Keywords
Pancreatitis, Chronic; Quality of Life; Surgical Procedures, Operative
INTRODUCTION
Chronic pancreatitis is an inhomogeneous clinical picture of multifactorial genesis and variable development. The predominant clinical symptom of patients with chronic pancreatitis is epigastric pain, which is sometimes difficult to manage by medication.
Although it is well known that pain is the main symptom of chronic pancreatitis, it has until now been assessed in very common and varying categories. Pain, however, is only one aspect of the large variety of sensitive facets of daily life. In addition to an improvement in pain symptoms and the preservation of pancreatic function, occupational rehabilitation of the mostly young patients [1, 2, 3] and an increase in the quality of life should influence the evaluation of therapeutic success and are considered aims of the therapy [2]. Measuring the quality of life by means of standardized parametric tests, which were initially introduced for the evaluation of oncological therapeutic regimes, is a method increasingly applied in the evaluation of surgical therapies [1, 3].
After the disease has progressed for years or even decades, the limit of analgesia is reached in many cases and, in addition to the severe long-term pain, organ complications occur which cannot be managed conservatively or interventionally. Therefore, surgery is indicated in almost every other patient, due to the progression of the disease. Besides improvement in pain symptoms and the management of organ complications, an improvement in the quality of life must be a major aim of surgical therapy. In order to compare the effectiveness of different therapeutic strategies for chronic pancreatitis, it is essential to collect data on the quality of life, which can only be evaluated properly if standardized methods are used [4].
The present paper evaluates the influence of different surgical methods of chronic pancreatitis on the early and late postoperative quality of life.
METHODS
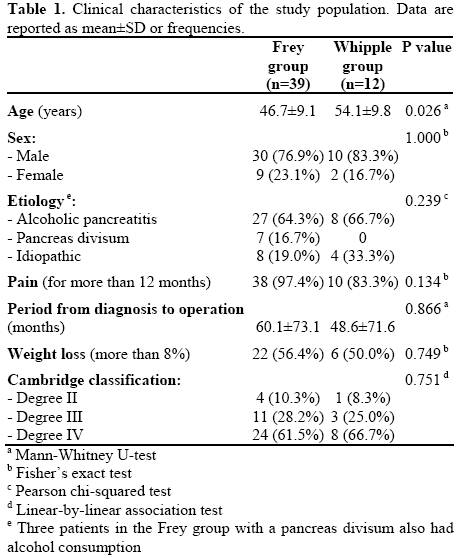
From March 2000 until April 2005, a total of 51 patients underwent surgical treatment for chronic pancreatitis in the Surgical Department of the Schleswig-Holstein University Hospital (Lübeck Campus). Of those 51 patients, 39 (76.5%) were operated on according to the Frey procedure, and in 12 cases (23.5%), a Whipple procedure was performed. Only those patients, for whom the diagnosis of chronic pancreatitis was confirmed histopathologically after surgery, were included in the evaluation.
There were 11 (21.6%) females and 40 (78.4%) males. The age span at the time of surgery was between 34 and 70 years, with an average value of 48.6 years (median: 47.5 years). Further characteristics of the study population are summarized in Table 1.
Surgery was indicated if conservative and endoscopic interventional techniques failed to yield therapeutic success. The method of surgery was mainly determined by the potentiality of a malignancy in the head of the pancreas. In cases with an increased CA 19-9 level, abnormalities in the head of the pancreas, documented by CT/endoscopic ultrasound, or questionable histopathological findings, a Whipple procedure was performed. In patients without potential malignancy, the Frey procedure was preferred.
Patient data were documented prospectively throughout the duration of the hospital stay. They included an exact patient history with respect to alcohol and analgesics, diagnoses of pancreatic insufficiency, diagnostic measures, and findings and information on the course of the surgery and postoperative progress. Information on the development of pain intensity, the new occurrence of diabetes mellitus and pancreoprivic maldigestion, as well as the long-term progress of the disease, were recorded retrospectively. For this purpose, 30 (76.9%) patients in the Frey group and 6 (50.0%) patients in the Whipple group were interviewed.
The resulting follow-up periods were between 20 and 90 months, with both average and median values of 50 months. Due to the differing follow-up periods, a comparison was also made with respect to the duration of the follow-up period.
