Keywords
Lymphatic Metastasis; Neoplasm Metastasis; Pancreatic Neoplasms; Round Ligament
INTRODUCTION
The incidence of pancreatic cancer has increased during the last decade and is ranked as the 4th leading cause of death in the United States [1]. The etiology of pancreatic cancer is poorly understood [2] and overall survival is only 4% [3].
Pancreatic cancer is characterized by early systemic dissemination and extraordinary local tumor progression [4]. Seventy-five percent of the patients diagnosed with pancreatic cancer have advanced disease [5]. Metastases are often present at the time of diagnosis. Common sites for metastases are the liver and the peritoneal cavity. Improvement in the preoperative workup has reduced the number of operations for non-resectable tumors in patients with tumors of the pancreatic head. A computed tomography scan is considered the gold standard in preoperative evaluation. However, its accuracy in detecting vascular involvement, liver or peritoneal metastasis is limited. Exploratory laparoscopy is an important tool in these patients’ workup but some authors call for its selective use. In our institution, as a result of a study we conducted on preoperative indicators for non-resectability, laparoscopy is performed only in patients with CA 19-9 levels higher than 300 U/mL [6]. Positron emission tomography combined with computed tomography is increasingly being used for a metastatic workup of pancreatic cancer, and some authors have reported a specificity and sensitivity of 94% and 90%, respectively [7].
During pancreatic surgery we routinely dissect the falciform and round ligaments and the surrounding fat for ease of retraction and exposure [8]. All resected tissues are routinely sent for pathological examination. In a busy pancreatic surgery center, this may impose extra work on the pathology laboratory.
In this study, we assessed whether the falciform and round ligaments are a possible site for metastases and whether routine pathology examination of these tissues is mandatory.
PATIENTS AND METHODS
Electronic charts of all patients who underwent pancreatic resection in the Department of Surgery at the Rambam Health Care Campus (RHCC), Haifa, Israel from June 2005 through January 2011 were retrospectively reviewed. The data collected included age, gender, type of operation performed, preoperative CA 19-9 levels, vascular and perineural invasion, level of tumor differentiation and pathological staging.
A unilateral left subcostal incision was performed for distal pancreatectomies and a bilateral subcostal was performed for subtotal, total and pancreaticoduodenectomies. Falciform and round ligaments were routinely resected and sent to the pathology lab in all operations in which the incision crossed the midline.
Only patients with adenocarcinoma of the pancreas were included; other periampullary tumors, such as duodenal carcinoma, ampullomas, tumors of the distal common bile duct and other pancreatic malignant (neuroendocrine), premalignant (intra-pancreatic mucinous neoplasm) or benign cystic lesions were excluded from the study.
Levels of CA 19-9 are expressed in U/mL with a reference range of 0-33 U/mL; the TNM staging system was used for postoperative pathological staging.
STATISTICS
Mean, standard deviation, range and frequencies were used as descriptive statistics. The one-way analysis of variance (ANOVA) and the linear-by-linear association chi-square test were applied to analyze data by running the SPSS for Windows (version 13.0) statistical package using a personal computer.
ETHICS
Informed consent was waived due to the retrospective nature of the study and the study protocol conformed to the ethical guidelines of the "World Medical Association Declaration of Helsinki - Ethical Principles for Medical Research Involving Human Subjects" adopted by the 18th WMA General Assembly, Helsinki, Finland, June 1964, as revised in Tokyo 2004, as reflected in a priori approval by the appropriate institutional review committee.
RESULTS
One hundred and 89 patients went through pancreatic resection in the study period; only 57 patients met the inclusion criteria for the study: 40 had had pancreaticoduodenectomies, 10 subtotal pancreatectomies, 2 total pancreatectomies, and 1 patient had a distal pancreatectomy with resection of the falciform ligament. Four patients had had an exploratory laparotomy but exploration revealed non-resectable (stage III) or metastatic (stage IV) disease. Table 1 depicts patient demographics as well as pre- and postoperative variables. Twenty-three patients (40.4%) had positive lymph nodes; the mean number of lymph nodes harvested was 12 and the mean positive to total lymph node ratio was 0.17.

