Key words
Biopsy; Biopsy, Fine-Needle; Cytological Techniques; Endosonography; Pancreatic Diseases; Pancreatic Neoplasms
Abbreviations
TCB: trucut biopsy
Introduction
Endoscopic ultrasound-guided fine-needle aspiration biopsy (EUS FNA) of pancreatic masses has a sensitivity ranging from 85% to 90% and a specificity of almost 100% for malignancy [1, 2]. The diagnostic accuracy relies on several factors including the presence of experienced on-site cytopathologist, endosonographer experience and tumor characteristics [3]. In welldifferentiated pancreatic adenocarcinomas, necrotic tumors or when chronic pancreatitis is present, EUS FNA with cytology becomes challenging to cytopathologists and endosonographers. In order to overcome limitations associated with EUS FNA cytology, a 19-gauge trucut biopsy (TCB) needle (Quick Core, Wilson-Cook, Winston- Salem, NC, USA) was introduced to allow core biopsy of lesions [4]. Studies that evaluated the use of EUS TCB for determining the etiology of pancreatic lesions suggested a lower yield when compared to FNA [5, 6, 7].
The aim of this retrospective, case-control study at a single tertiary referral center was to determine the diagnostic yield, safety and overall accuracy of EUS FNA alone or combined with EUS TCB for the diagnosis of suspected malignant pancreatic masses.
PATIENTS AND METHODS
This is a retrospective study of all patients referred to our university-based center for EUS-guided biopsy. Data from our EUS database was reviewed on consecutive patients who underwent EUS guided biopsy from March 2004 to April 2007.
Patients with unresectable tumors or patients with questionable imaging tests for pancreatic malignancy were referred for tissue acquisition. Patient demographics, reports of prior EUS/CT-guided or surgical biopsy, cytopathology and histology reports, imaging reports and clinical data were collected at the time of EUS. Patient follow-up, outcome and results of surgical pathology and/or cytology were obtained from medical records and EUS database when information was available. EUS findings, the number of needle passes performed and procedure-related complications were documented in our EUS database. Size and location of the pancreatic lesions was determined using available radiographic and EUS reports. All the procedures were performed by a single endosonographer (A.R.) in the Endoscopy Unit of University of Miami Hospital and Clinics. EUS TCB was performed when it technically possible when there were transgastrically accessible lesions with no adjacent vascular structure or normal pancreatic parenchyma precluding advancement of the trucut needle and when EUS FNA was nondiagnostic as detailed ahead in methods. All patients had a prior imaging study demonstrating a pancreatic mass or clinical and radiological data suggested the presence of a pancreatic tumor. Radiological reports, laboratory data, serum tumor markers and images were reviewed before EUS-guided biopsy by the endosonographer. Imaging studies were reviewed to assess: i) location, ii) size, and iii) characteristics of the pancreatic lesion/s. Procedures involving solid pancreatic lesions only were selected for this review. Patients with EUS FNA/TCB of peripancreatic lesions, lymph nodes, or bileduct masses were excluded from the study.
EUS FNA and TCB
The linear Olympus echoendoscopes GFUC140P and GF-UCT140 (Olympus America Corp., Melville, NY, USA) with the Aloka (Prosound SSD 5000, Wallingford, CT, USA) processor were used in all cases for EUS guided sampling. Conscious sedation using intravenous meperidine and midazolam was used in all cases. None of the patients required monitored anesthesia care. All patients were carefully monitored to ensure recovery and discharged within 2 hours postprocedure. A trained nurse coordinator involved in the case called each patient within 24-48 hours after the EUS to assess for complications which if present are entered into the EUS database. Each lesion was initially sampled by EUS FNA using a 22- gauge needle in all cases (Echotip, Wilson- Cook, Winston-Salem, NC, USA) with 10 mL of suction applied for at least 10 to-andthrough movements of the needle through the mass. The cytological specimen was placed onto a glass slides and fixed in alcohol. Papanicolaou stain was performed for immediate reading by experienced cytopathologist. In most patients at least 5-7 FNA passes were done. Pancreatic corebiopsy (EUS TCB) was obtained using a 19- gauge TCB needle (Quick Core, Wilson- Cook, Winston-Salem, NC, USA) in selected patients. EUS TCB was performed when: i) lesion was technically accessible via the gastric wall and the size of the lesion was at least 20 mm with no intervening vessel(s), absence of normal pancreatic parenchyma, main pancreatic duct or bile duct in the TCB needle’s projected path; ii) lesions in the pancreatic head/uncinate, TCB was attempted only after initial review of FNA slides 3-4 passes failed to reveal malignant cells and there was favorable anatomy as describe. The trucut biopsy needle was prepared in a standard fashion by a nurse-assistant pulling back the spring-loaded handle as reported previously [7]. At least two core samples were obtained per patient. Formalin was used for preservation of the TCB specimen for histopathology analysis. No touch prep was used in the room. Two different pathologists reviewed the specimens for histopathology and cytology. For data analysis, the patients were divided in two groups: EUS FNA only and EUS FNA+TCB (combination).