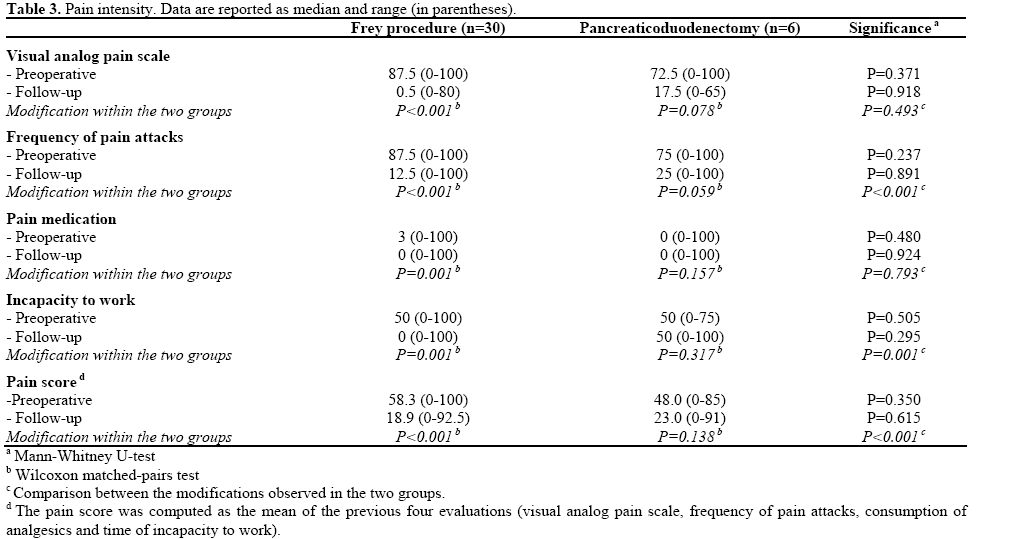
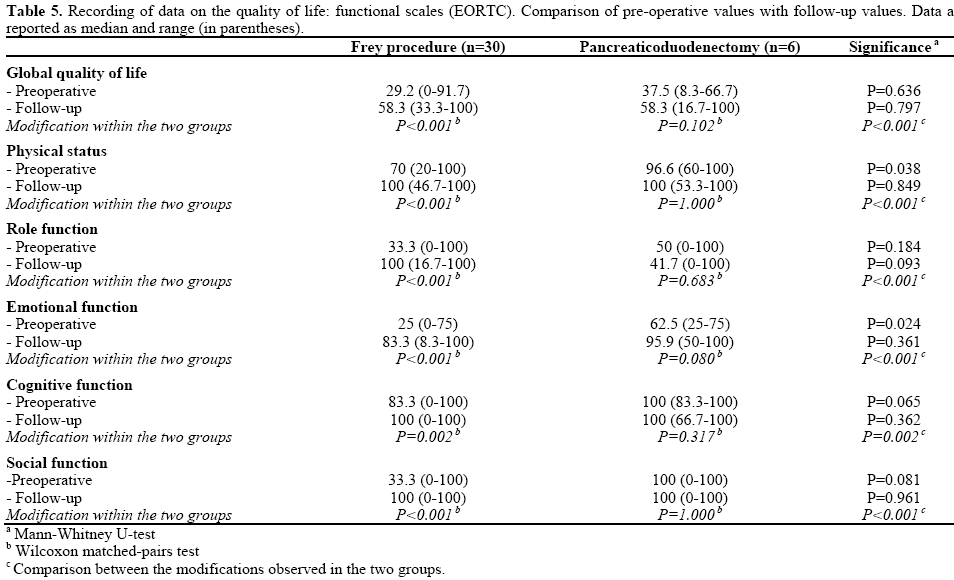
Pain intensity was evaluated by means of a predefined pain score, which includes a visual analog pain scale and the frequency of the pain attacks as subjective parameters, and the consumption of analgesics, as well as the time of incapacity to work, as objective parameters. These four evaluations were coded in 0- 100 scales (0: no pain, 100: maximum pain). The sum of the values divided by four yields the pain score. The pain score was evaluated as valid and reliable in patients with chronic pancreatitis by the working group of the University Medical Center in Hamburg- Eppendorf [2]. For quality of life assessment, a standardized questionnaire from the European Organization for Research and Treatment of Cancer (EORTC) was used [5]. The quality of life questionnaire contains 30 questions not specific to the disease, which serve to generate scales on symptoms, physical status, fitness for work, emotional, cognitive and social functions as well as on the general quality of life. The scales allow an assessment of the various aspects of the quality of life and not only to a global quality of life score.
