Keywords
Alkamleen locality; Facilitating an enabling environment; Integrating health services
Introduction
Primary health care (PHC) emphasizes universal access to health services. The movement was accompanied by an expansion of basic health services in developing countries provided by paramedical and community health workers. Inevitably some health workers worked in isolation, in remote rural areas, with problems communicating with the centre. Primary health care (PHC) is the first level of contact individuals, families and communities have with the health care system. Primary healthcare (PHC) refers to "essential health care" that is based on scientifically sound and socially acceptable methods and technology, which make universal health care accessible to all individuals and families in a community. International conference on primary health care. The Alma-Ata Declaration of 1978 emerged as a major milestone of the twentieth century in the field of public health and it identified primary health care as the key to the attainment of the goal of Health for All.
Selective primary health care
In response to the vagueness of primary health care and the conference of Alma Ata, an alternative movement began to gain momentum. This movement, termed Selective Primary Health Care (SPHC), emphasized the cost-effectiveness of vertical programs with measurable results. Primary health care has two meanings. The narrow definition (sometimes called primary medical care) focuses on the provision of medical services treating individual, generally acute medical conditions. It forms only a part of comprehensive primary health care which is the broader, holistic approach to health problems.
Health care delivery system reform
In the United States, two groups experience problems with their health care more intensely and more frequently than any other. One group is people with high health care needs and high costs — the 5 percent of the population that accounts for 50 percent of all health spending. Curative care refers to health care practices that treat patients with the intent of curing them, not just reducing their pain or stress. An example is chemotherapy, which seeks to cure cancer patients.
Medical definition of secondary care: Medical care that is provided by a specialist or facility upon referral by a primary care physician and that requires more specialized knowledge, skill, or equipment than the primary care physician can provide — compare primary care, tertiary care. Tertiary care is specialized consultative health care, usually for inpatients and on referral from a primary or secondary health professional, in a facility that has personnel and facilities for advanced medical investigation and treatment, such as a tertiary referral hospital Integration of primary health care is very important approach for sustaining healthcare system. In Sudan Many interrelated factors are jointly affecting the functionality of the integration between health projects. Some of those are staff shortages, continuing cost inflation, service demand and scarce resources. There is a critical need to seek out and apply the current knowledge on health systems integration to enhance efficient and effective health services. A study was conducted for investigating the factors affecting the integration between the health projects Definition of integration: Integration means coordination of health services and collaboration among provider organizations to create a real health system [1-10].
Rationale of the study
In some low- and middle-income countries, healthcare services are organized around a specific health problem. This can cause fragmentation as people are required to visit separate clinics depending on their health problem or need. On the other hand, separating out services for specific diseases can be inefficient for both the provider with service duplication, and the patient who has to visit different services for their health care. For example, a mother has to go to one clinic for family planning services and another for her children to be vaccinated, or a person with HIV and TB has to go to separate clinics for each disease.
Primary health care in Alkamleen locality
The primary health care in Alkamleen locality is currently being delivered through a multiple service/interventions, several vertical programs of public health services. There is duplication of effort, poor human resource, poor health provision/consumption and resource collapse. Verticality was seen to be as a result of not joining the provision of health services to the federal ministry of health, absent of policies and regulations and bad management.
Study Methodology
Study design
It is a pre-test – post-test control group design where all health personnel working at all health facilities in alkamleen locality will witness a training programme in integrated services at health facilities. That will be followed with a post intervention evaluation/study to assess the impact of the training programme in improving the provision of health services. Findings of the evaluation will be compared to the findings of the base line study conducted during the last year 2012. Control health facilities at another locality will be reached by the post intervention study.
Study area
The study area will be all the health facilities at Alkamleen locality, it is about 401,930 populations. Its area is 1750 km2; it composed of seven hospitals, forty eight health centers, forty dispensaries, one HIV centers and one TB centers.
Study population and targets
The health personnel providing the health services at the health facilities mentioned above will be targeted by the study intervention.
