Keywords
Pancreatitis
Abbreviations
CT computed tomography; NPO nil per os; PEG
percutaneous endoscopic gastrostomy
INTRODUCTION
Since its first description by Guadener in 1980 [1],
percutaneous endoscopic gastrostomy – PEG placement,
has become the preferred method to provide nutritional
support for patients requiring long term (more than
4-6 weeks ) enteral feeding, due to its ease and safety of
placement [2]. The prevalence of PEG tube placement is
increasing [3]. Its estimated prevalence among nursing
home residents with advanced cognitive impairment is
about 18-34% [4, 5, 6]. Complications of PEG placement
may be minor (wound infection, minor bleeding) or
major (necrotizing fasciitis, colocutaneous fistula), but
most of the complications are minor. The reported rates
of complications following PEG placement vary from 16-
70% in different reports [7, 8, 9, 10, 11]. They are more
likely to occur in older adults with comorbid illnesses, particularly those with an infectious process or who
have a history of aspiration [10]. The procedure related
mortality is 0-0.2% [8]. Complications may be early, seen
immediately following PEG tube placement, late seen after
the gastrostomy tract has matured, or complications that
may occur at any time and they include tube dysfunction,
infection, bleeding, peristomal leakage, ulceration, gastric
outlet obstruction and inadvertent gastrostomy tube
removal [7, 8, 9, 10, 11].
CASE REPORT
A Forty-six-year-old female, a resident of a nursing
home who suffers from primary amyloidosis, dementia and
status post cerebrovascular accident with left hemiplegia,
has been nourished through percutaneous gastrostomy
tube in the last several years, which was replaced by
Foley catheter due to accidental dislodgement of the tube
several weeks ago. Her chronic medications are proton
pump inhibitors (PPI), Benzodiazepines & anti epileptics
with no recent use of any other drug. She was admitted to
the internal medicine ward for evaluation of black colored
vomiting and impacted nonfunctional Foley catheter used
as feeding tube without melena or fever. At admission
her vital signs were normal, and abdominal tenderness at
the epigastric region was found with no pathologic bowel
sounds.
Blood tests were as follows - Hct=41.6 (36-54),
Hb=13.7 g/dL (12-16 g/dL), WBCs=8.9 × 103/μL (4-10 ×
103/μL), PLT=215 × 109/L (130-400), BUN=17 mg/dL (7-
18 mg/dL), Creatinine= 0.4 mg/dl (0.5-1.02 mg/dl), K=4
mEq/L (3.5-5.1 mEq/L), Na=141 mEq/L (135-145 mEq/L),
Cl=106 mEq/L (98-107 mEq/L), ALT=199 U/L (0-55 U/L),
AST=178 U/L (5-34 U/L), ALP=185 U/L (40-150 U/L),
GGT=200 U/L (9-36 U/L), Lipase=636 U/L (8-78 U/L),
BILIRUBIN=0.3 mg/dL (0.3-1.2 mg/dL)
In a presumptive diagnosis of acute pancreatitis she
was treated with nil per os (NPO) and intravenous (IV)
normal saline. In the second hospitalization day a contrast
enhanced abdominal computed tomography (CECT) was
done (Figures 1, 2), and revealed dilated gall bladder,
with prominent Wirsung and common bile ducts, a
peripancreatic fluid around the pancreatic tail as a sign
of acute pancreatitis without pancreatic necrosis. There
was no cholelithiasis or choledocholithiasis. A replaced
catheter tip was seen in the descending duodenum with
no evidence of bowel obstruction. The Balthazor grade of
pancreatitis was D and the computed tomography severity
index (CTSI) was 3 points.
Figure 1. CECT with dilated gallbladder with prominent Wirsung and
common bile duct.
Figure 2. CECT with peripancreatic tail fluid.
Fluoroscopy (Figure 3) was done one day later, and
showed contrast in the small bowel with feeding tube tip
in the same region. Id the same day a gastroscopy (Figures
4, 5, 6) was done and it revealed migration of the Foley
catheter passing through the pylorus distally to the second
portion of the duodenum with catheter balloon stuck to the
major papilla and causing a pressure ulcer in the papilla.
Figure 3. Fluoroscopy showing contrast in small bowel.
Figure 4. Gastroscopy showing Stomach with tube migrating through
the pylorus.
Figure 5. Gastroscopy revealing balloon stuck to major papilla
Figure 6. Gastroscopy revealing ulcerated papilla.
The balloon was deflated and the catheter was
removed and replaced by balloon replacement tube
gastrostomy. Biopsies taken from the ulcerated papilla
showed ulcerated small bowel mucosa with acute and
chronic inflammatory cells, granulation tissue and necrotic
inflamed material from ulcer base. Her medical condition
improved dramatically without vomiting or fever and her
vital signs were normal. Hemoglobin was within normal
range, and lipase normalized.