ETHICS
Written informed consent was obtained from each patient. A study protocol or approval by a review committee was not necessary because there was no new treatment and we just performed a retrospective analysis of our treatment outcome.
STATISTICS
All the data collected were digitalized for statistical evaluation by Excel. Data evaluation was carried out by SPSS for Windows. Dependent variables, in particular for comparison of preoperative and postoperative results, were tested for significance using the Mann-Whitney rank test, the Wilcoxon matchedpairs rank test, the Fisher’s exact test, the Pearson chisquared, and the linear-by-linear association test. For comparative quantification, the P values of the test variables were given. Two-tailed P values less than 0.05 were significant.
RESULTS
Overall morbidity was 20.5% in the Frey group and 41.7% in the Whipple group. Thirty-day mortality was zero for all patients. Intraoperatively, there was one surgery-induced complication with injury of the portal vein and consecutive massive transfusion in the Whipple group. In the Frey group, one patient suffered an iatrogenic injury of the spleen during surgery, which was safely repaired by gluing the spleen. Two patients of the Frey group had to be reoperated, one due to diffuse bleeding and the other owing to an anastomotic insufficiency of the pancreaticojejunostomy. The most frequent complication developing after surgery was pneumonia, which occurred in 7.8% of all patients.
Average duration of surgery was 240 minutes for the Frey group and 360 minutes for the Whipple group. Further postoperative complications and clinically relevant parameters are summarized in Table 2.

Freedom from Pain
During the median follow-up period of 50 months, an improvement in the pain score was observed in 36 patients (92.3%) of the Frey group. One patient had a preoperative and postoperative score of 0 and one patient exhibited deterioration. Eight (66.7%) patients treated according to the Whipple procedure exhibited an improvement in their pain score during a median follow-up period of 50 months. In this group, one patient also had a score of 0 before and after surgery and one patient exhibited deterioration (Table 3).
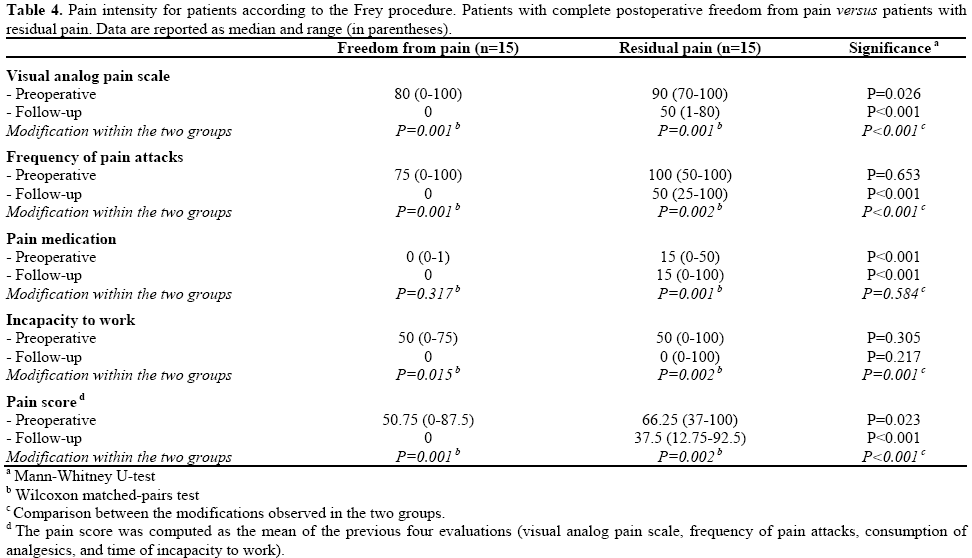
One-half of the patients in the Frey group reported the absence of pain after surgery. The remaining half exhibited an improvement in the pain score, and in pain intensity and frequency (Table 4).
Quality of Life
During the follow-up period, the indices for the global quality of life, and for both the physical and emotional status increased in both surgical groups. Cognitive and social functions increased in the Frey group after surgery while, in the Whipple group, the maximum had already been achieved prior to surgery. In the patients of the Whipple group, non-significant postoperative deterioration of the role function occurred (Table 5).