Study Results
Managers at 45 health facilities were met by the study (Annexure 1). The average number of the working force per a health facility was 6.6 persons (Min=1, Max=22). Table 1 shows the health cadre/total population proportion in the area. The average population served by the health facility were 6053 persons; (Min=1197*, health cadre population proportion=399), (Max=28154*, health cadre population proportion=2815.4).
| |
Name of the health facility |
No. of the health cadre |
Total population served by the health facility |
Health cadre population proportion |
| 1 |
Almnara/Alshekh Altayb |
1 |
1396 |
1396.0 |
| |
| 2 |
Altkena |
2 |
7893 |
3946.5 |
| 3 |
Albager Algdafy |
5329 |
2664.5 |
| 4 |
Algmlon Alsadana |
2451 |
1225.5 |
| 5 |
Altakla Hamd |
1539 |
769.5 |
| |
| 6 |
Botry |
3 |
6782 |
2260.7 |
| 7 |
Alhlela |
3420 |
1140.0 |
| 8 |
Abd Alla |
3305 |
1101.7 |
| 9 |
Alabdallab |
1767 |
589.0 |
| 10 |
Almhlj |
1653 |
551.0 |
| 11 |
Abo |
1197* |
399.0 |
| |
| 12 |
Klol |
4 |
5386 |
1346.5 |
| 13 |
Om Magad |
2992 |
748.0 |
| |
| 14 |
Alhaded 2/Omran |
5 |
4873 |
974.6 |
| 15 |
Flgala |
4046 |
809.2 |
| 16 |
Alhtela |
3904 |
780.8 |
| 17 |
Alsyed |
3647 |
729.4 |
| 18 |
Omrhy/Alshekh Altayb |
3306 |
661.2 |
| 19 |
Alsmer Alhela |
2878 |
575.6 |
| 20 |
Helt Hmd |
2565 |
513.0 |
| 21 |
Bet Alhaj |
2479 |
495.8 |
| 22 |
Alglfy |
1881 |
376.2 |
| 23 |
Alfdgoba |
1881 |
376.2 |
| 24 |
Dar Alslam |
6 |
6070 |
1011.7 |
| 25 |
Dr. Algady |
5357 |
892.8 |
| 26 |
Alkber |
5329 |
888.2 |
| 27 |
Altoraby |
4474 |
745.7 |
| 28 |
Aded Albshagra |
3733 |
622.2 |
| 29 |
Kab Alhdad |
3192 |
532.0 |
| 30 |
Alwaha |
3163 |
527.2 |
| |
| 31 |
Aldbaseen |
7 |
18237 |
2605.3 |
| 32 |
Habeba |
8748 |
1249.7 |
| 33 |
Om Dgrd |
8036 |
1148.0 |
| 34 |
Abo Oshar |
6782 |
968.9 |
| 35 |
Albager |
4987 |
712.4 |
| 36 |
Tkla |
4730 |
675.7 |
| |
| 37 |
Helt Abas |
8 |
3590 |
448.8 |
| 38 |
Aldera Alshrgya |
4246 |
530.8 |
| 39 |
Abros |
4046 |
505.8 |
| |
| 40 |
Aldera Algrbya |
9 |
9546 |
1060.7 |
| 41 |
Albanyo |
10 |
28154* |
2815.4 |
| |
| 42 |
Almsodyas |
20 |
13707 |
685.4 |
| |
| 43 |
Alsaha Almdrsa Alkamlen |
21 |
22341 |
1063.9 |
| 44 |
Alhaded 1 |
5010 |
238.6 |
| |
| 45 |
Altamen Alsehy |
22 |
22341 |
1015.5 |
| |
Table 1: Proportion of the health cadre to the total population in the area.
Health information system
All the managers (100%) at the health facilities reported the presence of a systematic and regular reporting system. However, 29 (64.4%) reported the presence of health information system at their health facilities while 16 (35.6%) didn't.
Working environment at the health facilities
Three indicators were set to appraise the working environment at the health facilities; those were 1- the general condition of the buildings (excellent, good, average), 2- size of the health facility (suitable, not suitable) in compare to the volume of health services provided and 3- the furniture condition (good and adequate, good and not adequate, not good and not adequate). The centers that obtained the best of those specifications (excellent, suitable, good and adequate) were evaluated as having an excellent working environment, those obtained two were evaluated as good, those obtained one were evaluated as fair while the centers attained none of the best specifications were evaluated as having a poor working environment. Figure 1 below shows that 10 (22.2%) were having excellent working environment while 17 (37.8%) were of poor working condition.