Two days later, enteral feeding and her chronic
medications were resumed with no complications, and
the day after she was discharged with a diagnosis of acute
pancreatitis due to mechanical compression of the papilla
from migrating Foley catheter introduced to feed the
patient instead of inadvertently dislodged tube.
DISCUSSION
PEG placement; has become the modality of choice of
enteral feeding for patients requiring long term enteral
feeding. Its placement is considered easy and safe [2], and
a growing number of nursing home residents and Medicare
patients over the age of 85 years are being fed by PEG [2].
This procedure, though considered safe, can be
complicated with early, late, minor and major complications
and complications that may occur at any time [7, 8, 9, 10, 11].
One complication that may occur at any time is gastrostomy
tube inadvertent removal if traction is placed on tube. This common complication usually occurs in a combative or
confused patient who may pull the tube. If the gastrostomy
tube has time to mature (i.e. at least four weeks old), and a
dedicated replacement tube is not available, a Foley catheter
may be placed through the gastrostomy tract as a temporary
replacement for the gastrostomy tube in order to prevent
tract closure would otherwise begin within 24 hours.
Ulceration related to the gastrostomy tube can occur at any
time and may develop underneath the internal bolster, or on
the contralateral gastric wall from the site of the gastrostomy
tube with balloon gastrostomy replacement tubes [12].
Gastrostomy tubes can migrate forward into the
duodenum at any time after PEG placement, and cause
gastric outlet obstruction [13]. This occurs if the external
bolster on the gastrostomy tube is not attached to the
abdominal wall allowing the gastrostomy tube to slide
forward through the gastrostomy tract into the duodenum.
A similar problem has been reported with balloon
gastrostomy tubes where the inflated balloon is allowed
to migrate through the pylorus resulting in obstruction
[14]. Migration also has been associated with using tubes
without external bumpers, or using Foley catheter G-tubes.
The underlying mechanism of tube migration is thought to be intestinal peristalsis which carries the tube through the
duodenum [15].
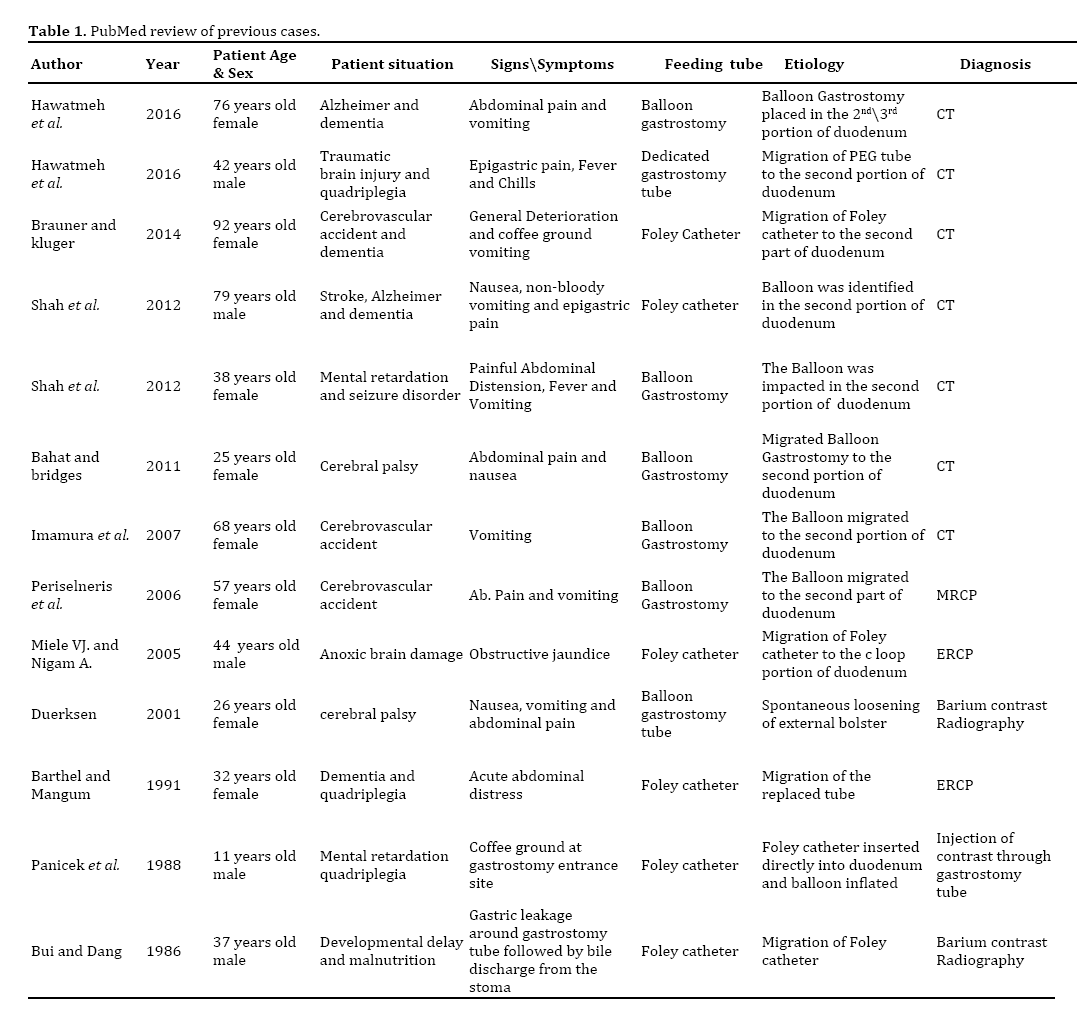
Acute pancreatitis caused by mechanical obstruction
of the major papilla secondary to G-tube migration
seems to be rare and infrequently reported entity in
the English literature. In 1986 Bui and Dang reported
the first case of acute pancreatitis caused by inflated
balloon of a Foley catheter G-tube migrating into the
duodenum [16]. A PubMed search identified 12 cases
since their first report (Table 1) [17, 18, 19, 20, 21, 22, 23, 24, 25, 26].
