Keywords
Fibrosis; Gene Expression Profiling; Immunohistochemistry; In Situ Hybridization; Interleukin-8; Pancreatic Diseases; Pancreatitis
Abbreviations
GRO/CINC: growth-regulated gene product/cytokine-induced neutrophil chemoattractant; ISH: in situ hybridization
INTRODUCTION
Interleukin (IL)-8 is a member of the C-X-C chemokine family which mediates the recruitment of polymorphonuclear neutrophils, basophils, eosinophils and lymphocytes to inflammatory sites [1]. IL-8 acts as both a neutrophil activator and a chemoattractant [2]. Growth-regulated gene product/cytokine-induced neutrophil chemoattractant (GRO/CINC)-1 in rats corresponds to IL-8 in humans [3]. GRO/CINC-1 consists of 72 amino acids which are homologous to human peptides with melanoma growth stimulatory activities, indicating that GRO/CINC-1 has a structural and functional homology to human IL-8 [3]. GRO/CINC-1 or IL-8 is expressed in experimental models such as gastric ulcer [4], ischemia-reperfused liver [5] and acute pancreatitis [6].
In humans, serum levels of IL-8 are reported to be an early predictor of disease severity and complications in acute pancreatitis [7]. An anti-IL-8 neutralizing antibody inhibited cytokine response and acute lung injury in experimental acute pancreatitis [8]. Although IL-8 mRNA was recently reported to be expressed in human chronic pancreatitis [9, 10], the role of IL-8 in the pathogenesis of chronic pancreatitis is still unclear. It is often difficult to obtain chronic pancreatitis tissue, especially surgical specimens, in clinical settings. Obstructive pancreatitis is a specific form of pancreatitis, which is caused by the obstruction of the main pancreatic duct due to tumors or some other causes. Obstructive pancreatitis is different from chronic pancreatitis caused by alcohol abuse or cholelithiasis. However, obstructive pancreatitis tissue is often available at pancreatic surgery, and analysis of IL-8 expression in obstructive pancreatitis might provide some insight into the significance of IL-8 in the pathogenesis of chronic pancreatitis or pancreatic fibrosis.
In the present study, we attempted to assess the involvement of IL-8 in human obstructive pancreatitis.
MATERIALS AND METHODS
Patients
Fifteen cases of pancreatic cancer (14 cases of ductal adenocarcinoma and 1 case of islet cell carcinoma), 7 cases of mucinous cystadenoma, and 3 cases of Vater’s papilla cancer were studied. All cases were diagnosed histopathologically. The mean age of the 25 analyzed patients was 63.0±6.6 years (range: 51-74 years); 15 were males and 10 were females. Nine patients with normal pancreases were also included in this study; the gender (5 males, 4 females) and ages (mean 61.0±5.1 years; range: 54-69 years) of these patients were not significantly different from those of pancreatic cancer patients (P=1.000 and P=0.401, respectively).
Pancreatic Tissue
All pancreatic tissue was obtained at surgery; 25 specimens of obstructive pancreatitis portions from the patients with the above diseases and 9 specimens of normal pancreatic tissue were analyzed. Normal pancreatic tissue was obtained from patients with illnesses other than pancreatic disease and was confirmed to be histologically normal.
Immediately after surgical removal, all pancreatic tissue samples were fixed in 10% formalin, and sectioned at a thickness of 4 mm. The sections were stained with hematoxylin and eosin (H&E), and the severity of obstructive pancreatitis was graded from the viewpoint of pancreatic fibrosis as follows: grade 1 (mild), the percentage of fibrotic area in the total specimen was less than 25%; grade 2 (moderate), the fibrotic involvement was between 25 and 50%; grade 3 (severe), the fibrotic involvement was greater than 50%.
Immunohistochemistry
We used a DAKO LSAB kit (DAKO, Carpinteria, CA, USA) for in situ hybridization (ISH). The sections were incubated with a monoclonal anti-human IL-8 antibody (1:25 dilution, Genzyme, Minneapolis, MN, USA) overnight at 4°C. Normal mouse IgG was used as a negative control. The immunohistochemical reactivity of IL-8 was evaluated in each cell type as the frequency (in percentage) of pancreatic lobules displaying more than 20 cells which were positive for IL-8 expression [9].
