers. The largest cohort study to date included 539 patients with various cystic pancreatic lesions, where the risk of progression to malignancy among lesions less than 3 cm in size without a solid component was around 3% [81]. The risk of malignancy and the benefit of pancreatic resection should be carefully weighed, and review of available cross sectional imaging, EUS and cyst fluid analysis to differentiate mucinous (premalignant) and non-mucinous cystic lesions is warranted prior to committing to a particular approach. Clinicians frequently face the question of how to best manage cystic pancreatic lesions. Experts agree on the importance of taking into consideration the patient age, comorbidities, and an estimation of the cancer risk in the lesion. CT scan, MRI and MRCP are generally considered safe and reliable in providing follow-up data on cyst and pancreatic duct size, but are less sensitive in detecting intra-mural nodules, which are better evaluated by EUS-FNA [81, 82]. Long term follow-up studies of conservatively managed IPMNs is warranted [83].
Surgical Approach
Surgical resection of all malignant and some premalignant cystic pancreatic lesions is warranted. Surgical mortality rates associated with pancreatic surgery used to be high but have decreased in recent years: currently is below 5% at most referral centers [84, 85]. Morbidity from surgical resection however remains over 20% in most series. One high-volume surgical center reported a complication rate of 22% and mortality rate of 0.6% following pancreatic cyst surgery in a group of 170 patients [81]. Enucleation has emerged as an alternative less invasive option in certain surgical centers, with reduced operative times and blood loss without increasing post operative morbidity [86, 87]. However, this approach remains limited to a selective population of patients and referral centers.
Future Developments
Cystic pancreatic lesion ablation using ethanol has been described in a few recent series. In a pilot study of 25 patients, Gan et al. [88] reported their initial technical success with ethanol injection into cystic pancreatic lesions without complications. Twenty three patients underwent follow-up with either surgical resection (5 patients) or repeat imaging. Eight out of 23 patients had complete resolution of the cysts on radiology studies. In a more recent multicenter randomized double-blinded study, DeWitt et al. reported on 42 patients with suspected mucinous or nonmucinous cystic pancreatic lesions and pseudocysts who were randomized to lavage with ethanol (25 patients) vs. saline (17 patients) [89]. EUS-guided ethanol lavage resulted in a statistically significant decrease in cyst surface area compared to saline lavage with a similar safety profile. Overall, 33% of patients had complete cyst resolution by follow-up CT scan [89]. Besides alcohol, other cyst lavage agents have been reported recently. Oh et al. [90] used EUS-guided ethanol lavage with paclitaxel in 10 patients with cystic pancreatic lesions. Results are promising but remain limited by the small number of patients and the shorttem follow-up.
The horizon carries several promising techniques that could improve diagnostic accuracy in malignant cysts like the use of optical coherence tomography and confocal endomicroscopy. Additional cyst ablative techniques are under study and development using preexisting technology like radiofrequency ablation, photodynamic therapy, and isolated or combined use of alcohol and chemotherapeutic agents.
Conclusion
Cystic pancreatic lesions are increasingly detected in symptomatic and asymptomatic patients. Diagnosis and management of such lesions employs a multidisciplinary approach involving gastroenterologists, radiologists and surgeons. Characterization of cyst morphology by cross-sectional imaging studies should be supplemented by the routine use of EUS-FNA in the management of cystic pancreatic lesions. Cytology, tumor markers and DNA analysis can further characterize these lesions and increase the diagnostic accuracy of mucinous and malignant cysts. While certain cystic pancreatic lesions with known high riskfeatures should be considered for surgical resection, expectant management appears to be safe in the majority of mucinous cystic pancreatic lesions. In this group of patients, periodic clinical and imaging surveillance is recommended to monitor signs of cyst progression.