Final Diagnosis
Confirmed malignancy on follow-up was defined as: i) death from pancreatic cancer; ii) surgery with resection or biopsy confirming malignancy; iii) progression of disease based on radiological or clinical data; or iv) histological evidence of malignancy on core biopsy. Presence of either ‘atypical’, ‘suspicious’ or ‘abnormal cells’ on cytology were interpreted as a negative result for malignancy in our study. In order to ensure that no malignancy developed in any of the patients with a final diagnosis of a benign disease, patients were followed for at least 6 months.
ETHICS
Detailed informed consent for EUS FNA alone or combined with TCB was obtained from all patients before the procedure. This study was approved by the University of Miami Institutional Review Board (IRB number #2006715). The study protocol conforms to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects".
STATISTICS
Statistical analyses were performed using the SAS package (Version 9.1; SAS Institute Inc., Cary, NC, USA). Characteristics of pancreatic cancer patients are presented as frequencies, means, standard deviations, and ranges [8]. The sensitivities, specificities, positive predictive values (PPV), the negative predictive values (NPV), and the frequencies of cases correctly classified by EUS FNA or EUS FNA+TCB were evaluated versus the final diagnosis together with their 95% confidence intervals (95% CIs) by using the GraphPad software (https://www.graphpad.com/ quickcalcs/ConfInterval1.cfm) [9]. The comparison of the characteristics between the FNA only and FNA+TCB groups was done using the Fisher's exact, the Student t, and the McNemar tests [8]. The product-limit method of Kaplan-Meier was used to estimate median survival times [10]. Two-tailed P values less than 0.05 were considered statistically significant. The power analysis and the calculation of the sample size were made by means of the PS software (Version 2.1.31; Department of Statistics, Vanderbilt University, Nashville, TN, USA; https://biostat. mc.vanderbilt.edu/twiki/bin/view/Main/Power SampleSize) [11, 12, 13].
RESULTS
Patients and Tumor Characteristics
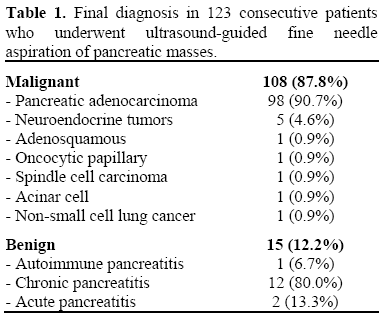
A total of 126 consecutive patients underwent EUS-guided biopsy of pancreatic masses during the study period. Three patients (2.4%) (two with positive FNA and one with a FNA negative for malignancy) were excluded from the final analysis because of insufficient clinical and imaging follow-up for confirmation of final diagnosis. The final cohort comprised 123 patients. There were 60 men and 63 women enrolled in the study. The final diagnosis was malignant in 108 patients (87.8%) and benign in 15 (12.2%). Pancreatic adenocarcinoma (90.7%) was the most frequent final pathological malignant diagnosis and chronic pancreatitis (80.0%) was the most frequent benign one (Table 1). The mean size of malignant and benign lesions was 30.5±9.4 mm (range: 8-68 mm) and 24.7±6.4 mm (range: 14-36 mm), respectively (P=0.024). A total of 72 patients (58.5%) underwent EUS-guided FNA alone and 51 (41.5%) underwent EUS FNA+TCB. The baseline characteristics of the two groups of patient are shown in Table 2. The two groups were similar as far as age, number of FNA passes, failure of prior biopsy, and pathological diagnosis are concerned, while a significantly higher percentages of males and tumors located in the head and uncinate were found in the FNA alone group.