In Situ Hybridization
An ISH kit (Maxim Biotech, Inc., San Francisco, CA, USA) was used. The hybridization was done at 42°C overnight, with 250 ng/mL of an oligonucleotide (30 mer) antisense human IL-8 probe (Biognostik GmbH, Göttingen, Germany). As negative control experiments, serial sections were hybridized with a sense probe. These probes were labeled with biotin using a DNA labeling kit (Biotin-High Prime, Boehringer Mannheim GmbH, Mannheim, Germany).
ETHICS
Informed consent was obtained from each patient and the study protocol conforms to the ethical guidelines of the 1975 Declaration of Helsinki as revised in 1983, as reflected in a priori approval by the Kanazawa University School of Medicine Review Committee.
STATISTICS
All data were expressed as mean, standard deviations, range, and frequencies. The Mann-Whitney, the Pearson chi-square, the Fisher's exact, and the McNemar tests were used to analyze differences in human IL-8 expression. Two-tailed P values less than 0.05 were considered statistically significant. The SPSS version 8.0 software (SPSS Inc., Chicago, Illinois, USA) was used for statistical analysis.
RESULTS
Histological Evaluation of Human Obstructive Pancreatitis
Pathological analysis revealed the histological characteristics of obstructive pancreatitis with heterogeneously extended fibrosis in the vicinity of damaged parenchyma. Mononuclear cell infiltrates and ductal proliferation were observed. As for histological severity, a representative figure for each grade is shown in Figure 1: grade 1 (mild, Figure 1a), 10 cases; graded 2 (moderate, Figure 1b), 6 cases; grade 3 (severe, Figure 1c), 9 cases. The 9 control specimens showed normal pancreatic histology (grade 0).
Figure 1. Different grades of pancreatic fibrosis in human chronic obstructive pancreatitis as defined in the section "Materials and Methods: Pancreatic Tissue" by hematoxylin and eosin staining. Mild, grade 1 (a); moderate, grade 2 (b); severe, grade 3 (c). (Original magnification: ´25).
IL-8 Expression in Human Obstructive Pancreatitis
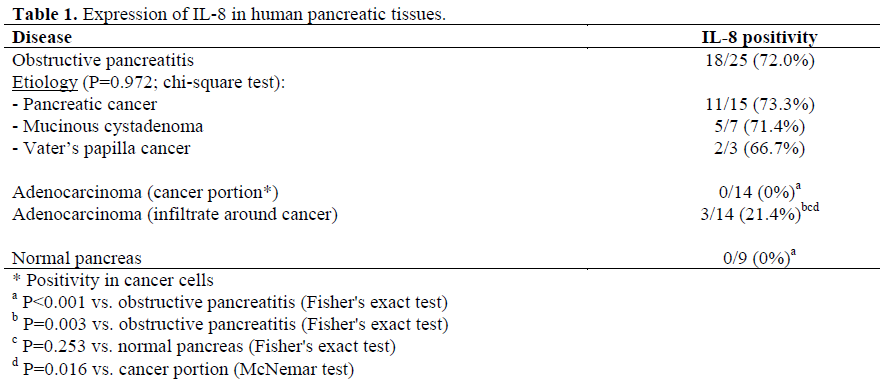
IL-8 was expressed in 72.0% (18/25) of obstructive pancreatitis specimens although the frequency of positive cells varied considerably among the samples. IL-8 was localized in the cytoplasm of acinar, ductal and inflammatory cells (Figure 2). Most IL-8- positive-infiltrates were seen in fibrotic areas. The relationship between the expression of IL-8 and the histological stage of chronic obstructive pancreatitis is shown in Figure 3. In grade 1 (mild), IL-8 was expressed mostly in acinar cells, whereas in grade 2 (moderate) and 3 (severe), IL-8 expression was found to be increased in the inflammatory infiltrates and ductal cells.