Conflict of interest The authors have no potential conflict of interest
References
- Spinelli KS, Fromwiller TE, Daniel RA, Kiely JM, Nakeeb A,
Komorowski RA, et al. Cystic pancreatic neoplasms: observe or
operate. Ann Surg 2004; 239:651-7. [PMID 15082969]
- Warshaw AL, Rutledge PL. Cystic tumors mistaken for
pancreatic pseudocysts. Ann Surg 1987; 205:393-8. [PMID 3566376]
- Brugge WR, Lauwers GY, Sahani D, Fernandez-del Castillo C,
Warshaw AL. Cystic neoplasms of the pancreas. N Engl J Med 2004;
351:1218-26. [PMID 15371579]
- Kloppel G, Luttges J. WHO-classification 2000: exocrine
pancreatic tumors. Verh Dtsch Ges Pathol 2001; 85:219-28. [PMID
11894402]
- Mathieu D, Guigui B, Valette PJ, Dao TH, Bruneton JN, Bruel
JM, et al. Pancreatic cystic neoplasms. Radiol Clin North Am 1989;
27:163-76. [PMID 2642272]
- Le Borgne J, de Calan L, Partensky C. Cystadenomas and
cystadenocarcinomas of the pancreas: a multiinstitutional
retrospective study of 398 cases. French Surgical Association. Ann
Surg 1999; 230:152-61. [PMID 10450728]
- Procacci C, Biasiutti C, Carbognin G, Accordini S, Bicego E,
Guarise A, et al. Characterization of cystic tumors of the pancreas:
CT accuracy. J Comput Assist Tomogr 1999; 23:906-12. [PMID
10589565]
- Bassi C, Salvia R, Molinari E, Biasutti C, Falconi M, Pederzoli
P. Management of 100 consecutive cases of pancreatic serous
cystadenoma: wait for symptoms and see at imaging or vice versa?
World J Surg 2003; 27:319-23. [PMID 12607059]
- Kehagias D, Smyrniotis V, Kalovidouris A, Gouliamos A,
Kostopanagiotou E, Vassiliou J, Vlahos L. Cystic tumors of the
pancreas: preoperative imaging, diagnosis, and treatment. Int Surg
2002; 87:171-4. [PMID 12403093]
- Minami M, Itai Y, Ohtomo K, Yoshida H, Yoshikawa K, Iio M.
Cystic neoplasms of the pancreas: comparison of MR imaging with
CT. Radiology 1989; 171:53-6. [PMID 2928546]
- Koito K, Namieno T, Ichimura T, Yama N, Hareyama M, Morita
K, Nishi M. Mucin-producing pancreatic tumors: comparison of MR
cholangiopancreatography with endoscopic retrograde
cholangiopancreatography. Radiology 1998; 208:231-7. [PMID
9646818]
- Waters JA, Schmidt CM, Pinchot JW, White PB, Cummings
OW, Pitt HA, et al. CT vs MRCP: optimal classification of IPMN
type and extent. J Gastrointest Surg 2008; 12:101-9. [PMID
17917784]
- Koito K, Namieno T, Nagakawa T, Shyonai T, Hirokawa N,
Morita K. Solitary cystic tumor of the pancreas: EUS-pathologic
correlation. Gastrointest Endosc 1997; 45:268-76. [PMID 9087833]
- Gress F, Gottlieb K, Cummings O, Sherman S, Lehman G.
Endoscopic ultrasound characteristics of mucinous cystic neoplasms
of the pancreas. Am J Gastroenterol 2000; 95:961-5. [PMID
10763945]
- Ahmad NA, Kochman ML, Lewis JD, Ginsberg GG. Can EUS
alone differentiate between malignant and benign cystic lesions of
the pancreas? Am J Gastroenterol 2001; 96:3295-300. [PMID
11774939]
- Ahmad NA, Kochman ML, Brensinger C, Brugge WR, Faigel
DO, Gress FG, et al. Interobserver agreement among
endosonographers for the diagnosis of neoplastic versus nonneoplastic
pancreatic cystic lesions. Gastrointest Endosc 2003;
58:59-64. [PMID 12838222]
- Frossard JL, Amouyal P, Amouyal G, Palazzo L, Amaris J,
Soldan M, et al. Performance of endosonography-guided fine needle
aspiration and biopsy in the diagnosis of pancreatic cystic lesions.
