Keywords
Endoscopic Ultrasound-Guided Fine Needle Aspiration; Pancreatic Neoplasms
Abbreviations
CP chronic pancreatitis; CT computed tomography;
EUS endoscopic ultrasound; EUS- 1 first EUS-FNA; EUS-2 second
EUS-FNA; EUS-3 third EUS-FNA; FNA fine needle aspiration; IRB
institutional review board; JHH johns hopkins hospital; MRI magnetic
resonance imaging; PD pancreatic duct
INTRODUCTION
Pancreatic cancer is the fourth leading cause of cancer death in the United States and it is projected that there will be 47,000 new cases in 2015 [1]. Pancreatic cancer has the lowest survival rate of all cancers with 74% of patients dying within the first year of diagnosis [1]. Surgical resection is the only potentially curative treatment for pancreatic cancer though this procedure carries a significant morbidity and mortality even if performed by experienced surgeons [2]. Early and accurate diagnosis impacts not only patients’ outcome and patients’ possible surgical candidacy, but also potential targeted chemotherapies.
Endoscopic ultrasound (EUS) with fine needle aspiration (FNA) is considered the current gold standard for preoperative pancreatic cancer staging and tissue acquisition [3]. However, the sensitivity of EUS-FNA for pancreatic tumors is suboptimal and ranges between 62% and 96% [4, 5]. The value of repeat EUS-FNA in patients with non-diagnostic EUS-FNA has not been well established. The aim of this study was to determine the yield of a single or if necessary multiple EUS-FNA procedures for the cytological diagnosis of a pancreatic mass at an academic tertiary-care center.
MATERIALS AND METHODS
The study was approved by the institutional review board (IRB) at Johns Hopkins Hospital (JHH) and complied with Health Insurance Portability and Accountability Act (HIPAA) regulations. All patients provided written informed consent to undergo EUS-FNA. We conducted a retrospective analysis of consecutive patients who underwent EUS-FNA of a pancreatic mass identified on CT or MRI presenting to JHH between January 2006 and October 2010. Patients were identified using a prospectively updated electronic endoscopy database that was updated during the follow-up period which continued until October 2012. All patients were referred for EUS-FNA on the basis of a clinical suspicion of pancreatic cancer. Patients with cystic tumors of the pancreas were excluded because of the different diagnostic algorithm for these patients.
A linear array echoendoscope (GF-UC140P-AL5 or GFUC30P [Olympus America Inc, Center Valley, PA], or FG32- UA or FG36-UX [Pentax Medical Corp, Montvale, NJ]) was used in all patients. EUS-FNA was performed with either a 22-gauge or 25-gauge EchoTip Ultra [Cook Endoscopy Inc, Winston-Salem, NC]) or Expect [Boston Scientific, Natick, Mass] needle. The choice of the needle was at the discretion of the endoscopist. A cytopathologist was available on-site for preliminary interpretations of all FNA procedures. Passes were repeated until the cytopathologist confirmed adequate cellular yield or the endoscopist felt that further sampling would not safely increase the possibility of obtaining a diagnosis.
All procedures were performed by or under the supervision of experienced faculty endoscopists who had each performed greater than 500 EUS procedures. For the purposes of this study, the accuracy of EUS-FNA was categorized based on the final cytopathology report. The cytological diagnosis for each procedure was classified as either “diagnostic” or “non-diagnostic”. Diagnostic procedures obtained cells that were malignant, highly suspicious for malignancy, benign or consistent with chronic pancreatitis. Non-diagnostic procedures obtained cells that were either atypical or inadequate.
If EUS-FNA yielded a non-diagnostic result and the clinical suspicion for pancreatic cancer remained high, then our institutional protocol was to perform repeat EUS-FNA until a diagnostic result was obtained up to a maximum of 3 procedures. The first procedure was termed EUS-1, the second EUS-2 and the third EUS-3.
In this study the final diagnosis was established by careful review of electronic medical records. A final diagnosis of a pancreatic malignancy was based upon (a) cytologic or histologic evidence of malignancy from material obtained by EUS-FNA or alternative means (ERCP, surgical or percutaneous biopsy) or (b) clinical progression judged by evolving local invasion or metastatic disease on follow up CT or MRI or (c) death attributed to a malignant pancreatic lesion based upon clinical records if the cytology or surgical pathology results were inconclusive. A lesion was defined as being benign based upon EUS-FNA results, clinical follow-up, and lack of disease progression over a period of at least 6 months. Patients without adequate follow-up were excluded.
