Keywords
Deoxycytidine; Dihydrouracil Dehydrogenase (NADP); Drug Toxicity; Fluorouracil; Gastrointestinal Hemorrhage; Pancreatic Neoplasms; Radiotherapy; Thymidine Phosphorylase
Abbreviations
CAP: capecitabine; CAPXRT: concurrent capecitabine and irradiation; CT: computed tomography; CTC: common toxicity criteria; CTV: clinical target volume; DVH: dose-volume histogram; 5-FU: 5- fluorouracil; EGD: esophagogastroduodenoscopy; FUdR: 5-fluorodeoxyuridine; GI: gastrointestinal; GTV: gross tumor volume; INR: international normalized ratio; NCI: National Cancer Institute; RTOG: Radiation Therapy Oncology Group; TP: thymidine phosphorylase; UAB: University of Alabama at Birmingham; XRT: external beam radiation therapy
INTRODUCTION
Concurrent fluorouracil (5-FU) and radiotherapy has been the mainstay of treatment for non-metastatic pancreatic cancer in the adjuvant or locally advanced setting [1]. Common gastrointestinal symptoms associated with this treatment include diarrhea, nausea, vomiting, and intestinal fibrosis, sometimes leading to bowel obstruction.
Capecitabine (CAP) is an oral 5-FU pro-drug that is currently being investigated as an alternative treatment for pancreatic cancer [2]. Like 5-FU, it is a well-known radiation sensitizer. The last step in the conversion of CAP to 5-FU occurs through thymidine phosphorylase (TP). This enzyme, which is also known as the platelet-derived endothelial cell growth factor, tends to be found in higher concentrations in tumor tissue than in surrounding normal tissue [3]. This differential creates the potential for tumor selectivity and an enhanced therapeutic index, which has been demonstrated in vivo [4]. Furthermore, clinical studies have documented higher 5-FU concentrations in primary colorectal tumor tissue relative to adjacent normal tissue 5 to 7 days after administration of CAP [5].
Tumor selectivity by CAP leads to speculation that treatment-related toxicity may be diminished by the use of concurrent CAP with external beam radiation therapy (CAP-XRT) when compared to other agents, such as 5-FU. In this study, we report on our clinical experience with this regimen and report on the incidence of late gastrointestinal (GI) bleeding.
PATIENTS AND METHODS
From May 2002 to May 2003, 24 patients began concurrent treatment with CAP-XRT for pancreatic cancer at the University of Alabama at Birmingham (4 resected initially and 20 locally advanced, unresectable). Patients received CAP (600-800 mg/m2 orally twice daily Monday through Friday, total of 1,200-1,600 mg/m2 per day) concurrently with radiation (50.4-54.0 Gy delivered in 28- 30 fractions 5 days per week over 6 weeks) followed by a 4-week rest. Patients then received either 2-4 cycles of capecitabine (surgically resected) or until disease progression occurred (unresected). For both cases, each cycle consisted of capecitabine 1,000-1,250 mg/m2 orally twice daily for 14 days every 3 weeks.
Computed tomography (CT) image-based three dimensional treatment planning was utilized to optimize radiation treatment planning by facilitating identification of the target volume and surrounding normal structures (Figure 1). Attempts were made to minimize radiation dose to surrounding normal tissues while ensuring adequate dose to the target volume. CT simulation was performed with intravenous and oral contrast material to assist in localizing the kidneys, liver, stomach, and intestines. The gross tumor volume (GTV) was defined as the maximum extent of the tumor and involved nodal areas, or tumor bed after surgical resection (marked with clips placed at the time of surgery). The clinical target volume (CTV) was then defined as the GTV plus adjacent loco-regional nodes (celiac, peripancreatic and portal) and para-aortic nodal areas at risk for residual microscopic disease. Anatomical structures were contoured for dose-volume histogram (DVH) analysis. The intestines were defined as the contents within the peritoneal cavity, excluding the stomach, spleen, liver, kidneys, aorta, CTV, and GTV.
Figure 1. Three-dimensional treatment plan with color
wash dose-distributions identifying dose delivered to
tumor volume and surrounding normal anatomical
structures.
Radiation therapy began on the first day of week 1 of CAP therapy. The initial target volume received 1.8 Gy per day delivered Monday through Friday for 25 fractions (45 Gy). After 45 Gy, an additional 3 to 5 fractions of 1.8 Gy were delivered to the GTV or tumor bed with a 1.5 cm margin for a total dose of 50.4 to 54.0 Gy.
Patients were assessed weekly during CAPXRT and every 3 weeks during CAP treatment alone. Acute side effects (within 90 days from the start of XRT) were documented using the National Cancer Institute (NCI) Common Toxicity Criteria (CTC) version 2.0 [https://ctep.info.nih.gov/reporting/CTC-3.html]. Late side effects (after 90 days from the start of XRT) were evaluated and graded according to the Radiation Therapy Oncology Group (RTOG) Late Radiation Morbidity Scoring Scale.