Figure 2. IL-8 expression in pancreatic tissue sections from patients with CP. IL-8 protein is localized in the cytoplasm of acinar and stromal infiltrating cells (a). Proliferating ductular cells were also positive for IL-8 (b). Immunohistochemistry (magnification: ´25, inset ´100).
Figure 3. IL-8 protein expression in pancreatic acinar, stromal and ductular cells in different grades of pancreatic fibrosis. IL-8 expression was semiquantified as defined in the section "Materials and Methods: Immunohistochemistry".
IL-8 immunoreactivity data are shown in Table 1. The positivity of IL-8 was not significantly related to the etiology of obstruction (P=0.972). In the normal human pancreases, IL-8 immunoreactivity was absent (P<0.001 vs. obstructive pancreatitis) and it was not expressed in any adenocarcinoma tissue (P<0.001 vs. obstructive pancreatitis). In 3 (21.4%) of the 14 adenocarcinoma lesions examined, IL-8 immunoreactivity was present in infiltrates around cancer cells (P=0.003 vs. obstructive pancreatitis; P=0.253 vs. normal pancreas; P=0.016 vs. cancer portion of adenocarcinoma). These 3 cases also had positive IL-8 immunoreactivity in the obstructive pancreatitis portions.
IL-8 mRNA Expression in Human Obstructive Pancreatitis
The localization of the mRNA was similar to that of the protein. IL-8 mRNA was localized in acinar, inflammatory and ductal cells in serial sections of obstructive pancreatitis (Figure 4), whereas it was not expressed in the normal pancreas and cancer cells.
Figure 4. IL-8 mRNA is expressed in acinar cells (a) and infiltrating inflammatory cells (b). In situ hybridization (magnification: ´25; inset: ´100).
DISCUSSION
Major etiologies of chronic pancreatitis are alcohol abuse and gallstones, but obstructive pancreatitis [11] develops due to the stricture or obstruction of the main pancreatic duct by post-inflammatory fibrosis, stones or tumors [12]. We attempted to assess whether IL-8 expression is involved in the pathophysiology of obstructive pancreatitis.
In previous reports, the main source of IL-8 was inflammatory cells, including neutrophils [13]. Saurer et al. [9] demonstrated that IL-8 mRNA is expressed in acinar, ductal and infiltrating cells in human chronic pancreatitis using in situ hybridization, which is consistent with our results. However, they did not study the expression of IL-8 protein. Different results for IL-8 protein and mRNA have been reported in alcoholic liver disease [14]. In the present study, we have clearly shown that the expression of IL-8 protein is up-regulated in pancreatic lobules with histopathologic alterations of obstructive pancreatitis. The distribution of IL-8 protein was consistent with that of IL-8 mRNA. Therefore, IL-8 was obviously expressed in obstructive pancreatitis, whereas it was not found in the normal pancreases and in pancreatic cancer. In other human chronic diseases, including idiopathic pulmonary fibrosis [15], and cystic fibrosis [16], an enhanced expression of IL-8 has been associated with fibrosis. Although no direct link between IL-8 and pancreatic fibrosis has been proven, Andoh et al. [17] reported that TNF-alpha and IL-1beta regulate IL-8 production in pancreatic periacinar myofibroblasts and that most IL-8-positive infiltrates were located in the vicinity of fibrotic areas.
IL-8 expression is related to the histological activity of inflammation in inflammatory bowel diseases [18]. In the pancreas, it is reported that IL-8 gene expression in the pancreatic parenchyma is frequently observed in advanced grades of the disease. Our results do not fully support this report. In the present study, IL-8 was expressed mostly in acinar cells in mild obstructive pancreatitis, whereas its expression was increased in interstitial infiltrating cells in moderate and severe obstructive pancreatitis, suggesting that the type of cells expressing IL-8 differs depending on the histological grade of obstructive pancreatitis. The differences might be explained by the etiologies of pancreatitis. Saurer’s study [9] was carried out, for the most part, on alcoholic chronic pancreatitis, whereas our study was on obstructive pancreatitis.