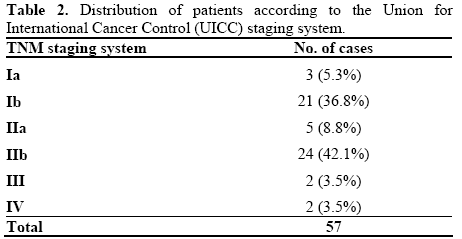
Table 2 depicts the pathological staging of the patients. We noted that 24 patients (42.1%) were in stage IIb.
The falciform and round ligaments were all negative for metastases, even when poor prognostic factors were present, such as perineural invasion (14 cases; 24.6%), vascular invasion (3 cases; 5.3%) and high CA 19-9 levels (mean CA 19-9 level was 448 U/mL; range: 0- 6,162 U/mL). Table 3 depicts the pathological staging of patients correlated to age, grade of differentiation and the described prognostic factors. The falciform and round ligaments were negative for metastases even in patients with unresectable (stage III) or metastatic disease (stage IV).

DISCUSSION
Metastatic pancreatic cancer is common and 75% of patients diagnosed with pancreatic cancer have either metastatic or locally advanced disease [5, 9]. The most common sites of metastasis are the liver and the peritoneal lining but unusual sites such as the lung, muscle, skin, heart, pleura, stomach, bone, umbilicus, kidney, appendix, spermatic cord and prostate have also been described [10, 11, 12, 13, 14, 15, 16, 17, 18, 19].
The falciform ligament is a broad and thin anteroposterior peritoneal fold, which is a remnant of the ventral mesentery of the fetus. It is attached to the undersurface of the diaphragm and the posterior surface of the right rectus sheath as low down as the umbilicus. On its right margin, it extends from the notch on the anterior margin of the liver as far back as the posterior surface. The two layers of the peritoneum are closely attached together and the free edges contain the round ligament and the paraumbilical veins. The round ligament, or ligamentum teres, is a degenerative string of tissue which anatomically divides the left lobe of the liver from the medial and lateral sections. The metastatic progression of pancreatic cancer is poorly understood; falciform ligament metastasis could occur by contiguous peritoneal spread, by hematogenous spread through the arterial and venous system or by lymphatic spread with extension along the round ligament. In the English literature, there are only scattered reports of falciform ligament metastasis from stomach and renal cell carcinoma [20, 21]. To our knowledge, pancreatic cancer metastasis to the falciform ligament has never been reported. In our study, none of the patients had falciform or round ligament metastases, even when poor prognostic markers were present (e.g., perineural invasion, high preoperative levels of CA 19-9, or poor pathological staging in resectable, non-resectable or metastatic disease).
CONCLUSIONS
Based on our study, we concluded that routine falciform and round ligament pathological examination is not indicated when these are removed during surgery for pancreatic cancer. This may reduce the workload on the pathology laboratory. Additional larger scale studies are needed to confirm and determine the real incidence of falciform and round ligament metastases from pancreatic cancer.
Conflicts of interest
The authors have no potential conflicts of interest
References
- American Cancer Society. Cancer Facts and Figures 2010. Atlanta, GA, USA: American Cancer Society, 2010.
- Silverman DT, Schiffman M, Everhart J, Goldstein A, Lillemoe KD, Swanson GM, et al. Diabetes mellitus, other medical conditions and familial history of cancer as risk factors for pancreatic cancer. Br J Cancer 1999; 80:1830-7. [PMID 10468306]
- Greenlee RT, Murray T, Bolden S, Wingo PA. Cancer statistics, 2000. CA Cancer J Clin 2000; 50:7-33. [PMID 10735013]
- DiMagno EP, Reber HA, Tempero MA. AGA technical review on the epidemiology, diagnosis, and treatment of pancreatic ductal adenocarcinoma. Gastroenterolgy 1999; 117:1464-84. [PMID 10579989]
- Neoptolemos JP, Dunn JA, Stocken DD, Almond J, Link K, Beger HG, et al. Adjuvant chemoradiotherapy and chemotherapy in resectable pancreatic cancer: a randomised controlled trial. Lancet 2001; 358:1576-85.