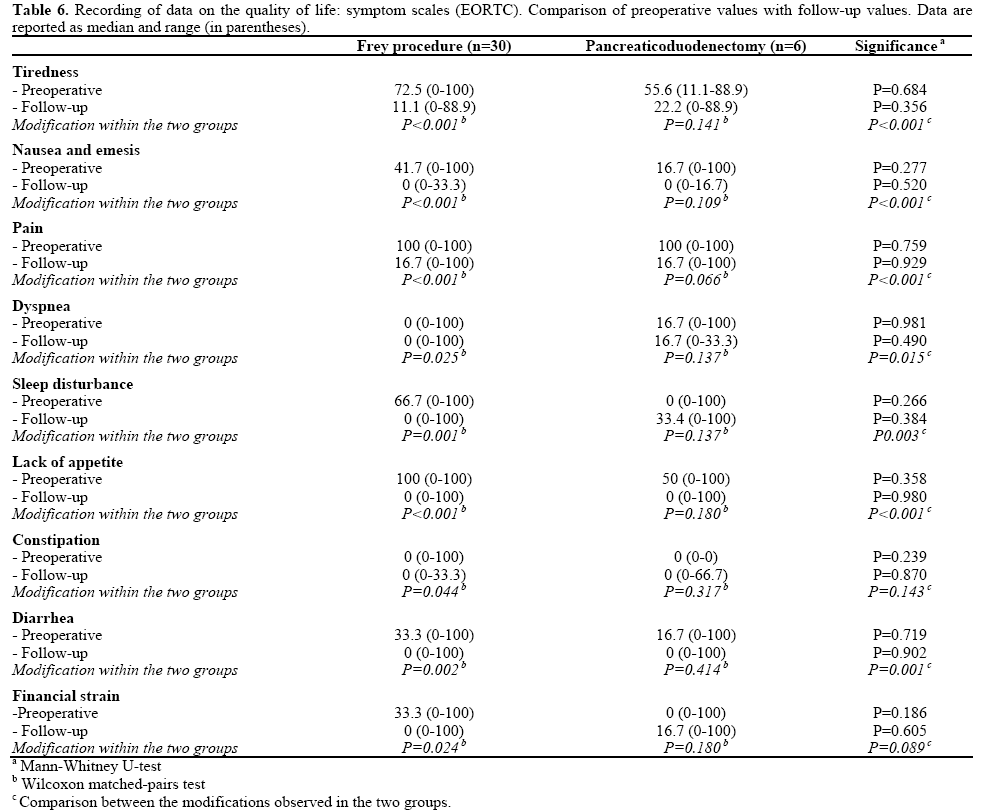
The patients of the Whipple group exhibited nonsignificantworse evaluations after surgery as far as the questions relating to insomnia and financial strain were concerned (Table 6). All other symptom scales improved in both groups, although they did not reach a significant level in the Whipple group due to the low number of cases.
Parameters Influencing the Quality of Life
Influence of the Follow-up Period
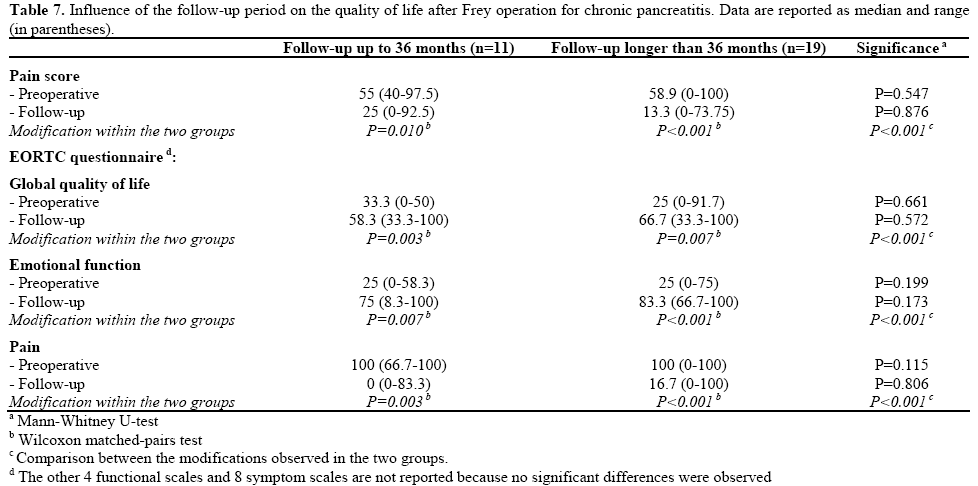
The average follow-up period of the 30 patients operated on according to the Frey procedure was 51 months, ranging from 20 to 90 months. Nineteen patients (63.3%) had a follow-up period of more than 36 months and, as opposed to the 11 patients (36.7%) with periods of up to 36 months, exhibited better postoperative results with respect to improvement in the pain score, the global quality of life and emotional function (Table 7).