Follow-up and Complications
The median survivals were 11 months (range: 5.0-27.2 months) and 8 months (range: 4.6- 27.2 months) in patients with malignant and benign disease, respectively. Among the two patients with shorter follow-up in malignant and benign diseases, one had resection of mass and the lesion resolved on CT, confirming the diagnosis of pancreatitis, in the other. Final diagnosis in our cohort of 123 patients was confirmed as follows (Table 3): 54 had died from pancreatic cancer at time of follow-up (35 FNA and 19 FNA+TCB), 28 (23 with malignant and 5 with benign diseases) were alive and had surgical confirmation (malignant: 17 FNA and 6 FNA+TCB; benign: 5 FNA), 13 were alive and had no surgery but had a positive histological biopsy (FNA+TCB), 18 had clinical or radiological progression of disease (10 FNA and 8 FNA+TCB). Ten patients with benign disease (5 FNA and 5 FNA+TCB) had no progression in follow-up and five patients (FNA) underwent surgery confirming benign disease. Minor complications from EUS guided biopsy were seen in three patients (2.4%): one patient developed periduodenal bleeding following biopsy that did not require transfusion and a small hematoma was developed during EUS but the patient was asymptomatic; one patient was admitted for abdominal pain 24 h after EUS, but no pancreatitis or bleeding was identified; the third patient had abdominal pain but was not admitted with resolution of pain within 24 h.

Results of EUS FNA Alone and EUS FNA Combined with TCB
The sensitivity for malignancy, specificity and frequency of cases correctly identified in the 72 patients who underwent EUS FNA were 87.1% (54/62; 95% CI: 76.1-94.3%), 100% (10/10; 95% CI: 69.2-100) and 88.9% (64/72; 95% CI: 79.3-95.1%) respectively (Table 4). The PPV of FNA was 100% (95% CI: 93.4-100%) and the NPV was 55.6% (95% CI: 30.8-78.5%).

In the group of the 46 patients with malignant lesion who underwent FNA+TCB, 21 patients (45.7%) had both FNA and TCB positive, 20 patients (43.5%) were positive at FNA alone, TCB correctly diagnosed cancer in three patients missed by FNA (6.5%), and in 2 cases (4.3%) the malignancy was not detected; therefore, FNA alone in this group of patients had a sensitivity of 89.1% (41/46; 95% CI: 76.4-96.4%) while TCB alone had a significantly (P<0.001; McNemar test) lower sensitivity of 52.2% (24/46; 95% CI: 37.0- 67.1%). The overall sensitivity of EUS FNA+TCB was 95.7% (44/46; 95% CI: 85.2- 99.5%) and the specificity was 100% (5/5; 95% CI: 47.8-100%; it should be pointed out that TCB failed to obtain tissue in 2 patients) and 96.1% (49/51; 95% CI: 86.5-99.5%) of the patients was correctly classified. The PPV of the combination was 100% (44/44; 95% CI: 92.0-100%) and the NPV was 71.4% (5/7; 95% CI: 29.0-96.3%). No significant differences in sensitivity, specificity, frequency of cases correctly classified, as well as PPV and NPV, were detected between the EUS FNA and EUS FNA+TCB groups (Table 4).
In seven patients, TCB failed to obtain a specimen (5 with malignancy). A mean of 2.7±1.0 (range 1-5) trucut passes were performed per patient. Ten patients in both groups had a false-negative EUS biopsy, eight had a lesion in the head/uncinate and were not sampled by EUS TCB. Five patients had a previous failed CT guided biopsy one had a previous failed EUS biopsy elsewhere. Therefore only four patients were undergoing their first pancreatic biopsy. The cytology on five patients showed atypical cells and benign cells on the other five. Patients with atypical cytology and final diagnosis of cancer were considered EUS false negative in our study.