Am J Gastroenterol 2003; 98:1516-24. [PMID 12873573]
- Brugge WR, Lewandrowski K, Lee-Lewandrowski E, Centeno
BA, Szydlo T, Regan S, et al. Diagnosis of pancreatic cystic
neoplasms: a report of the cooperative pancreatic cyst study.
Gastroenterology 2004; 126:1330-6. [PMID 15131794]
- Al-Haddad M, Wallace MB, Woodward TA, Gross SA,
Hodgens CM, Toton RD, Raimondo M. The safety of fine-needle
aspiration guided by endoscopic ultrasound: a prospective study.
Endoscopy 2008; 40:204-8. [PMID 18058615]
- Giovannini M, Seitz JF, Monges G, Perrier H, Rabbia I. Fineneedle
aspiration cytology guided by endoscopic ultrasonography:
results in 141 patients. Endoscopy 1995; 27:171-7. [PMID 7601050]
- Lee LS, Saltzman JR, Bounds BC, Poneros JM, Brugge WR,
Thompson CC. EUS-guided fine needle aspiration of pancreatic
cysts: a retrospective analysis of complications and their predictors.
Clin Gastroenterol Hepatol 2005; 3:231-6. [PMID 15765442]
- DeWitt J, McGreevy K, Sherman S, LeBlanc J. Utility of a
repeated EUS at a tertiary-referral center. Gastrointest Endosc 2008;
67:610-9. [PMID 18279866]
- Klapman JB, Logrono R, Dye CE, Waxman I. Clinical impact of
on-site cytopathology interpretation on endoscopic ultrasound-guided
fine needle aspiration. Am J Gastroenterol 2003; 98:1289-94. [PMID
12818271]
- Wiersema MJ, Vilmann P, Giovannini M, Chang KJ, Wiersema
LM. Endosonography-guided fine-needle aspiration biopsy:
diagnostic accuracy and complication assessment. Gastroenterology
1997; 112:1087-95. [PMID 9097990]
- Levy MJ, Smyrk TC, Reddy RP, Clain JE, Harewood GC,
Kendrick ML, et al. Endoscopic ultrasound-guided trucut biopsy of
the cyst wall for diagnosing cystic pancreatic tumors. Clin
Gastroenterol Hepatol 2005; 3:974-9. [PMID 16234042]
- Al-Haddad M, Raimondo M, Woodward T, Krishna M,
Pungpapong S, Noh K, Wallace MB. Safety and efficacy of cytology
brushings versus standard FNA in evaluating cystic lesions of the
pancreas: a pilot study. Gastrointest Endosc 2007; 65:894-8. [PMID
17210151]
- Bruno M, Bosco M, Carucci P, Pacchioni D, Repici A,
Mezzabotta L, et al. Preliminary experience with a new cytology
brush in EUS-guided FNA. Gastrointest Endosc 2009; 70:1220-4.
[PMID 19665706]
- Al-Haddad M, Gill KR, Raimondo M, Woodward T, Krishna M,
Crook JE, et al. Safety and efficacy of cytology brushings versus
standard fine-needle aspiration in evaluating cystic pancreatic
lesions: a controlled study. Endoscopy 2010; 42:127-32. [PMID
19998218]
- Brandwein SL, Farrell JJ, Centeno BA, Brugge WR. Detection
and tumor staging of malignancy in cystic, intraductal, and solid
tumors of the pancreas by EUS. Gastrointest Endosc 2001; 53:722-7.
[PMID 11375578]
- Sedlack R, Affi A, Vazquez-Sequeiros E, Norton ID, Clain JE,
Wiersema MJ. Utility of EUS in the evaluation of cystic pancreatic
lesions. Gastrointest Endosc 2002; 56:543-7. [PMID 12297771]
- Attasaranya S, Pais S, LeBlanc J, McHenry L, Sherman S,
DeWitt JM. Endoscopic ultrasound-guided fine needle aspiration and
cyst fluid analysis for pancreatic cysts. JOP. J Pancreas (Online)
2007; 8:553-63. [PMID 17873459]
- DeWitt J. EUS-FNA of cystic pancreatic tumors. Tech
Gastrointest Endosc 2005; 7:181-7.
- Hammel P, Levy P, Voitot H, Levy M, Vilgrain V, Zins M, et al.