Demographic and clinical data such as age, gender, maximum diameter of pancreatic mass, EUS features of chronic pancreatitis (with ≥ 5/9 features being diagnostic of chronic pancreatitis), number of FNA passes, needle size, final cytolopathology report, final diagnosis and number of EUS-FNA procedures per patient were all recorded.
Statistical Analysis
Continuous variables were reported as means and standard deviation, while categorical variables were reported as proportions. Statistical analysis was performed by using SPSS software (version 16, Inc, Chicago, IL). The sensitivity, specificity, positive predictive value, negative predictive value and diagnostic accuracy of EUS-1, EUS- 2 and EUS-3 were calculated. Univariate analysis was performed using chi-square test for categorical variables and student’s t test for continuous variables. Multivariate analysis was performed using logistic regression to evaluate the predictive value of the variables which were significant in univariate analysis (p<0.05).
RESULTS
Study Population
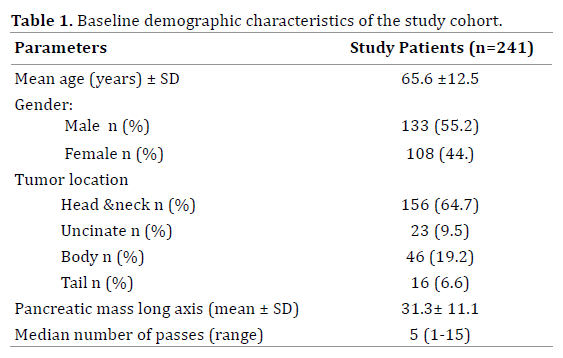
Between January 2006 and October 2010, we identified 249 patients with a pancreatic mass who underwent EUS-FNA. After review, 8 cases were excluded because of insufficient information in their electronic medical record to determine the final diagnosis. Therefore, 241 patients (133 male, mean age 65.6 ±12.5 years) comprised the study population. Of these, 82.2% (198/241) had only one procedure (EUS-1), 16.1% (39/241) had two procedures (EUS-2) and 1.7% (4/241) had three procedures (EUS-3). Hence a total of 288 EUS-FNA procedures were performed in our study population.
Patient demographics and pancreatic mass characteristics are shown in Table 1. With regards to the location of the pancreatic mass, 64.7% were located in the head/neck, 9.5% in the uncinate, 19.2% were in the body, 6.6% were in the tail. The mean maximum diameter of the mass was 31.3 ± 11.1 mm. The median number of passes during the EUS-FNA was 5 (1-15).
The operating characteristics of EUS-FNA are summarized in Table 2. The sensitivity of EUS-1 was 74.1%. Repeating the EUS-FNA up to three times if necessary increased the sensitivity to 86.9%. There was no false positive EUS-FNA diagnosis of pancreatic adenocarcinoma. There were, however, 6 patients who underwent surgical resection despite a negative EUS-FNA and were found to have benign pathologies (5 chronic pancreatitis and 1 autoimmune pancreatitis) on final diagnosis. Therefore, the rate of surgical resection for benign pancreatic masses in the entire cohort was 2.5%.
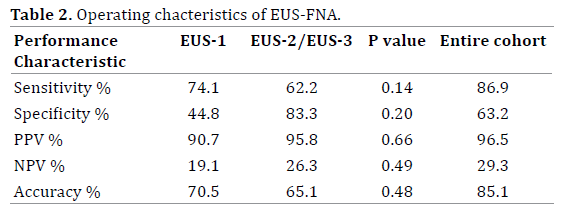
There were 43 patients who underwent 47 repeat EUSFNA (EUS-2 = 39, EUS-3 = 4) due to a non-diagnostic EUS-1. As the number of subjects for EUS-3 is too small to be analyzed alone, the operating characteristics EUS-2 and EUS-3 (EUS- 2/EUS-3) were combined for the purposes of comparison. The operating characteristics of EUS-2/EUS-3 were not significantly different to those of EUS-1 (Table 2). Of the 47 repeat procedures performed, there was no statistically significant difference between the median number of FNA passes performed at EUS-1 (5, range 1-15) compared with EUS-2/EUS-3 combined (6, range 2-12) (p = 0.33).