DISCUSSION
Increasing the diagnostic accuracy of EUS guided biopsy for pancreatic lesions is a continuous challenge for endosonographers. Accuracy depends on many factors including: operator’s learning curve, availability of an experienced on-site cytopathology and tumor histopathological characteristics. Eloubeidi et al. [14] recently reported their experience of EUS FNA in 300 patients with pancreatic mass and demonstrated that proficiency increases over time as expertise with the procedure increases. However, even in expert hands, EUS FNA and cytological interpretation can be difficult in masses with a large amount of necrosis, chronic pancreatitis or in very well differentiated cancers. Endoscopic ultrasound guided trucut biopsy (EUS TCB) is emerging as a method that seeks to overcome the limitations of EUSguided fine needle aspiration (EUS FNA) by providing a core-tissue biopsy specimen [15]. Studies have suggested that there is a higher yield of EUS TCB over EUS FNA for GI stromal tumors [16] and lymphomas [17], but this was not shown in pancreatic malignancy [5]. However, case series have shown improved accuracy of EUS TCB over EUS FNA in autoimmune pancreatitis [18], chronic pancreatitis [19] and cystic pancreatic tumors [20]. Endosonographers in the USA have not fully embraced this technique due to its difficulty in sampling tissue from the duodenum, long tissue tray which limits full deployment of the needle in areas close to blood vessels and the additional cost of trucut needle.
Our retrospective study has some limitations because of the selection of patients for TCB in the body and tail of the pancreas. Nonetheless, TCB did not result in an improved accuracy in detecting malignancy over EUS FNA alone in pancreatic masses. The lack of benefit of additional TCB in our data may be explained by our high sensitivity of FNA alone. Our result is contrast to that previously reported by Wittman et al. in 83 patients with pancreatic masses [21]. The prospective study from Wittman et al. did not use on-site cytopathology and only performed up to four FNA passes and three TCB passes whereas we performed more FNA and TCB passes. The FNA sensitivity was 60% and increased to 76% for the combination suggesting a benefit of the combined approach when the FNA sensitivity is low. It should be taken into account that our results could be secondary to the presence of a type II error. Considering our FNA sensitivity of 87% in the FNA alone group, a FNA+TCB sensitivity of 93% would require a study population of at least 424 patients in order to demonstrate a significant advantage of additional EUS TCB (Figure 1, Table 5). A sensitivity higher than 93% of the combination FNA+TCB would demand less patients (e.g., 133 patients per group if a sensitivity of 97% would be reached) but these values are unlikely to be achieved in large cohort studies. Since the completion of this study in our Cancer Center, we have had any other case of FNA negative and trucut positive in pancreatic cancer. Therefore, increasing the sample size would not have changed much our conclusions. A lower FNA sensitivity may justify the use of additional TCB as demonstrated in the study by Wittman et al. [21]. The presence of on-site cytopathology might have improved our FNA sensitivity and further denied the benefit of combined TCB, thus our results cannot be applied to centers not using on-site cytopathology. It was not our intention to determine whether the combination without on-site cytopathology can replace EUS FNA plus the presence of on-site cytopathologist. Our study also cannot determine whether performing additional FNA passes instead of using TCB would improve EUS accuracy. This hypothesis seems unlikely because we have performed a mean of almost 7 passes per patient and have not seen much higher yield using more than seven FNA passes. A study comparing a fixed number of FNA versus FNA with additional passes versus FNA+TCB should be able to answer that question.
Figure 1. Relationship between sensitivity of
FNA+TCB (x axis) ad sample size needed to
demonstrate benefit of additional TCB at the Fisher’s
exact test with a fixed 87% sensitivity of FNA alone
(alpha value: 0.05; power: 0.80; PS software).

One of potential biases of our data is that our FNA+TCB group may be comprised of masses that are easier to sample by EUS as they are located in the body and tail of the pancreas. The sensitivity of FNA alone was not significantly different between the two groups (89% and 87%) indicating that selection bias towards TCB did not affect the yield of FNA. In other words, the lack of a difference was not due to a drop in FNA sensitivity in either group but the inability to increase diagnostic yield with TCB only providing diagnosis in three additional cases.