Preoperative cyst fluid analysis is useful for the differential diagnosis
of cystic lesions of the pancreas. Gastroenterology 1995; 108:1230-5.
[PMID 7535275]
- Van der Waaij LA, Van Dullemen HM, Porte RJ. Cyst fluid
analysis in the differential diagnosis of pancreatic cystic lesions: a
pooled analysis. Gastrointest Endosc 2005; 62:383-9. [PMID
16111956]
- Gerdes B, Wild A, Wittenberg J, Barth P, Ramaswamy A,
Kersting M, et al. Tumor-suppressing pathways in cystic pancreatic
tumors. Pancreas 2003; 26:42-8. [PMID 12499916]
- Wada K, Takada T, Yasuda H, Amano H, Yoshida M, Sugimoto
M, Irie H. Does "clonal progression" relate to the development of
intraductal papillary mucinous tumors of the pancreas? J Gastrointest
Surg 2004; 8:289-96. [PMID 15019925]
- Kim SG, Wu TT, Lee JH, Yun YK, Issa JP, Hamilton SR,
Rashid A. Comparison of epigenetic and genetic alterations in
mucinous cystic neoplasm and serous microcystic adenoma of
pancreas. Mod Pathol 2003; 16:1086-94. [PMID 14614047]
- Berthélemy P, Bouisson M, Escourrou J, Vaysse N, Rumeau JL,
Pradayrol L. Identification of K-ras mutations in pancreatic juice in
the early diagnosis of pancreatic cancer. Ann Intern Med 1995;
123:188-91. [PMID 7598300]
- Tada M, Teratani T, Komatsu Y, Kawabe T, Shiratori Y, Omata
M. Quantitative analysis of ras gene mutation in pancreatic juice for
diagnosis of pancreatic adenocarcinoma. Dig Dis Sci 1998; 43:15-20.
[PMID 9508517]
- Tateishi K, Tada M, Yamagata M, Isayama H, Komatsu Y,
Kawabe T, et al. High proportion of mutant K-ras gene in pancreatic
juice of patients with pancreatic cystic lesions. Gut 1999; 45:737-40.
[PMID 10517912]
- Khalid A, Zahid M, Finkelstein SD, LeBlanc JK, Kaushik N,
Ahmad N, et al. Pancreatic cyst fluid DNA analysis in evaluating
pancreatic cysts: a report of the PANDA study. Gastrointest Endosc
2009; 69:1095-102. [PMID 19152896]
- Sawhney M, Devarajan S, O'Farrell R, Cury M , Rabi Kundu R,
Girish Anand G, et al. Comparison of CEA and DNA analysis in 100
consecutive patients with pancreatic cysts. Gastrointest Endosc 2008;
67:AB209.
- Sarr MG, Carpenter HA, Prabhakar LP, Orchard TF, Hughes S,
van Heerden JA, DiMagno EP. Clinical and pathologic correlation of
84 mucinous cystic neoplasms of the pancreas: can one reliably
differentiate benign from malignant (or premalignant) neoplasms?
Ann Surg 2000; 231:205-12. [PMID 10674612]
- Zamboni G, Scarpa A, Bogina G, Iacono C, Bassi C, Talamini
G, et al. Mucinous cystic tumors of the pancreas: clinicopathological
features, prognosis, and relationship to other mucinous cystic tumors.
Am J Surg Pathol 1999; 23:410-22. [PMID 10199470]
- Reddy RP, Smyrk TC, Zapiach M, Levy MJ, Pearson RK, Clain
JE, et al. Pancreatic mucinous cystic neoplasm defined by ovarian
stroma: demographics, clinical features, and prevalence of cancer.
Clin Gastroenterol Hepatol 2004; 2:1026-31. [PMID 15551256]
- Sperti C, Pasquali C, Pedrazzoli S, Guolo P, Liessi G.
Expression of mucin-like carcinoma-associated antigen in the cyst
fluid differentiates mucinous from nonmucinous pancreatic cysts.