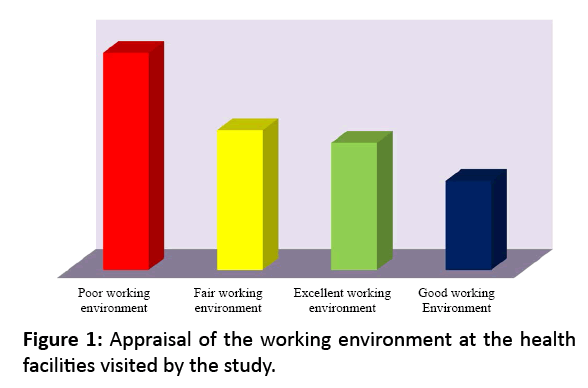
Figure 1: Appraisal of the working environment at the health facilities visited by the study.
Training in integration of provision of health services
A question was introduces about the integration between the health service programmes in the areas of planning process, supervision, reporting, distribution of recourses… etc. and whether the health personnel were attended a training programme in integration of provision of health services. All of the health managers (100%) reported that none of the health personnel have been trained in the integration between the health programmes in the provision of health services. Yet, a total of 18 (40%) managers reported the presence of integration system between the health service programmes while 27 (60%) didn’t (Figure 2). Of the total managers who affirmed the presence of the integration between the health programmes; only 2 (11.1%) reported that the delivery of the health service was ideally integrated.
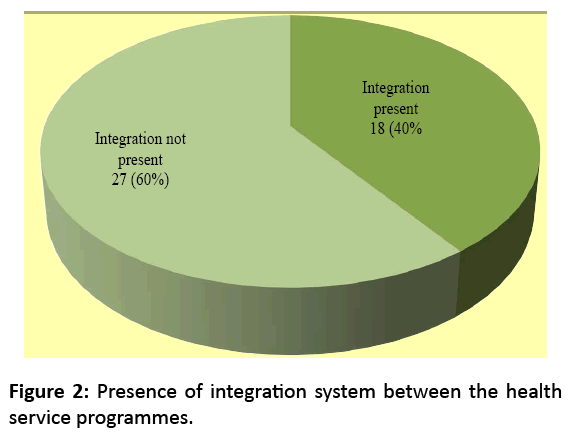
Figure 2: Presence of integration system between the health service programmes.
Strength of integration between programmes
Table 2 shows that 41 (91.1%) respondents reported that the integration was present between the Health Education, Nutrition, EPI and Maternal and Child Health programs while 4 (8.9%) reported between the Health Education and/or the Nutrition, EPI and Maternal and Child Health programs. The Health Education was the intersection programme between them.
| |
Total |
| H.E, NUT., EPI and MCH |
41 (91.1%) |
| H.E and/or NUT., EPI , MCH |
4 (8.9%) |
| Total |
45 (100.0%) |
Table 2: Distribution of the programmes integrated in the provision of health services.
Figure 3 shows that 38 (84.4%) respondents reported the presence of perfect integration between them while 7 (14.4%) reported a partial integration between them. The integration was realized in terms of cooperation among health cadre, logistics and supplies, reports writing and attendance of the monthly meetings.
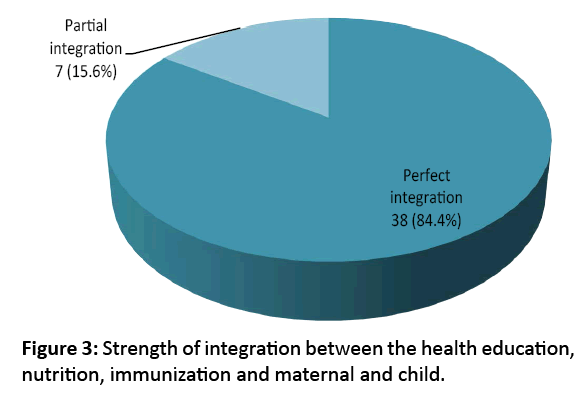
Figure 3: Strength of integration between the health education, nutrition, immunization and maternal and child.