Based on this data, we now limit TCB to cases of failed FNA. This approach has been recently challenged in a study of 167 patients of solid lesions [22]. In this prospective trial a sequential sampling (TCB followed by FNA rescue) was equal to a dual sampling (92% and 93% diagnostic accuracy, respectively) with only 11% of patient requiring both sampling procedures. The results of this trial, however, cannot be applied to our data because the study included all types of solid lesions and excluded patients with tumors in the head of the pancreas in whom TCB would likely fail requiring rescue FNA more often.
The data for the subset of patients with pancreatic cancer (53 patients) is not reported; therefore, their results cannot, in our opinion, be generalized to pancreatic mass with FNA or TCB. As confirmed in this study, it has been our experience that TCB adds little to the sensitivity of FNA.
Our study also confirms a poor sensitivity (52%) of EUS TCB in pancreatic masses as reported by others [5, 6]. EUS TCB is difficult to perform in pancreatic lesions located in the head or uncinate as access is only possible through the distal stomach or the duodenum and from this position EUS TCB needle may fail to deploy and obtain a tissue core. The decreased performance is due to poor flexibility of the needle tip and the use of scope elevator to position the needle may result in disruption of the firing mechanism. Therefore, technical improvements in the EUS needle device are needed to allow improved tissue sampling when using a transduodenal approach. EUS TCB combined with FNA holds promise if most lesions can be sampled by TCB as suggested by a higher sensitivity in selected patients in our cohort (95%). We therefore feel that the use of EUS TCB for tissue sampling in accessible pancreatic masses be reserved for lesions that failed diagnosis by EUS FNA particularly if the mass is located in the body and tail where TCB can be easily performed. In uncinate lesions, a higher number of FNA passes (at least seven) should be able to maximize EUS yield. We performed a mean of 6.7 FNA passes to increase the diagnostic yield of EUS FNA in pancreatic masses. Performing several needle passes, EUS FNA is a safe procedure with complications reported in less than 0.5-2.5% of the cases [23, 24]. We had two minor complications in the group of patients with FNA alone and one in the group of patients who underwent combined FNA+TCB. The paucity of complications using additional EUS TCB can be explained by a very selective use of TCB in only 51 patients. We avoided TCB sampling through any normal pancreatic parenchyma to reduce the risk of pancreatitis or pancreatic duct injury. One of the complication occurred in a patient who underwent both EUS FNA and EUS TCB therefore it is not possible to know which of the two modalities resulted in bleeding.
In conclusion, adding EUS TCB to EUS FNA does not significantly improve the yield of EUS guided biopsy. Possibly molecular techniques applied to FNA cytological samples hold a better future than TCB in pancreatic masses.
Conflict of interest
The authors have no potential conflicts of interest
References
- Harewood GC, Wiersema MJ. Endosonographyguided fine needle aspiration biopsy in the evaluation of pancreatic masses. Am J Gastroenterol 2002; 97:1386-91. [PMID 12094855]
- Gress F, Gottlieb K, Sherman S, Lehman G. Endoscopic ultrasonography-guided fine-needle aspiration biopsy of suspected pancreatic cancer. Ann Intern Med 2001; 134:459-64. [PMID 11255521]
- Erickson RA, Sayage-Rabie L, Beissner RS. Factors predicting the number of EUS-guided fineneedle passes for diagnosis of pancreatic malignancies. GastrointestEndosc 2000; 51:184-90. [PMID 10650262]
- Wiersema MJ, Levy MJ, Harewood GC, Vazquez- Sequeiros E, Jondal ML, Wiersema LM. Initial experience with EUS-guided trucut needle biopsies of perigastric organs. GastrointestEndosc 2002; 56:275-8. [PMID 12145612]
- Larghi A, Verna EC, Stavropoulos SN, Rotterdam H, Lightdale CJ, Stevens PD. EUS-guided trucut needle biopsies in patients with solid pancreatic masses: a prospective study. GastrointestEndosc 2004; 59:185-90. [PMID 14745390]
- Varadarajulu S, Fraig M, Schmulewitz N, Roberts S, Wildi S, Hawes RH, et al. Comparison of EUSguided 19-gauge trucut needle biopsy with EUS-guided fine-needle aspiration. Endoscopy 2004; 36:397-401. [PMID 15100946]
- Levy MJ, Wiersema MJ. EUS-guided trucut biopsy. GastrointestEndosc 2005; 62:417-26. [PMID 16111962]
- Armitage P, Berry G, Matthews JNS. Statistical Methods in Medical Research. 4th Edition. Blackwell, Oxford, UK. 2001. [ISBN: 0632052570]
- Clopper C, Pearson S. The use of confidence or fiducial limits illustrated in the case of the binomial. Biometrika 1934; 26:404-13.