Final Diagnosis of Pancreatic Mass Lesions
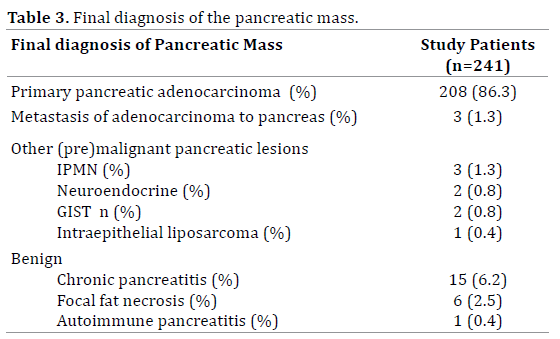
The final diagnoses of the pancreatic masses are shown in Table 3. Pancreatic adenocarcinoma as the final diagnosis was confirmed in 87.6%. Of these, 86.3% were primary pancreatic adenocarcinomas and the remaining 1.3% were metastatic adenocarcinomas to the pancreas. The three metastatic adenocarcinomas originated from renal cell (n=1), primary peritoneal (n=1) and unknown (n=1). There were 8 patients with premalignant pancreatic mass lesions that were not adenocarcinoma [IPMN (n=3), GIST (n=2), neuroendocrine tumor (n=2) and intraperitoneal liposarcoma (n=1)]. Chronic pancreatitis (n=15) was the most common benign lesion followed by focal fat necrosis (n=6) and autoimmune pancreatitis (n=1).
Variable affecting EUS-FNA
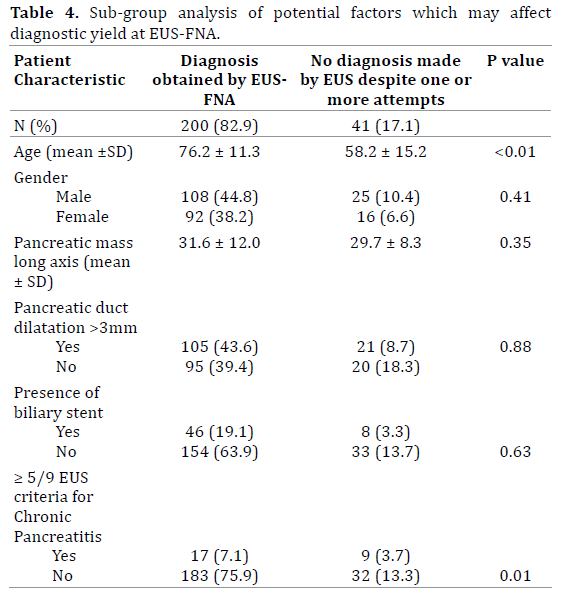
The factors that were thought to influence the ability to obtain a diagnostic specimen are reviewed in Table 4. Univariate analysis revealed absence of ≥5/9 EUS features of chronic pancreatitis was more likely to result in a diagnostic specimen at EUS-FNA (85.1% vs. 65.4% p = 0.011). On the multivariate analysis, age was set as group >65 years old and ≤ 65 years old. Age >65 (OR 2.8, 1.3-6.0 95% CI, p = 0.008) was confirmed to be an independent predictor of diagnostic EUS-FNA. The size of the mass, pancreatic duct dilatation to > 3 mm or the presence of a pre-existing biliary stent did not significantly influence the ability to gain a diagnostic specimen.
DISCUSSION
Despite EUS-FNA being the current gold standard for the diagnosis of a pancreatic mass, 6 to 30% of patients with clinical and imaging findings suggestive of pancreatic malignancy have negative cytology on EUS-FNA [6, 7]. There is no unanimously agreed approach on how to best manage these patients. Possibilities include CTguided biopsy, surgical resection and repeat EUS-FNA. CT-guided biopsy may result in tumor seeding into the peritoneum via spread of malignant cells through the needle tract [8]. Surgical resection is associated with considerable morbidity and hence should be exclusively reserved for malignant resection only [2]. The reported risks of repeat EUS-FNA in this population appears low [9-11]. Additionally, as the risk of a false positive EUS-FNA is negligible [12-14], a repeat EUS-FNA may be the most attractive option.