Efficiency of health delivery packages
Five indicators were investigated to appraise the efficiency of the health delivery packages introduce by the health facilities, those were the presence of a manager, monitoring and evaluation system, supplies and equipments, communication system and presence of training programmes. Table 3 below shows that the EPI is topping the list where 44 (95.6%) of the total interviewed reported the presence of a responsible person and/or a manager who overseeing the delivery of EPI service, 37 (77.8%) reported the immunization technician, 42 (91.1%) reported the presence of monitoring and evaluation activity, 41 (91.1%) reported the presence of supplies and equipments and 42 (93.3%) managers reported the presence of training programmes in relation to EPI. However, the mental health, the aged and the health education were the least efficient health packages introduced; none of them was met any of the efficiency mental health indicators.
| |
Presence of manager |
Job name |
M & E |
Supplies and Equip. |
Communication |
Training |
| EPI |
43 (95.6%) |
Immun. Tech. (35:77.8%), Tech. preparation (6:13.3%), Medical assistant (1:2.2%) |
42 (93.3%) |
41 (91.1%) |
12 (26.7%) |
42 (93.3%) |
| GEN |
40 (88.9%) |
Doctors (19: 42.2%), Medical assistant (14: 31.1%), Immun. Tech. (1: 2.2%) |
40 (88.9%) |
38 (84.4%) |
4 (8.9%) |
39 (86.7%) |
| RES. |
40 (88.9%) |
Doctors (22: 48.9%), Medical assistant (19: 42.2%) |
39 (86.7%) |
37 (82.2%) |
2 (4.4%) |
39 (86.7%) |
| MCH |
38 (84.4%) |
Health visitors (15:33%), Mid wives (20:44.4%), doctor (1:2.2%) |
38 (84.4%) |
36 (80%) |
3 (6.7%) |
37 (82.2%) |
| DRG |
36 (80%) |
Doctors (10: 22.2%), Medical assistant (27: 60.0%), Pharmacists (2: 4.4%), Nurse (2: 4.4%), Other (2: 4.4%) |
35 (77.8%) |
34 (75.6%) |
2 (4.4%) |
33 (73.3%) |
| NCD |
35 (77.8%) |
Doctors (21: 46.7%), Medical assistant (14: 31.1%) |
34 (75.6%) |
34 (75.6%) |
2 (4.4%) |
34 (75.6%) |
| Nutri. |
30 (66.7%) |
Immun. Tech. (10: 22.2%), Mentor feed (10: 22.2%), Tech feed (5: 11.1%), volunteer (3: 6.7%) |
30 (66.7%) |
29 (64.4%) |
5 (11.1%) |
30 (66.7%) |
| CDC |
13 (28.9%) |
Doctors (8: 8.8%), Medical assistant (7: 15.6%), Other cadre (2: 4.4%) |
12 (26.7%) |
10 (22.2%) |
1 (2.2%) |
12 (26.7%) |
| DENT. |
4 (8.9%) |
Dentist (2:4.4%), Medical assistants (2: 4.4%) |
4 (8.9%) |
4 (8.9%) |
1 (2.2%) |
4 (8.9%) |
| Enviro. |
1 (2,2%) |
Immun Tech (1: 2.2%) |
1 (2.2%) |
1 (2.2%) |
1 (2.2%) |
1 (2.2%) |
| MENT |
1 (2,2%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| Aged |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| H.Edu. |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
Table 3: Distribution of efficiency indicators of health delivery packages introduced by the health facilities.
Crosscutting integration of the health delivery packages
Table 4 above shows a perfect integration between the EPI and the Nutrition programmes; that was reported by 40 (88.9%) of the total health managers met by the study. Findings show the each of the EPI and Nutrition programmes were of good integration with the health education programme as was reported by 35 (77.8%) and 31 (68.9%) health managers consequently. However the aged (GER), mental and dental health were seen to be stand vertically with no integration 0 (0%) with any of the health delivery packages.