This rarely reported complication appears to be more
common when a balloon type placement gastrostomy tube
is used, and even more common when a Foley catheter
is used as a replacement tube [24, 25]. The presence of a
water filled balloon on the end of the gastric tube allows
the gastric peristalsis to propel the balloon and forward
the tube. Foley catheters tend more to migrate because
they lack the external bumper which secures the tube to
the abdominal wall, and they lack markings on the catheter
surface that allows measuring the depth of balloon
placement which may lead to inadvertent inflation of the
balloon on the duodenum [24].
The case presented here highlights the recommendation
made by others [24, 25] to prevent this complication by
using Foley catheters only as temporary replacement tube
where dedicated tubes are lacking in order to maintain
the integrity of the tract, and to replace it with a dedicated
tube as soon as possible. In cases where Foley catheters
are used, they should be marked to determine the depth
of insertion prior to inflation and be secured to the
abdominal wall. A radiographic confirmation of the tube
is recommended before initiation of feeding, if there is a
doubt about its location [24].
Expert guidelines recommend avoiding placement of
catheters or tubes not intended for use as enteral feeding
devices, such as urinary or gastrointestinal drainage tubes
which usually are without external anchoring device. Their
use leads to internal misconnection and tube migration
[27]. This rare complication of acute pancreatitis caused
from migrating feeding tube is scarcely reported in the
English literature. To the best of our knowledge, this is
the first case to document endoscopically the mechanical
obstruction of the major papilla by the G-tube balloon
and a papillary ulcer produced by the balloon with biopsy
proven inflammation.
In summary, most of these cases could be prevented by
using dedicated feeding tubes, and in cases where it is not
available, the use of Foley catheter should be temporary
and must be replaced by a dedicated tube as soon as
possible. In any doubt about the location of the tube tip,
a gastrografin film should be done to confirm its location
before initiating feeding. Awareness to this potentially
fatal complication is very important since early diagnosis
and treatment can be crucial.
Competing Interest
The authors declare that they have no competing
interests.