We report on 241 consecutive patients with a suspicious pancreatic mass who underwent up to three EUS-FNA at our institution over a 5-year period. The majority of patients had their mass in the pancreatic head or neck. Pancreatic adenocarcinoma was confirmed in 87.7% of patients which is exceptionally high in comparison to other studies reporting EUS-FNA for pancreatic mass [15]. In patients who had a final diagnosis of pancreatic cancer, the sensitivity of EUS-1 was 74.1% and repeating the EUSFNA if necessary increased the sensitivity to 86.9%.
In our cohort, 10.4% of patients had a pancreatic mass for which surgical therapy would not be deemed necessary(metastatic adenocarcinoma to the pancreas and benign lesions). This again signifies the importance of pursuing a diagnosis prior to contemplating surgical resection. The sensitivity of EUS-1 was 74.1% despite an on-site cytopathologist being present. This result is lower than the 85% that was reported in a recent meta-analysis [16]. JHH is a tertiary referral center, the cases included are often challenging with masses in locations that are difficult to clearly delineate or access. Our institutions approach was to refer patients with a resectable mass suspicious for pancreatic cancer despite multiple negative EUS-FNA for surgical resection. This resulted in 2.5% patients with a non-diagnostic EUS-FNA undergoing surgical resection having a benign final diagnosis. This number is less than de la Fuente et al. who reported 7.4% of 494 patients having benign disease on postoperative pathology [17].
This study focused exclusively on repeat EUS-FNA for pancreatic mass lesions within a single tertiary referral center. The question of whether the same proceduralist or different one should perform the repeat EUS-FNA is unknown. This question was not answered by the present study as there was no policy in place regarding who should perform the repeat EUS-FNA. It is possible that if the same proceduralist repeated the procedure they may make the same “mistake” again. Alternatively, more diligence may have been observed. Of note, our study did not reveal an increased number of passes in the repeat EUS-FNA as compared to the initial (6 vs. 5, p = 0.33). Another method to increase cytological yield may be to use elastography to aid in precisely targeting the FNA [18].However, there is no published data to describe its value in patients with a previous negative EUS-FNA.
Extrapolating the results of studies in which repeat EUS-FNA was performed in another institution; repeat EUS-FNA appears to have a variable ability to confirm the diagnosis of pancreatic malignancy. Dewitt et al. reported repeating the EUS-FNA had a clinical impact in 65% of 17 patients with a pancreatic mass [9]. Suzuki et al. reported that EUS clarified the diagnosis in 82% of 84 of patients, though in this study, patients with cytology “suspicious for malignancy” were included [11]. Tadic et al. in a study of 46 patients demonstrated a sensitivity of 68% at the initial EUS-FNA which rose to 92% when a repeat procedure was performed [19]. Although a benefit is seen in repeating the EUS-FNA in each of the aforementioned studies, the variation in the method of reporting the results makes comparison between these studies difficult.
Our study showed that older age at EUS-FNA was more likely to result in diagnostic specimen. These results are in keeping with current knowledge. The National Cancer Institute’s Surveillance, Epidemiology, and End Results (SEER) revealed the rate of pancreatic cancer for all ages is 11.7 per 100,000 though for individuals older than 65 years increases it increases to 66.4 per 100,000 [20]. In addition to age, the presence of EUS features of chronic pancreatitis was found to decrease the sensitivity of EUSFNA, consistent with other series that have reported that diagnosing pancreatic cancer on a background of chronic pancreatitis is challenging [21-23]. Other reported reasons for a non-diagnostic sample are the presence of extensive necrotic or cystic areas and intervening vasculature.
Limitations of our study include its retrospective nature and lack of control group. Additionally, we did not record the time interval between the initial and repeat EUS-FNA procedures. Therefore, the intervening time may have resulted in a larger pancreatic mass which may overestimate the benefit of repeat EUS-FNA. Also, we did not record the exact size of needle used (22-gauge vs. 25-gauge) and hence are not clear if a change in needle size contributed to an increased diagnostic yield at the repeat EUS-FNA. However, the literature to date supports no difference in diagnostic yield between these two sized needles so it is unlikely that this affected our results [24-27].
In conclusion, this single center series of 241 patients found that EUS-FNA is an effective method for providing cytological diagnosis in patients with solid pancreatic mass lesions. Repeat procedures appear to be a reasonable course of action in patients with an initial non-diagnostic result. Future studies are required to clarify if the same or a different proceduralist should perform the repeat EUSFNA and define the role of elastography in these patients.