| |
EPI |
EDU |
MCH |
NUT |
ENV |
CDC |
GEN |
DRG |
MEN |
NCD |
GER |
DEN |
RES |
| EPI |
|
35 (77.8%) |
31 (68.9%) |
33 (73.3%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| NUT |
40 (88.9%) |
34 (75.6%) |
28 (62.2%) |
|
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| EDU |
32 (71.1%) |
|
24 (53.3%) |
26 (57.8%) |
0 (0%) |
2 (4.4%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| MCH |
32 (71.1%) |
33 (73.3%) |
|
30 (66.7%) |
0 (0%) |
2 (4.4%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| DRG |
2 (4.4%) |
1 (2.2%) |
0 (0%) |
1 (2.2%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| RES |
0 (0%) |
4(8.9%) |
3 (6.3%) |
0 (0%) |
0 (0%) |
0 (0%) |
6 (13.3%) |
0 (0%) |
0 (0%) |
5 (11.1%) |
0 (0%) |
0 (0%) |
|
| NCD |
0 (0%) |
4 (8.9%) |
3 (6.3%) |
0 (0%) |
0 (0%) |
0 (0%) |
5 (11.1% |
2 (4.4%) |
0 (0%) |
|
0 (0%) |
0 (0%) |
4 (8.9%) |
| CDC |
0 (0%) |
2 (4.4%) |
1 (2.2%) |
0 (0%) |
1 (2.2%) |
|
1 (2.2%) |
1 (2.2%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| GEN |
0 (0%) |
3 (6.3%) |
0 (0%) |
0 (0%) |
0 (0%) |
1 (2.2%) |
|
5 (11.1%) |
0 (0%) |
4 (8.9%) |
1 (2.2%) |
0 (0%) |
5 (11.1% |
| ENV |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
1 (2.2%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| MEN |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
| GER |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
0 (0%) |
0 (0%) |
| DEN |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
0 (0%) |
|
0 (0%) |
Table 4: Cross-cutting integration of the health delivery packages introduced by the health facilities.
Conclusion
The working environment at most of the health facilities needs to be improved (that 10 (22.2%) were having excellent working environment while 17 (37.8%) were of poor working condition. Besides, the size of the health personnel working in the health facilities as not adequate with the population density served by those health facilities (average population served by the health facility were 6053 persons; (Min=1197*, health cadre population proportion=399), (Max=28154*, health cadre population proportion=2815.4).
Strategic and operational plans for the integration of health services were not in place the thing that reflects the ineffective coordination between the delivery services of health programmes.
Recommendations
• To improve the working environment at the health facilities in terms of buildings, infrastructure and foundation as well as the furniture, supplies and equipments.
• To increase the number of the health facilities and the number of the health cadre to secure a suitable health provider population proportion.
• To design a strategic and operational plans for integration of health services.
• To make use of the EPI experience in the integration of health delivery services
• To provide effective care coordination services between the health delivery programmes.
• To orient the health providers about the concept and train them on the mechanisms and the knowhow of providing integrated health delivery.
• To conduct health facility and community based consumer surveys to assess the proportion of the people reporting service coordinators help them get what they need.
• To replicate the conduction of this study at a wider scale.
References
- WHO. Integration of health care delivery: Report of a WHO Study Group. WHO Technical Report, Geneva, 1996; 861.
- Pedersen TÅ, Kowenz-Leutz E, Leutz A, Nerlov C. Cooperation between C/EBPα TBP/TFIIB and SWI/SNF recruiting domains is required for adipocyte differentiation. Genes & development 2001; 15: 3208-3216.
- IPPF W, UNAIDS U. Sexual & Reproductive Health and HIV Linkages: Evidence Review and Recommendations. 2008.
- Ekman F, Keränen A, Karvo J, Ott J. Working day movement model. Proceedings of the 1st ACM SIGMOBILE workshop on Mobility models, ACM 2008.
- Oliveiraâ€ÂÂÂÂCruz V, Kurowski C, Mills A. Delivery of priority health services: Searching for synergies within the vertical versus horizontal debate. Journal of International Development 2003; 15: 67-86.
- Dudley L, Garner P. Strategies for integrating primary health services in low-and middle-income countries at the point of delivery. Cochrane Database Systematic Reviews 2011; 7.
- Shigayeva A, Atun R, McKee M, Coker R. Health systems, communicable diseases and integration. Health Policy and Planning 2010; 25: i4-i20.
- Kerber KJ, de Graft-Johnson JE, Bhutta ZA, Okong P, Starrs A, et al. Continuum of care for maternal, newborn, and child health: From slogan to service delivery. Lancet 2007; 370: 1358-1369.
- Silow-Carroll S, Alteras T, Stepnick L. Patient-centered care for underserved populations: Definition and best practices: Economic and social research institute 2006.
- Muhammad Amir Khan. Public Health Consultant, Pakistan , Consultant Report on Integrated Services at Health Facilities in Sudan, 2011.