Am J Gastroenterol 1997; 92:672-5. [PMID 9128321]
- Crippa S, Salvia R, Warshaw AL, Domínguez I, Bassi C,
Falconi M, et al. Mucinous cystic neoplasm of the pancreas is not an
aggressive entity: lessons from 163 resected patients. Ann Surg 2008;
247:571-9. [PMID 18362619]
- Warshaw AL, Compton CC, Lewandrowski K, Cardenosa G,
Mueller PR. Cystic tumors of the pancreas. New clinical, radiologic,
and pathologic observations in 67 patients. Ann Surg 1990; 212:432-
4. [PMID 2171441]
- Sohn TA, Yeo CJ, Cameron JL, Hruban RH, Fukushima N,
Campbell KA, Lillemoe KD. Intraductal papillary mucinous
neoplasms of the pancreas: an updated experience. Ann Surg 2004;
239:788-97. [PMID 15166958]
- D'Angelica M, Brennan MF, Suriawinata AA, Klimstra D,
Conlon KC. Intraductal papillary mucinous neoplasms of the
pancreas: an analysis of clinicopathologic features and outcome. Ann
Surg 2004; 239:400-8. [PMID 15075659]
- Pais SA, Attasaranya S, Leblanc JK, Sherman S, Schmidt CM,
DeWitt J. Role of endoscopic ultrasound in the diagnosis of
intraductal papillary mucinous neoplasms: correlation with surgical
histopathology. Clin Gastroenterol Hepatol 2007; 5:489-95. [PMID
17350894]
- Sugiyama M, Izumisato Y, Abe N, Masaki T, Mori T, Atomi Y.
Predictive factors for malignancy in intraductal papillary-mucinous tumours of the pancreas. Br J Surg 2003; 90:1244-9. [PMID
14515294]
- Salvia R, Fernández-del Castillo C, Bassi C, Thayer SP, Falconi
M, Mantovani W, et al. Main-duct intraductal papillary mucinous
neoplasms of the pancreas: clinical predictors of malignancy and
long-term survival following resection. Ann Surg 2004; 239:678-85.
[PMID 15082972]
- Stelow EB, Stanley MW, Bardales RH, Mallery S, Lai R, Linzie
BM, Pambuccian SE. Intraductal papillary-mucinous neoplasm of the
pancreas. The findings and limitations of cytologic samples obtained
by endoscopic ultrasound-guided fine-needle aspiration. Am J Clin
Pathol 2003; 120:398-404. [PMID 14502804]
- Maire F, Couvelard A, Hammel P, Ponsot P, Palazzo L, Aubert
A, et al. Intraductal papillary mucinous tumors of the pancreas: the
preoperative value of cytologic and histopathologic diagnosis.
Gastrointest Endosc 2003; 58:701-6. [PMID 14595305]
- Wiesenauer CA, Schmidt CM, Cummings OW, Yiannoutsos CT,
Howard TJ, Wiebke EA, et al. Preoperative predictors of malignancy
in pancreatic intraductal papillary mucinous neoplasms. Arch Surg
2003; 138:610-7. [PMID 12799331]
- Hara T, Yamaguchi T, Ishihara T, Tsuyuguchi T, Kondo F, Kato
K, et al. Diagnosis and patient management of intraductal papillarymucinous
tumor of the pancreas by using peroral pancreatoscopy and
intraductal ultrasonography. Gastroenterology 2002; 122:34-43.
[PMID 11781278]
- Kubo H, Chijiiwa Y, Akahoshi K, Hamada S, Harada N, Sumii
T, et al. Intraductal papillary-mucinous tumors of the pancreas:
differential diagnosis between benign and malignant tumors by
endoscopic ultrasonography. Am J Gastroenterol 2001; 96:1429-34.
[PMID 11374678]
- Serikawa M, Sasaki T, Fujimoto Y, Kuwahara K, Chayama K.
Management of intraductal papillary-mucinous neoplasm of the
pancreas: treatment strategy based on morphologic classification. J
Clin Gastroenterol 2006; 40:856-62. [PMID 17016145]
- Kawamoto S, Lawler LP, Horton KM, Eng J, Hruban RH,
Fishman EK. MDCT of intraductal papillary mucinous neoplasm of
the pancreas: evaluation of features predictive of invasive carcinoma.