Influence of Alcohol Consumption
Before surgery, 23 (76.7%) of the 30 patients operated on according to the Frey procedure reported regular high alcohol consumption. Six of these patients (26.1%) continued alcohol abuse after surgery and 17 patients (73.9%) became abstinent. No significant differences were observed in relation to alcohol consumption for all pain scores and EORTC scales (data not shown). Three of the six patients who continued alcohol consumption after surgery (50.0%) were rehospitalized, in contrast to a rehospitalization rate of 35.3% (6 out of 17 patients) for those who abstained from alcohol post-operatively.
Influence of Exocrine Pancreatic Insufficiency
Preoperative exocrine pancreatic function was limited in 15 (50.0%) patients in the Frey group, and 4 (66.7%) in the Whipple group had symptomatic exocrine pancreatic insufficiency before surgery. Post-operatively, 20 (66.7%) of the patients in the Frey group and 5 (83.3%) in the Whipple group received enzyme substitution as a therapy for exocrine pancreatic insufficiency. No significant differences were observed in relation to the presence/absence of exocrine insufficiency for all pain scores and EORTC scales (data not shown).
Influence of Diabetes Mellitus
A total of 5 patients (16.7%) in the Frey group had insulin-requiring diabetes mellitus before surgery whereas, after surgery, two patients (6.7%) exhibited clear improvement of the diabetic metabolic condition; glucose metabolism considerably deteriorated in five patients (16.7%). Three of the five patients developed diabetes which required insulin therapy, and the other two patients, who had pre-operatively undergone diabetes drug therapy, had to change to insulin after surgery. Postoperatively, 8 patients (26.7%) suffered from insulin-requiring diabetes mellitus.
In the Whipple group, one patient (16.7%) suffered from insulin-requiring diabetes mellitus before surgery. Postoperatively, there was a significant deterioration in the diabetic metabolic condition in three patients who had to switch to insulin therapy. Therefore, four of the six patients (66.7%) had insulin-requiring diabetes postoperatively.
No significant differences were observed in relation to the presence/absence of diabetes mellitus for all pain scores and EORTC scales (data not shown).
Influence of Pain
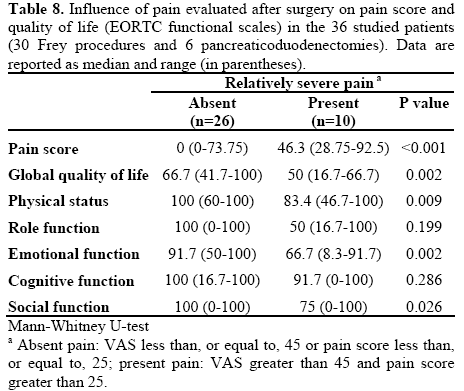
Before surgery, the mean VAS and pain scores were 45 and 25, respectively in the 36 patients studied (30 Frey procedures and 6 pancreaticoduodenectomies). Patients with above-average pain after surgery (i.e. both visual analog scale greater than 45 and pain score greater than 25) had worse results than patients without relatively severe pain (Table 8).
Age, sex and the time between the initial diagnosis of chronic pancreatitis and surgery did not have any significant influence on the postoperative outcome as far as evaluation of the quality of life and the pain score were concerned.
The average duct pressure was 33 cm water column and, on average, 11.4 g of pancreatic tissue was removed. In the Frey group, there was no significant relationship between duct pressure determined intraoperatively and the weight of the resected tissue.
As far as the origin of the disease is concerned, we did not see any differences in the results for alcoholic or idiopathic chronic pancreatitis (data not shown). In the Frey group, all four patients with duodenal stenosis were pain free postoperatively.