ETHICS
Informed consent was obtained from each patient and the study protocol conformed to the ethical guidelines of the 1975 Declaration of Helsinki as revised in 2000 [6], as reflected in a priori approval by the University of Alabama Institutional Review Board.
STATISTICS
Descriptive statistics have been used: median, range, and frequencies.
RESULTS
The patient population characteristics are listed in Table 1. There were 11 males and 13 females, with a median age of 64.5 years (range 26-80 years). Median follow-up was 10.3 months (range 2.25 to 23.0). There were 22 cases of adenocarcinoma and 2 cases of neuroendocrine carcinoma. Both neuroendocrine patients had functioning tumors and were given somatostatin analogs. Four patients underwent tumor resection prior to irradiation, and 20 patients had locally advanced disease that was initially unresectable. Patients received a median dose of 50.4 Gy. A representative example of radiation fields is shown in Figure 1. Normal anatomical structures were contoured for DVH analysis, and the partial dose-volume histograms for small bowel included in radiation ports are shown in Figure 2. The ‘safe region for complications’ shown in this figure was derived from data estimating the risk of late obstruction, perforation and fistula complications at 5 years after radiation treatment [7]. No patient received small bowel radiation doses in excess of known normal tissue tolerance.

Figure 2. Small bowel partial dose-volume histograms
depicting volumes of small bowel receiving 40, 50, and
60 Gy. Small bowel volumes included all intraperitoneal
contents excluding the kidneys, liver,
stomach, spleen, and gross target volume. The ‘safe
region for complications’ was derived from data
estimating the risk of late obstruction, perforation and
fistula complications at 5 years after radiation
treatment [7].
Three patients developed serious GI bleeding within the radiation port as a late complication. One of these patients recovered, whereas the other 2 patients died as a result of uncontrolled bleeding. Each patient that experienced bleeding had an adenocarcinoma that was initially unresectable due to locally advanced disease. None of the 3 patients who experienced bleeding had a history of prior ulcers or GI bleeding. Review of the patients’ medical records revealed no apparent correlation between the occurrence or severity of acute treatment-related GI side effects and late GI complications. The first patient was a 65-year-old male who presented with obstructive jaundice and a 9 kg weight loss.
He was initially staged as having T4N0M0 disease. The patient’s medical history was notable for atrial fibrillation for which he was taking coumadin. Follow-up CT scan after CAP-XRT revealed a decrease in the size of the pancreatic mass (2.3 cm versus 2.9 cm in maximum dimension prior to treatment), but multiple liver metastases were noted at that time. The patient was therefore started on gemcitabine, but subsequent doses were held because of elevated liver function tests and an upper respiratory infection. He subsequently experienced bright red blood per rectum approximately 1.5 months after completion of CAP-XRT. His platelet count was normal, but his international normalized ratio (INR) was noted to be significantly elevated at 8.00. Esophagogastroduodenoscopy (EGD) revealed 2 antral ulcers and a duodenal ulcer. The patient was stabilized and recovered without further incident.
The second patient was a 63-year-old female who presented with abdominal pain and bloating. She was initially staged as having T3N1M0 disease. She did not have a history of ulcers or gastrointestinal bleeding, but did take famotidine prior to beginning definitive treatment. Follow-up CT scan after CAPXRT revealed the tumor’s size had decreased (4.1 cm to 2.9 cm in maximum dimension). She was therefore continued on xeloda for 5 additional cycles until presenting to the hospital for hematemesis almost 8 months after completing CAP-XRT. Laboratory values drawn at that time showed an INR of 1.30 and a normal platelet count. Both antral and duodenal ulcers as well as an esophageal tear had been seen at an outside hospital, and EGD at UAB revealed an exposed artery in the duodenum. During this procedure, it was also noted that the gastroduodenal artery was encased and severely narrowed by tumor invasion. Angiogram embolization was undertaken and the patient was transfused with 4 units of packed red blood cells. At the request of the family, only supportive care was then given and the patient died 5 days later.
The final patient who experienced GI bleeding was a 67-year-old male who presented with epigastric pain and a 13.6 kg weight loss over a period of 4 months. He was staged as having T4N1M0 disease. The patient’s past medical history was notable for coronary artery disease and a hiatal hernia, for which he took daily aspirin and milk of magnesia, respectively. Serial CT scans after CAP-XRT showed stable disease until the patient developed near total obstruction beginning at the distal stomach approximately 7.5 months after CAP-XRT. Two stents were placed during separate procedures shortly after this time, and a follow-up CT scan revealed marked worsening of the pancreatic disease as well as multiple probable liver metastases. Portal vein thrombosis had developed in addition to worsening biliary and gastric obstruction. The patient then presented with hematemesis 9 months after completion of CAP-XRT. EGD revealed an ulceration around the previously placed stents as well as a large linear ulcer along the greater curvature which was believed to be due to tumor infiltration. The bleeding could not be stopped despite multiple epinephrine injections, and additional aggressive measures were not undertaken at the request of the family. The patient died 12 days after admission to the hospital.