- Collett D. Modeling Survival Data in Medical Research. 2nd Edition. New York, NY, USA: Chapman & Hall/CRC Press, 2003. [ISBN: 1584883251]
- Casagrande JT, Pike MC. An improved approximate formula for calculating sample sizes for comparing two binomial distributions. Biometrics 1978; 34:483-6. [PMID 719125]
- Fleiss JL. Statistical Methods for Rates and Proportions 2nd Ed. New York, NY, USA: John Wiley, 1981:38-46.
- Dupont WD, Plummer WD Jr. Power and sample size calculations. A review and computer program. Control Clin Trials 1990; 11:116-28. [PMID 2161310]
- Eloubeidi MA, Tamhane A. EUS-guided FNA of solid pancreatic masses: a learning curve with 300 consecutive procedures. GastrointestEndosc 2005; 61:700-8. [PMID 15855975]
- Levy MJ, Jondal ML, Clain J, Wiersema MJ. Preliminary experience with an EUS-guided trucut biopsy needle compared with EUS-guided FNA. GastrointestEndosc 2003; 57:101-6. [PMID 12518144]
- Ribeiro A, Vernon S, Quintela P. EUS-guided trucut biopsy with immunohistochemical analysis of a gastric stromal tumor. GastrointestEndosc 2004; 60:645-8. [PMID 15472700]
- Eloubeidi MA, Mehra M, Bean SM. EUS-guided 19-gauge trucut needle biopsy for diagnosis of lymphoma missed by EUS-guided FNA. GastrointestEndosc 2007; 65:937-9. [PMID 17324409]
- Levy MJ, Reddy RP, Wiersema MJ, Smyrk TC, Clain JE, Harewood GC, et al. EUS-guided trucut biopsy in establishing autoimmune pancreatitis as the cause of obstructive jaundice. GastrointestEndosc 2005; 61:467-72. [PMID 15758927]
- DeWitt J, McGreevy K, LeBlanc J, McHenry L, Cummings O, Sherman S. EUS-guided trucut biopsy of suspected nonfocal chronic pancreatitis. GastrointestEndosc 2005; 62:76-84. [PMID 15990823]
- Levy MJ, Smyrk TC, Reddy RP, Clain JE, Harewood GC, Kendrick ML, et al. Endoscopic ultrasound-guided trucut biopsy of the cyst wall for diagnosing cystic pancreatic tumors. ClinGastroenterolHepatol 2005; 3:974-9. [PMID 16234042]
- Wittmann J, Kocjan G, Sgouros SN, Deheragoda M, Pereira SP. Endoscopic ultrasound-guided tissue sampling by combined fine needle aspiration and trucut needle biopsy: a prospective study. Cytopathol 2006; 17:27-33. [PMID 16417562]
- Aithal GP, Anagnostopoulos GK, Tam W, Dean J, Zaitoun A, Kocjan G, et al. EUS-guided tissue sampling: Comparison of dual sampling (trucut biopsy plus FNA) with sequential sampling (trucut biopsy and then FNA as required). Endoscopy 2007; 39:725-30. [PMID 17620230]
- Wiersema MJ, Vilmann P, Giovannini M, Chang KJ, Wiersema LM. Endosonography-guided fineneedle aspiration biopsy: diagnostic accuracy and complication assessment. Gastroenterology 1997; 112:1087-95. [PMID 9097990]
- Lee LS, Saltzman JR, Bounds BC, Poneros JM, Brugge WR, Thompson CC. EUS-guided fine needle aspiration of pancreatic cysts: a retrospective analysis of complications and their predictors. ClinGastroenterolHepatol 2005; 3:231-6. [PMID 15765442]