Conflicts of Interest
Vikesh Singh Consultant for Abbvie, Santarus, D-Pharm, Novo Nordisk, Boston Scientific and Enteromedics.
Mouen A Khashab is a consultant for Boston Scientific, Xlumena and Olympus America and has received research support from Cook Medical.
Anthony Kalloo is a founding Member, equity Holder and consultant for Apollo Endosurgery.
All other authors have no relevant disclosures.
References
- Rahib L, Smith BD, Aizenberg R, Rosenzweig AB, Fleshman JM, Matrisian LM. Projecting cancer incidence and deaths to 2030: the unexpected burden of thyroid, liver, and pancreas cancers in the United States. Cancer Res 2014;74:2913-21. [PMID: 24840647]
- Corcione F, Pirozzi F, Cuccurullo D, Piccolboni D, Caracino V, Galante F, Cusano D, Sciuto A. Laparoscopic pancreaticoduodenectomy: experience of 22 cases. SurgEndosc 2013;27:2131-6. [PMID: 23355144]
- Eloubeidi MA, Varadarajulu S, Desai S, Wilcox CM.Value of repeat endoscopic ultrasound-guided fine needle aspiration for suspected pancreatic cancer. J GastroenterolHepatol 2008;23:567-70. [PMID: 18397485]
- Uehara H, Ikezawa K, Kawada N, Fukutake N, Katayama K, Takakura R, Takano Y, Ishikawa O, et al. Diagnostic accuracy of endoscopic ultrasound-guided fine needle aspiration for suspected pancreatic malignancy in relation to the size of lesions. J GastroenterolHepatol 2011;26:1256-61. [PMID: 21501226]
- Tada M, Komatsu Y, Kawabe T, Sasahira N, Isayama H, Toda N, Shiratori Y, Omata M.Quantitative analysis of K-ras gene mutation in pancreatic tissue obtained by endoscopic ultrasonography-guided fine needle aspiration: clinical utility for diagnosis of pancreatic tumor. Am J Gastroenterol 2002;97:2263-70. [PMID: 12358243]
- Eloubeidi MA, Varadarajulu S, Desai S, Shirley R, Heslin MJ, Mehra M, Arnoletti JP, et al. A prospective evaluation of an algorithm incorporating routine preoperative endoscopic ultrasound-guided fine needle aspiration in suspected pancreatic cancer. J GastrointestSurg 2007;11:813-9. [PMID: 17440790]
- Turner BG, Cizginer S, Agarwal D, Yang J, Pitman MB, Brugge WR. Diagnosis of pancreatic neoplasia with EUS and FNA: a report of accuracy. GastrointestEndosc 2010;71:91-8. [PMID: 19846087]
- Micames C, Jowell PS, White R, Paulson E, Nelson R, Morse M, Hurwitz H, et al. Lower frequency of peritoneal carcinomatosis in patients with pancreatic cancer diagnosed by EUS-guided FNA vs. percutaneous FNA. GastrointestEndosc 2003;58:690-5. [PMID: 14595302]
- DeWitt J, McGreevy K, Sherman S, LeBlanc J. Utility of a repeated EUS at a tertiary-referral center. GastrointestEndosc 2008;67:610-9. [PMID: 18279866]
- Nicaud M, Hou W, Collins D, Wagh MS, Chauhan S, Draganov PV. The utility of repeat endoscopic ultrasound-guided fine needle aspiration for suspected pancreatic cancer. Gastroenterol Res Pract 2010;2010:268290. [PMID: 21234311]
- Suzuki R, Lee JH, Krishna SG, Ramireddy S, Qiao W, Weston B, Ross WA, Bhutani MS. Repeat endoscopic ultrasound-guided fine needle aspiration for solid pancreatic lesions at a tertiary referral center will alter the initial inconclusive result. J Gastrointestin Liver Dis 2013;22:183-7. [PMID: 23799217]
- Gleeson FC, Kipp BR, Caudill JL, Clain JE, Clayton AC, Halling KC, Henry MR, Rajan E, et al. False positive endoscopic ultrasound fine needle aspiration cytology: incidence and risk factors. Gut 2010;59:586-93. [PMID: 20427392]
- Schwartz DA, Unni KK, Levy MJ, Clain JE, Wiersema MJ.The rate of false-positive results with EUS-guided fine-needle aspiration.GastrointestEndosc 2002;56:868-72. [PMID: 12447300]