AJR Am J Roentgenol 2006; 186:687-95. [PMID 16498096]
- Pyke CM, van Heerden JA, Colby TV, Sarr MG, Weaver AL.
The spectrum of serous cystadenoma of the pancreas. Clinical,
pathologic, and surgical aspects. Ann Surg 1992; 215:132-9. [PMID
1546898]
- Pelaez-Luna M, Chari ST, Smyrk TC, Takahashi N, Clain JE,
Levy MJ, et al. Do consensus indications for resection in branch duct
intraductal papillary mucinous neoplasm predict malignancy? A
study of 147 patients. Am J Gastroenterol 2007; 102:1759-64.
[PMID 17686073]
- Kobari M, Egawa S, Shibuya K, Shimamura H, Sunamura M,
Takeda K, et al. Intraductal papillary mucinous tumors of the
pancreas comprise 2 clinical subtypes: differences in clinical
characteristics and surgical management. Arch Surg 1999; 134:1131-
6. [PMID 10522860]
- Matsumoto T, Aramaki M, Yada K, Hirano S, Himeno Y,
Shibata K, et al. Optimal management of the branch duct type
intraductal papillary mucinous neoplasms of the pancreas. J Clin
Gastroenterol 2003; 36:261-5. [PMID 12590239]
- Sarr MG, Kendrick ML, Nagorney DM, Thompson GB, Farley
DR, Farnell MB. Cystic neoplasms of the pancreas: benign to
malignant epithelial neoplasms. Surg Clin North Am 2001; 81:497-
509. [PMID 11459267]
- Song MH, Lee SK, Kim MH, Lee HJ, Kim KP, Kim HJ, et al.
EUS in the evaluation of pancreatic cystic lesions. Gastrointest
Endosc 2003; 57:891-6. [PMID 12776038]
- Carlson SK, Johnson CD, Brandt KR, Batts KP, Salomao DR.
Pancreatic cystic neoplasms: the role and sensitivity of needle
aspiration and biopsy. Abdom Imaging 1998; 23:387-93. [PMID
9663274]
- Centeno BA, Lewandrowski KB, Warshaw AL, Compton CC,
Southern JF. Cyst fluid cytologic analysis in the differential diagnosis of pancreatic cystic lesions. Am J Clin Pathol 1994;
101:483-7. [PMID 8160642]
- Matsumoto T, Hirano S, Yada K, Shibata K, Sasaki A,
Kamimura T, et al. Malignant serous cystic neoplasm of the
pancreas: report of a case and review of the literature. J Clin
Gastroenterol 2005; 39:253-6. [PMID 15718870]
- Tseng JF, Warshaw AL, Sahani DV, Lauwers GY, Rattner DW,
Fernandez-del Castillo C. Serous cystadenoma of the pancreas:
tumor growth rates and recommendations for treatment. Ann Surg
2005; 242:413-9. [PMID 16135927]
- Chen X, Zhou GW, Zhou HJ, Peng CH, Li HW. Diagnosis and
treatment of solid-pseudopapillary tumors of the pancreas.
Hepatobiliary Pancreat Dis Int 2005; 4:456-9. [PMID 16109536]
- Cheng DF, Peng CH, Zhou GW, Tao ZY, Chen X, Lei RQ, et al.
Clinical misdiagnosis of solid pseudopapillary tumour of pancreas.
Chin Med J (Engl) 2005; 118:922-6. [PMID 15978193]
- Peng CH, Chen DF, Zhou GW, Yang WP, Tao ZY, Lei RQ, et
al. The solid-pseudopapillary tumor of pancreas: the clinical
characteristics and surgical treatment. J Surg Res 2006; 131:276-82.
[PMID 16457845]
- Peng CH, Cheng DF, Zhou GW, Yang WP, Lei RQ, Jin XL, et
al. The surgical treatment of the solid-pseudopapillary tumor of
pancreas: report of 21 cases. Zhonghua Wai Ke Za Zhi 2005; 43:145-
8. [PMID 15842889]
- Jani N, Dewitt J, Eloubeidi M, Varadarajulu S, Appalaneni V,
Hoffman B, et al. Endoscopic ultrasound-guided fine-needle
aspiration for diagnosis of solid pseudopapillary tumors of the
pancreas: a multicenter experience. Endoscopy 2008; 40:200-3.