DISCUSSION
Chronic pancreatitis is primarily a disease which requires conservative treatment. Recent studies on long-term development, however, have shown that the majority of patients with chronic pancreatitis will not become pain-free, even after the disease has progressed for more than 10 years. In addition, until now, there has been no parameter which predicts long-term development for the patients [6].
Chronic pain syndrome and complications, such as bile duct stenosis, duodenal, pancreatic duct or vascular obstruction or symptomatic pancreatic pseudocysts, make patients seek surgical advice, frequently after years of progression. In the past, surgical procedures involving drainage as well as resection were employed successfully.
According to the pathophysiological processes, resective procedures have become most common as fundamental principles of surgical therapy in chronic pancreatitis. Worldwide, chronic inflammation of the pancreatic head accompanied by a tumor of unclear origin is treated by a partial pancreaticoduodenectomy according to the Whipple procedure even today [7]. Drawbacks of the surgery are, in addition to a high morbidity rate of up to 50% [1], the frequent occurrence of postoperative diabetes and maldigestion after pancreatectomy [2]. Loss of disease-free neighboring organs is an additional disadvantage of a partial pancreatectomy [1] and frequently leads to dumping complaints and episodes of cholangitis [2]. The pylorus-preserving modification of the traditional Whipple procedure failed to lead to a considerable improvement of the adverse aspects [1, 2, 3].
The relatively new surgical method according to Frey combines a longitudinal pancreaticojejunostomy with local resection of the pancreatic head, and is an alternative to a traditional partial pancreaticoduodenectomy [4]. The advantages of the organpreserving operative technique according to Frey are long-term freedom from pain, low morbidity and mortality as compared to the Whipple procedure and a low rate of newly occurring, postoperative diabetes mellitus [1, 2, 3].
Although pain is the main symptom of chronic pancreatitis, until now there have not been any uniform categories, which makes it difficult to interpret different therapeutic results. Furthermore, pain is one of several aspects to be included in assessing the quality of the therapy. Preservation of the pancreatic function, occupational rehabilitation [1, 2, 3] and an increase in the quality of life also have a decisive influence on the evaluation of therapeutic success [2].
Measuring the quality of life by means of standardized parametric tests, which had initially been introduced for the evaluation of oncological therapeutic regimes, is therefore an increasingly applied method in the evaluation of surgical therapeutic regimes [1]. In order to make it possible to compare the effectiveness of different therapeutic strategies of chronic pancreatitis, it is essential to collect data on the quality of life, which can only be evaluated properly if standardized methods are used; this is also true for the assessment of pain [4].
The results of existing studies cannot be compared easily because the definition of “freedom from pain” is often vague; not all patients receive the same therapy for the same indication [8], and postoperative results are recorded after follow-up periods which vary considerably. For a better overview, the following tables provide a comparison of the most important study results (Tables 9 and 10).
The results of our own and other studies show that both the Frey procedure and partial pancreaticoduodenectomy are capable of improving chronic pain symptoms and the quality of life in chronic pancreatitis patients. As far as later endocrine and exocrine pancreatic insufficiency is concerned, however, extended drainage surgery according to Frey proves to be advantageous as compared with the traditional resection procedures. In this context, the preservation of the gastroduodenal passage, and bile duct continuity seem to be of decisive importance for the regulation of exocrine secretion efficiency of the pancreas and glucose metabolism [12]. A study by Kahl et al. [14] showed that patients with endocrine and exocrine insufficiency had significantly lower indices for physical, emotional, cognitive and role functions. Our data do not detect any significant results in relation to exocrine insufficiency.
However, endocrine and exocrine insufficiency are frequently the lesser problem as compared to pain symptoms since pancreatic enzymes and insulin provide a very good conservative treatment measure.
Pain has a very adverse effect on the quality of life. Patients with a postoperative pain score of over 25 and a pain intensity of over 45 on the visual analog scale exhibited worse indices than the comparison group of patients, not only in pain score but in all functional scales of the quality of life.
The results of various studies suggest that the evaluation of pain and the quality of life depends on the duration of the follow-up period. A study in collaboration with Dr. CF Frey states that studies with a follow-up period of fewer than three years must be assessed skeptically [15] since pain attacks often recur during later development [16]. Our data cannot confirm this assumption and show better evaluations, particularly with respect to the pain score and the global quality of life, if the follow-up period exceeds 36 months as compared to the results of patients with a follow-up of less than 36 months.