References
- Gauderer MW, Ponsky JL, Izant RJ. Gastrostomy without laparotomy: A percutaneous endoscopic technique. J Pediatr Surg 1980; 15:872-5. [PMID: 6780678]
- Grant MD, Rudberg MA, Brody JA. Gastrostomy placement and mortality among hospitalized Medicare beneficiaries. JAMA 1998; 279:1973-6. [PMID: 9643861]
- Mendiratta P, Tilford JM, Prodhan K, Azhar G, Wei JY. Trends in percutaneous endoscopic gastrostomy placement in the elderly from 1993 to 2003. Am J Alzheimers Dis Other Demen 2012; 27:609-13. [PMID: 23038714]
- Teno JM, Mor V, De Silva D, Kabumoto G, Roy J, Wetle T. Use of feeding tubes in nursing home residents with severe cognitive impairment. JAMA 2002; 287:3211-2. [PMID: 12076216]
- Gessert CE, Mosier MC, Brown EF, Frey B. Tube feeding in nursing home residents with severe and irreversible cognitive impairment. J Am Geriatr Soc 2000; 48:1593-600. [PMID: 11129748]
- Mitchell SL, Teno JM, Roy J, Kabumoto G, Mor V. Clinical and organizational factors associated with feeding tube use among nursing home residents with advanced cognitive impairment. JAMA 2003; 290:73-80. [PMID: 12837714]
- Taylor CA, Larson DE, Ballard DJ, Bergstrom LR, Silverstein MD, Zinsmeister AR, DiMango EP. Predictors of outcome after percutaneous endoscopic gastrostomy: a community-based study. Mayo Clin Proc 1992; 67:1042-9. [PMID: 1434864]
- Larson DE, Burton DD, Schroeder KW, DiMango EP. Percutaneous endoscopic gastrostomy. Indications, success, complications, and mortality in 314 consecutive patients. Gastroenterology 1987; 93:48-52. [PMID: 3108063]
- Blomberg J, Lagergen J, Martin L, Mattsson F, Lagergren P. Complications after percutaneous endoscopic gastrostomy in a prospective study. Scand J Gastroenterol 2012; 47:736-42. [PMID: 22471958]
- Raha SK, Woodhouse K. The use of percutaneous endoscopic gastrostomy (PEG) in 161 consecutive elderly patients. Age Ageing 1994; 23:162-3. [PMID: 8023728]
- Keung EZ, Liu X, Nuzhad A Rabinowits G, Patel V. In-hospital and long-term outcomes after percutaneous endoscopic gastrostomy in patients with malignancy. J Am Coll Surg 2012; 215:777-86. [PMID: 22999329]
- Kazi S, Gunasekaran TS, Berman JH, Kavin H, Kraut JR. Gastric mucosal injuries in children from inflatable low-profile gastrostomy tubes. J Pediatr Gastroenterol Nutr 1997; 25:123. [PMID: 9093991]
- Fischer LS, Bonello JC, Greenberg E. Gastrostomy tube migration and gastric outlet obstruction following percutaneous endoscopic gastrostomy. Gastrointest Endosc 1987; 33:381-2. [PMID: 3315831]
- Chong VH. Gastric outlet obstruction caused by gastrostomy tube balloon. Indian J Gastroenterol 2004; 23:80. [PMID: 15176550]
- Bhargava A, Andrews C, Belforti R. Acute pancreatitis from gastrostomy tube migration in a nursing home resident. Clinical Care and Aging 2011; 19:25-7.
- Bui HD, Dang CV. Acute pancreatitis: a complication of Foley catheter gastrostomy. J Natl Med Assoc 1986; 78:779-81. [PMID: 3093685]
- Panicek DM, Ewing DK, Gottlieb RH, Chew FS. Gastrostomy tube pancreatitis. Pediatr Radiol 1988; 18:416-7. [PMID: 3140201]
- Barthel JS, Mangum D. Recurrent acute pancreatitis in pancreas divisum secondary to minor papilla obstruction from a gastrostomy feeding tube. Gastrointest Endosc 1991; 37:638-40. [PMID: 1756928]
- Duerksen DR. Acute pancreatitis caused by a prolapsing gastrostomy tube. Gastrointest Endosc 2001; 54:792-3. [PMID: 11726866]
- Miele VJ, Nigam A. Obstructive jaundice and pancreatitis secondary to percutaneous endoscopic gastrostomy tube migration. Gastrointest Endosc 2001; 54:792-3. [PMID: 16246209]
- Periselneris J, England R, Hull M. Balloon gastrostomy migration leading to acute pancreatitis. Gut 2006; 55:1673-4. [PMID: 17047124]
- Imamura H, Konagaya T, Hashimoto T, Kasugai K. Acute pancreatitis and cholangitis: a complication caused by a migrated gastrostomy tube. World J Gastroenterol 2007; 13:5285-7. [PMID: 17876903]
- Bhat M, Bridges E. Acute obstructive pancreatitis caused by a migrated balloon gastrostomy tube. CMAJ 2011; 183:E759. [PMID: 21540162]
- Shah AM, Shah N, DePasquale JR. Replacement gastrostomy tube causing acute pancreatitis: case series with review of literature. JOP 2012; 13:54-7. [PMID: 22233947]
- Brauner E, Kluger Y. Gastrostomy tube dislodgment acute pancreatitis. World J Emerg Surg 2014; 9:23-5. [PMID: 24674106]
- Hawatmeh A, Alkhateeb A, Arqoub AA, Jumean K, Shaaban H. Gastrostomy tube migration complicated with acute pancreatitis: Two case reports with review of literature. Int J Crit Illn Inj Sci 2016; 6:48-50. [PMID: 27051623]
- Bankhead R, Boullata J, Brantley S, Corkins M, Guenter P, Krenitsky J, Lyman B, Metheny NA, Mueller C, Robbins S, Wessel J; A.S.P.E.N. Board of Directors. Enteral nutrition practice recommendations. JPEN J Parenter Enteral Nutr 2009; 33:122-67. [PMID: 19171692]