DISCUSSION
5-FU has traditionally been the agent of choice for pancreatic cancer [1]. It is a pyrimidine analogue that has often been used concurrently with radiation due to its known action as a radiation sensitizer [8, 9, 10, 11, 12, 13]. Capecitabine, an orally available prodrug of 5-FU, has generated considerable interest due to its ease of administration as well as other beneficial properties. It is also a radiation sensitizer. Tumor selectivity may be enhanced by preferential bioactivation of CAP to 5-FU in tumors due to increased levels of the activating enzyme thymidine phosphorylase (TP) as compared to normal tissue [3]. Furthermore, radiation may enhance this effect [14]. The possibility of increased selectivity of CAP over other agents has led to the hypothesis that toxicity would be reduced when used concurrently with radiation. This hypothesis, as well as the increased convenience of CAP administration, has led to the investigation of prolonged use of CAP after both definitive and adjuvant chemoradiation.
In our study, CAP was given for 2-4 cycles for patients who underwent surgical resection, and CAP was given indefinitely until disease progression for those with unresectable disease. Our results are similar to other studies of CAP for GI malignancies in that this regimen appeared to be well tolerated and acute toxicity was manageable. However, this regimen yielded an unexpected increased incidence of serious GI bleeding that has not been previously reported. Three out of the 24 patients treated with CAP-XRT followed by CAP therapy had a grade 3 or higher GI bleed. One patient recovered, whereas 2 patients died as a direct consequence of this complication. Each of the 2 fatal cases occurred in the presence of locally advanced disease. One of these patients was taking daily aspirin at the time of the incident. The nonfatal case occurred in a patient who was taking coumadin, and the INR was markedly abnormal at the time of bleeding. Multiple contributing factors were therefore likely responsible for the observed cases of bleeding.
Limited data is available regarding the toxicity of using capecitabine to treat pancreatic cancer. A phase II study of capecitabine alone has been reported that demonstrated a favorable safety profile, with no GI bleeding observed. Patients with advanced or metastatic pancreatic cancer received oral capecitabine 1,250 mg/m2 twice daily (2,500 mg/m2/day) during intermittent 3-week cycles for a duration of treatment based on tumor response. Radiotherapy was not allowed prior to beginning capecitabine or within 4 weeks of treatment start. Patients were monitored for 28 days after the last study treatment [15]. A phase I dose escalation study of bevacizumab with concurrent CAP-XRT was reported for patients with locally advanced, inoperable pancreatic adenocarcinoma. Forty-five patients were studied at varying doses of bevacizumab, a monoclonal antibody against vascular endothelial growth factor. This treatment was continued until disease progression occurred. Patients also received 50.4 Gy to the primary tumor and concurrent capecitabine with doses of either 650 mg/m2 twice daily (6 patients) or 825 mg/m2 twice daily (39 patients). Of the 45 patients studied, 3 patients had tumor-associated duodenal ulceration from 3-20 weeks after completion of XRT, with one case fatal [16]. One additional study evaluated the combination of capecitabine and gemcitabine in patients with advanced pancreatic carcinoma. Gemcitabine, another pyrimidine analogue, is also reported to be a radiation sensitizer and has been used to treat pancreatic cancer. This phase I/II trial utilized a fixed dose of gemcitabine in combination with increasing doses of capecitabine. Dose-limiting toxicies of myelotoxicity and mucositis occurred at 800 mg/m2 orally twice daily. Therefore, 650 mg/m2 twice daily was recommended in combination with gemcitabine at 1,000 mg/m2 on days 1 and 8 of a 21-day cycle. Out of 36 patients, 1 case of bleeding from a duodenal ulcer occurred, corresponding to grade 3 toxicity [17]. Additional data is available regarding the use of concurrent CAP and radiation for other types of GI cancer. One retrospective study reported on CAP-XRT for a variety of GI malignancies [18]. The median dose of CAP was 1,600 mg/m2/day (range: 1,200-2,500 mg/m2/day) orally for 5 days per week during radiation therapy, and 30 patients received a total dose ranging from 45 Gy to 64 Gy over 4-6 weeks. Continued chemotherapy was administered in some patients, with the exact agent chosen based on the specific disease type. However, no patient received continued therapy with CAP following CAP-XRT. No treatment-related mortality was observed in this study despite the higher doses of radiotherapy delivered [18]. Several others have reported on the use of concurrent use of CAP-XRT for rectal cancer [19, 20, 21]. Each of these studies utilized doses of CAP at 1,600 mg/m2/day, given twice daily for 2 weeks followed by 1- week rest. As in the above study, no patient received prolonged CAP therapy following concurrent administration with radiation. No late GI toxicities or treatment-related deaths were reported. Also, a case of CAP-induced radiation recall dermatitis has been reported in a 56-year-old woman treated with 30 Gy for breast cancer metastases to her bone. After therapy, a light skin erythema was detected within the radiation field. This radiationinduced dermatitis had resolved completely 3 weeks after treatment, but reappeared after a 14-day course of CAP was completed [22]. Additionally, we recently reported a case of radiation recall phenomenon in a patient who received CAP after 5-FU-XRT manifesting as GI bleeding [23].