The important early mechanism of progressive fibrosis in chronic obstructive pancreatitis is considered to be increased ductular pressure and acinar damage releasing local proinflammatory cytokines which stimulate peri-acinar stellate cells to accelerate pancreatic fibrosis. Animal experiments and some clinical studies show that obstructive pancreatitis can be reversible if the obstruction is released. This reversibility could partly explain the changing source of IL-8 during the development of fibrosis.
The overexpression of IL-8 in pancreatic cancer is predominant in regions exposed to hypoxia after orthotopic implantation in the pancreases of nude mice [19]. During the development and progression of pancreatic cancer, the expression of iNOS and protein tyrosine nitration is increased, indicating the potential involvement of oxidative stress [20]. The overexpression of iNOS has been reported in human chronic pancreatitis [21]. A significant association between NO and IL- 8 is also reported in human chronic obstructive pulmonary disease [22]. We speculate that IL-8 induction is associated with oxidative stress in obstructive pancreatitis.
The pathophysiology of pain in chronic pancreatitis is not yet fully understood, but it was recently reported that IL-8 is expressed in macrophages surrounding enlarged pancreatic nerves [10]. Substance P is released from sensory pancreatic nerves and directly stimulates the release of IL-8 from macrophages [23]. Such interaction between inflammatory cells and nerves could be called “neuroimmune cross talk” [23], and may be involved in the generation of pain in chronic pancreatitis. Our study showing the changing source of IL-8 in different cell types in the course of obstructive pancreatitis would suggest a role of IL-8 in the intrinsic maintenance of the inflammatory response, thus sustaining the progression of obstructive pancreatitis.
In conclusion, the present study shows that IL-8 is expressed in the pancreas of patients with obstructive pancreatitis with different expression sites depending on the grade of pancreatic fibrosis.
References
- Baggiolini M, Walz A, Kunkel SL. Neutrophilactivating peptide-1/ interluekin-8, novel cytokine that activates neutrophils. J Clin Invest 1989; 84:1045-9. [PMID 2677047]
- Rajarathnam K, Sykes BD, Kay CM, Dewald B, Geiser T, Baggiolini M, Clark-Lewis I. Neutrophil activation by monomeric interleukin-8. Science 1994; 264:90-2. [PMID 8140420]
- Watanabe K, Suematsu M, Iida M, Takaishi K, Iizuka Y, Suzuki H, et al. Effect of rat CINC/gro, a member of the interleukin-8 family, on leukocytes in microcirculation of the rat mesentery. Exp Mol Pathol 1992; 56:60-9. [PMID 1547869]
- Yamada H, Takahashi S, Fujita H, Kobayashi N, Okabe S. Cytokine-induced neutrophil chemoattractants in healing of gastric ulcers in rats. Dig Dis Sci 1999; 44:889-95. [PMID 10235592]
- Matsumura F, Yamaguchi Y, Goto M, Ichiguchi O, Akizuki E, Matsuda T, et al. Xanthine oxidase inhibition attenuates Kupffer cell production of neutrophil chemoattractant following ischemiareperfusion in rat liver. Hepatology 1998; 28:1578-87. [PMID 9828222]
- Osman MO, Kristensen JU, Jacobsen NO, Lausten SB, Deleuran B, Deleuran M, et al. A monoclonal anti-inteleukin 8 antibody (WS-4) inhibits cytokine response and acute lung injury in experimental severe acute necrotising pancreatitis in rabbits. Gut 1998; 43:232-9. [PMID 10189850]
- Pezzilli R, Billi P, Miniero R, Fiocchi M, Cappelletti O, Morselli-Labate AM, et al. Serum interleukin-6, interleukin-8, and beta 2-microglobulin in early assessment of severity of acute pancreatitis. Comparison with serum C-reactive protein. Dig Dis Sci 1995; 40:2341-8. [PMID 7587812]
- Rau B, Steinbach G, Gansauge F, Mayer JM, Grunert A, Beger HG. The potential role of procalcitonin and interleukin-8 in the prediction of infected necrosis in acute pancreatitis. Gut 1997; 41:832-40. [PMID 9462219]
- Saurer L, Reber P, Schaffner T, Buchler MW, Buri C, Kappeler A, et al. Differential expression of chemokines in normal pancreas and in chronic pancreatitis. Gastroenterology 2000; 118:356-67. [PMID 10648464]
- Di Sebastiano P, di Mola FF, Di Febbo C, Baccante G, Porreca E, Innocenti P, et al. Expression of interleukin 8 (IL-8) and substance P in human chronic pancreatitis. Gut 2000; 47:423-8. [PMID 10940282]
- Lankisch PG, Banks PA. Chronic pancreatitis: etiology. In: Pancreatitis. Lankisch PG, Banks PA, eds. Berlin, Germany: Springer-Verlag, 1993:199-206.