[PMID 18067066]
- Alexandrescu DT, O'Boyle K, Feliz A, Fueg A, Wiernik PH.
Metastatic solid-pseudopapillary tumour of the pancreas: clinicobiological
correlates and management. Clin Oncol (R Coll Radiol)
2005; 17:358-63. [PMID 16097567]
- Kongkam P, Al-Haddad M, Attasaranya S, O'Neil J, Pais S,
Sherman S, DeWitt J. EUS and clinical characteristics of cystic
pancreatic neuroendocrine tumors. Endoscopy 2008; 40:602-5.
[PMID 18612947]
- DeWitt J, Jowell P, Leblanc J, McHenry L, McGreevy K,
Cramer H, et al. EUS-guided FNA of pancreatic metastases: a
multicenter experience. Gastrointest Endosc 2005; 61:689-6. [PMID
15855973]
- Capitanich P, Iovaldi ML, Medrano M, Malizia P, Herrera J,
Celeste F, et al. Lymphoepithelial cysts of the pancreas: case report
and review of the literature. J Gastrointest Surg 2004; 8:342-5.
[PMID 15019932]
- Lim WC, Leblanc JK, Dewitt J. EUS-guided FNA of a
peripancreatic lymphocele. Gastrointest Endosc 2005; 62:459-62.
[PMID 16111976]
- Allen PJ, D'Angelica M, Gonen M, Jaques DP, Coit DG,
Jarnagin WR, et al. A selective approach to the resection of cystic
lesions of the pancreas: results from 539 consecutive patients. Ann
Surg 2006; 244:572-82. [PMID 16998366]
- Rodriguez JR, Salvia R, Crippa S, Warshaw AL, Bassi C,
Falconi M, et al. Branch-duct intraductal papillary mucinous
neoplasms: observations in 145 patients who underwent resection.
Gastroenterology 2007; 133:72-9. [PMID 17631133]
- Oh HC, Kim MH, Hwang CY, Lee TY, Lee SS, Seo DW, Lee
SK. Cystic lesions of the pancreas: challenging issues in clinical
practice. Am J Gastroenterol 2008; 103:229-39. [PMID 18076739]
- Lillemoe KD, Kaushal S, Cameron JL, Sohn TA, Pitt HA, Yeo
CJ. Distal pancreatectomy: indications and outcomes in 235 patients.
Ann Surg 1999; 229:693-8. [PMID 10235528]
- Yeo CJ, Cameron JL. Improving results of
pancreaticoduodenectomy for pancreatic cancer. World J Surg 1999;
23:907-12. [PMID 10449819]
- Madura JA, Yum MN, Lehman GA, Sherman S, Schmidt CM.
Mucin secreting cystic lesions of the pancreas: treatment by
enucleation. Am Surg 2004; 70:106-12. [PMID 15011911]
- Kiely JM, Nakeeb A, Komorowski RA, Wilson SD, Pitt HA.
Cystic pancreatic neoplasms: enucleate or resect? J Gastrointest Surg
2003; 7:890-7. [PMID 14592663]
- Gan SI, Thompson CC, Lauwers GY, Bounds BC, Brugge WR.
Ethanol lavage of pancreatic cystic lesions: initial pilot study.
Gastrointest Endosc 2005; 61:746-52. [PMID 15855986]
- DeWitt J, McGreevy K, Schmidt CM, Brugge WR. EUS-guided
ethanol versus saline solution lavage for pancreatic cysts: a
randomized, double-blind study. Gastrointest Endosc 2009; 70:710-23. [PMID 19577745]
- Oh HC, Seo DW, Lee TY, Kim JY, Lee SS, Lee SK, Kim MH.
New treatment for cystic tumors of the pancreas: EUS-guided
ethanol lavage with paclitaxel injection. Gastrointest Endosc 2008;
67:636-42. [PMID 18262182]