- Dorffman T, Eshkenazy R, Brauner E, Assi Z, Ariche A, Kluger Y. Preoperative indicators for non- resectability of patients with carcinoma of the head of the pancreas. HPB 2010; 12:243.
- Czernin J. PET/CT: Imaging structure and function. J Nucl Med 2004; 45(Suppl 1):1S-103s.
- Fischer J, Bland K, Callery M, Clagett G, Jones D. Mastery of Surgery. 5th ed. Philadelphia, PA, Lippincott Williams & Wilkins, 2006.
- Evans DB, Abbruzzese JL Willett CG. Cancer of the pancreas. In: Cancer: Principles and Practice of Oncology, Sixth Edition: De Vita VT, Hellman S, Rosenberg SA, eds Philadelphia, PA. Lippincott Williams and Wilkins, 2001:1126-1161.
- Wafflart E, Gibaud H, Lerat F, de Kersaint-Gilly A, Leborgne J. Muscular metastases of cancer of the pancreas. J Chir (Paris) 1996; 133:167-70. [PMID 8761070]
- Otegbayo JA, Oluswasola OA, Akere A, et al. Pancreatic carcinoma presenting as cutaneous nodules in a diabetic Nigerian male. West Afr J Med 2005; 24:180.
- Robinson BW, Lewis RR. Myocardial metastases from carcinoma of pancreas presenting as acute myocardial infarction. JR Soc Med 1982; 75:560-2.
- Turiaf J, Battesti JP, Basset F, Degos JD. Metastatic pleurisy in pancreatic cancer with the presence of considerable quantities of amylase in the pleural effusion and a major paraneoplastic peripheral neurologic syndrome. Ann Med Interne (Paris) 1969;120:449-58. [PMID 4309013]
- Takamori H, Kanemitsu K, Tsuji T, Kusano S, Chikamoto A, Okuma T, Iyama K. Metastatic gastric tumor secondary to pancreatic adenocarcinoma. J Gastroenterol 2005; 40:209-12. [PMID 15770407]
- Crescentini F, Deutsch F, Sobrado CW, et al. Umbilical mass as the sole presenting symptom of pancreatic cancer: a case report. Rev Hosp ClinFac Med Sao Paulo 2004; 59:198-202.
- Martino L, Martino F, Coluccio A, Mangiarini MG, Chioda C. Renal metastases from pancreatic adenocarcinoma. Arch Ital Urol Androl 2004; 76:37-9. [PMID 15185821]
- Filik L, Ozdal-Kuran S, Cicek B, Zengin N, Ozyilkan O, Sahin B. Appendicular metastases from pancreatic adenocarcinoma. Int J Gastrointest Cancer 2003; 34:55-8. [PMID 15235136]
- Bandyopadhyay D, Kapadia CR, Da Costa PE. Pancreatic carcinoma: report of two cases presenting with unusual metastases. Indian J Gastroenterol 2005; 24:75-6. [PMID 15879657]
- M. J. Borad, H. Saadati, and H. Saadati. Skeletal metastases in pancreatic cancer: a retrospective study and review of the literature Yale Journal of Biology and Medicine, vol 82, no 1, pp 1-6, 2009.
- Merseburger AS, Muller CC, MerseburgerSchonborn CT, et al. A rare case of isolated prostate metastasis from primary pancreatic cancer. Urologe A. 2005; 44:527-9.
- A. Shah, A. Dayal,V. Shanbough. Umbilical nodule. An indicator of intra abdominal malignancy. The Internet Journal of Surgery 2009 Volume 19 Number 1.