- Singh SM, Reber HA. The pathology of chronic pancreatitis. World J Surg 1990; 14:2-10. [PMID 2407035]
- Bazzoni F, Cassatella MA, Rossi F, Ceska M, Dewald B, Baggiolini M. Phagocytosing neutrophils produce and release high amounts of the neutrophilactivating peptide 1/interleukin 8. J Exp Med 1991; 173:771-4. [PMID 1997655]
- Afford SC, Fisher NC, Neil DA, et al. Distinct patterns of chemokine expression are associated with leukocyte recruitment in alcoholic hepatitis and alcoholic cirrhosis. J Pathol 1998; 186:82-9. [PMID 9875144]
- Carre PC, Mortenson RL, King TE Jr, Noble PW, Sable CL, Riches DW. Increased expression of the interleukin-8 gene by alveolar macrophages in idiopathic pulmonary fibrosis. A potential mechanism for the recruitment and activation of neutrophils in lung fibrosis. J Clin Invest 1991; 88:1802-10. [PMID 1752942]
- Tabary O, Escotte S, Couetil JP, Hubert D, Dusser D, Puchelle E, Jacquot J. Genistein inhibits constitutive and inducible NF-KappaB activation and decreases IL- 8 production by human cystic fibrosis bronchial gland cells. Am J Pathol 1999; 155:473-81. [PMID 10433940]
- Andoh A, Takaya H, Saotome T, Shimada M, Hata K, Araki Y, et al. Cytokine regulation of chemokine (IL-8, MCP-1, and RANTES) gene expression in human pancreatic periacinar myofibroblasts. Gastroenterology 2000; 119:211-9. [PMID 10889171]
- Mazzucchelli L, Hauser C, Zgraggen K, Wagner H, Hess M, Laissue JA, Mueller C. Expression of interleukin-8 gene in inflammatory bowel disease is related to the histological grade of active inflammation. Am J Pathol 1994; 144:997-1007. [PMID 8178948]
- Shi Q, Abbruzzese JL, Huang S, Fidler IJ, Xiong Q, Xie K. Constitutive and inducible interleukin 8 expression by hypoxia and acidosis renders human pancreatic cancer cells more tumorigenic and metastatic. Clin Cancer Res 1999; 5:3711-21. [PMID 10589791]
- Vickers SM, MacMillan-Crow LA, Green M, Ellis C, Thompson JA. Association of increased immunostaining for inducible nitric oxide synthase and nitrotyrosine with fibroblast growth factor transformation in pancreatic cancer. Arch Surg 1999; 134:245-51. [PMID 10088562]
- Ganesh Pai C, Sreejayan, Rao MN. Evidence for oxidant stress in chronic pancreatitis. Indian J Gastroenterol 1999; 18:156-7. [PMID 10531717]
- Kanazawa H, Shoji S, Yoshikawa T, Hirata K, Yoshikawa J. Increased production of endogenous nitric oxide in patients with bronchial asthma and chronic obstructive pulmonary disease. Clin Exp Allergy 1998; 28:1244-50. [PMID 9824391]
- Di Sebastiano P, di Mola FF, Bockman DE, Friess H, Buchler MW. Chronic pancreatitis: the perspective of pain generation by neuroimmune interaction. Gut 2003; 52:907-11. [PMID 12740353]