CONCLUSION
For a patient with chronic pancreatitis, the decisive factor is the quality of life, especially as far as the question of pain and metabolic changes are concerned. Compared with other traditional surgical techniques, Frey’s drainage procedure with additional local resection of the pancreatic head seems to offer advantages with respect to long-term freedom from pain and the low risk of surgery-induced deterioration of pancreatic function. From our point of view, Frey’s procedure can be recommended as a new standard method of surgical therapy for chronic pancreatitis. This method provides us with an organ-preserving surgical principle for treating the complications of chronic pancreatitis without worsening the situation for the patient.
Conflict of interest
The authors have no potential conflict of interest
References
- Izbicki JR, Bloechle C, Knoefel WT, Kuechler T, Binmoeller KF, Soehendra N, Broelsch CE. Drainage versus resection in surgical therapy of chronic pancreatitis of the head of the pancreas: a randomized study. Chirurg 1997; 68: 369- 377
- Bloechle C, Izbicki JR, Knoefel WT, Kuechler T, Broelsch CE. Quality of Life in Chronic Pancreatitis - Results After Duodenum- Preserving Resection of the Head of the Pancreas. Panceas 1995; 11: 77-85
- Izbicki JR, Bloechle C. Drainage operation as therapeutic principle of surgical organ saving treatmant of chronic pancreatitis. Chirurg 1997; 68: 865-873
- Frey CF, Pitt HA, Prinz RA. A Plea for Uniform Reporting of Patient Outcome in Chronic Pancreatitis. Arch Surg 1996; 131: 233-234
- Aaronson NK, Ahmedzai S, Bergman B, Bullinger M, Cull A, Duez NJ, Filiberti A, Flechtner H, Fleishman SB, de Haes JC, et al. The European Organization for Research and Treatment of Cancer QLQ-C30: a quality-of-life instrument for use in international clinical trials in oncology. J Natl Cancer Inst 1993; 85: 365-376
- Lankisch PG, Löhr-Pappe A, Otto J, Creutzfeldt W. Natural Course in Chronic Pancreatitis. Digestion 1993; 54: 148-155
- Beger HG, Schoenberg MH, KH Link, Safi F, Berger D. Duodenum-preserving pancreatic head resection: a standard method in chronic pancreatitis. Chirurg 1997; 68: 874-880
- Lankisch PG. Chronic Pancreatitis -still a surgical disease? Chirurg 1997; 68: 851-854
- Frey CF, Amikura K. Local resection of the head of the pancreas combined with longitudinal pancreaticojejunostomy in the management of patients with chronic pancreatitis. Ann Surg 1994; 220: 492 - 507
- Izbicki JR, Bloechle C, Knoefel WT, Kuechler T, Binmoeller KF, Broelsch CE. Duodenum-preserving resection of the head of the pancreas in chronic pancreatitis. Ann Surg 1995; 221: 350 - 358
- Izbicki JR, Bloechle C, Broering DC, Knoefel WT, Kuechler T, Broelsch CE. Extended drainage versus resection in surgery for chronic pancreatitis. Ann Surg 1998; 228: 771 - 779
- Klempa I, Spatny M, Menzel J, Baca I, Nustede R, Stöckmann F, Arnold W. Pancreatic function and quality of life after resection of he head of the pancreas in chronic pancreatitis. Chirurg 1995; 66:
350-359
- Witzigmann H, Max D, Uhlmann D, Geissler F, Ludwig S, Schwarz R, Krauss O et al. Quality of life in chronic pancreatitis: A prospective trial comparing classical whipple procedure and duodenum-preserving pancreatic head resection. J Gastrointest Surg
2002; 6: 173 - 180
- Kahl S, Zimmermann S, Leodolter A, Glasbrenner B, Schulz HU, Johnson CD, Malfertheiner P. Quality of Life in Patients with Chronic Pancreatitis after Medical Treatment. Pancreatology 2001; 1:129- 199
- Ho HS, Frey CF. Current approach to the surgical management of chronic pancreatitis. Gastroenterologist 1997; 5: 128-136
- Harrison JL, Prinz RA. The surgical management of chronic pancreatitis: pancreatic duct drainage. Adv Surg 1999; 32: 1-21