- Siddiqui AA, Kowalski TE, Shahid H, O'Donnell S, Tolin J, Loren DE, Infantolino A, Hong SK, et al. False-positive EUS-guided FNA cytology for solid pancreatic lesions.GastrointestEndosc 2011;74:535-40. [PMID: 21737075]
- Ainsworth AP, Hansen T, Fristrup CW, Mortensen MB. Indications for and clinical impact of repeat endoscopic ultrasound.Scand J Gastroenterol 2010;45:477-82. [PMID: 19968612]
- Hewitt MJ, McPhail MJ, Possamai L, Dhar A, Vlavianos P, Monahan KJ. EUS-guided FNA for diagnosis of solid pancreatic neoplasms: a meta-analysis. GastrointestEndosc 2012;75:319-31. [PMID: 22248600]
- de la Fuente SG, Ceppa EP, Reddy SK, Clary BM, Tyler DS, Pappas TN. Incidence of benign disease in patients that underwent resection for presumed pancreatic cancer diagnosed by endoscopic ultrasonography (EUS) and fine-needle aspiration (FNA). J GastrointestSurg 2010;14:1139-42. [PMID: 20424928]
- Iglesias-Garcia J, Dominguez-Munoz JE. Endoscopicultrasound image enhancementelastography. GastrointestEndosc Clin N Am 2012;22:333-48, x-xi. [PMID: 22632955]
- Tadic M, Kujundzic M, Stoos-Veic T, Kaic G, Vukelic-Markovic M.Role of repeated endoscopic ultrasound-guided fine needle aspiration in small solid pancreatic masses with previous indeterminate and negative cytological findings. Dig Dis 2008;26:377-82. [PMID: 19188731]
- 20.Altekruse SF, Kosary CL, Krapcho M, et al. SEER Cancer Statistics Review, 1975–2007. Bethesda, MD: National Cancer Institute. 2010. Available at: https://seer.cancer.gov/csr/1975_2007/
- Varadarajulu S, Tamhane A, Eloubeidi MA. Yield of EUS-guided FNA of pancreatic masses in the presence or the absence of chronic pancreatitis. GastrointestEndosc 2005;62:728-36; quiz 751, 753. [PMID: 16246688]
- Krishna NB, Mehra M, Reddy AV, Agarwal B.EUS/EUS-FNA for suspected pancreatic cancer: influence of chronic pancreatitis and clinical presentation with or without obstructive jaundice on performance characteristics. GastrointestEndosc 2009;70:70-9. [PMID: 19249774]
- Fritscher-Ravens A, Brand L, Knofel WT, Bobrowski C, Topalidis T, Thonke F, de Werth A, Soehendra N. Comparison of endoscopic ultrasound-guided fine needle aspiration for focal pancreatic lesions in patients with normal parenchyma and chronic pancreatitis. Am J Gastroenterol 2002;97:2768-75. [PMID: 12425546]
- Siddiqui UD, Rossi F, Rosenthal LS, Padda MS, Murali-Dharan V, Aslanian HR. EUS-guided FNA of solid pancreatic masses: a prospective, randomized trial comparing 22-gauge and 25-gauge needles. GastrointestEndosc 2009;70:1093-7. [PMID: 19640524]
- Lee JK, Lee KT, Choi ER, Jang TH, Jang KT, Lee JK, Lee KH. A prospective, randomized trial comparing 25-gauge and 22-gauge needles for endoscopic ultrasound-guided fine needle aspiration of pancreatic masses.Scand J Gastroenterol 2013;48:752-7. [PMID: 23600919]
- Yusuf TE, Ho S, Pavey DA, Michael H, Gress FG. Retrospective analysis of the utility of endoscopic ultrasound-guided fine-needle aspiration (EUS-FNA) in pancreatic masses, using a 22-gauge or 25-gauge needle system: a multicenter experience. Endoscopy 2009;41:445-8. [PMID: 19418399]
- Lee JH, Stewart J, Ross WA, Anandasabapathy S, Xiao L, Staerkel G. Blinded prospective comparison of the performance of 22-gauge and 25-gauge needles in endoscopic ultrasound-guided fine needle aspiration of the pancreas and peri-pancreatic lesions. Dig Dis Sci 2009;54:2274-81. [PMID: 19669880]