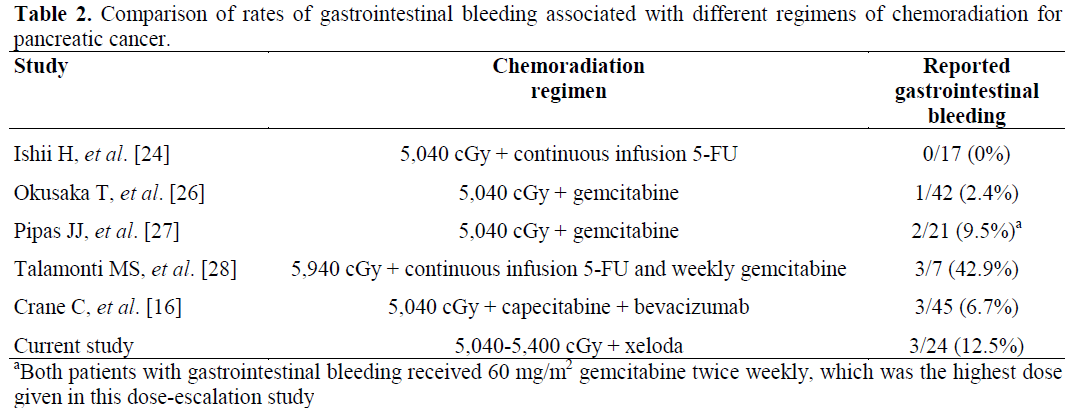
A comparison of our results to the rates of GI bleeding of other chemoradiation regimens for pancreatic cancer is shown in Table 2. 5- FU has been used for decades with little mention of GI bleeding. Common side effects include hematologic toxicity, hand-foot syndrome, and other GI complaints such as nausea, vomiting, and diarrhea. In a study using protracted 5-FU infusion and concurrent radiotherapy for locally advanced pancreatic cancer, none of the 17 patients suffered from GI bleeding [24]. One case report of multisite mucous membrane bleeding was believed to be caused by an interaction of 5-FU and warfarin [25]. It is believed that 5-FU may inhibit the synthesis of cytochrome P-450 2C9, thus causing a greatly increased prothrombin time by impairing the metabolism of warfarin. A phase II study of gemcitabine with concurrent radiotherapy reported 1 incidence of GI bleeding out of the 42 patients treated [26]. This patient’s death was attributed to duodenal bleeding and sepsis. A phase I dose escalation study of gemcitabine and concomitant radiotherapy for 21 patients with adenocarcinoma of the pancreas yielded 2 patients with severe GI bleeding [27]. Each incident occurred approximately 1 month after completion of treatment. One final study of patients with locally advanced pancreatic cancer utilized protracted venous infusion of 5-FU and weekly gemcitabine with concurrent radiotherapy (59.4 Gy). This regimen led to severe early toxicity. Out of 7 patients treated, 3 experienced severe GI bleeding requiring transfusions [28]. It was therefore recommended to avoid this combination regimen in conjunction with radiotherapy.
The mechanism of increased GI bleeding in our study is not clear. The doses of CAP used in this study were somewhat higher than those used in the other CAP-XRT studies cited above [18, 19, 20, 21]. As shown in Figure 2, each of the patients received a dose to the bowel below the normal tissue tolerance for radiation alone. Yet, each of the episodes of GI bleeding occurred within the radiation fields. Additional factors, including local tumor invasion and interactions with other drugs such as coumadin and aspirin likely played a role. However, it does appear that CAP had the effect of lowering the tolerance of the bowel to radiation. As noted above, CAP is believed to be a potent radiation sensitizer, but it was hoped that this effect would preferentially occur in the tumor. Our results suggest that normal tissues may also be adversely affected. It is also possible that an enhanced inflammatory response in the areas immediately adjacent to the tumor sites may have contributed to the observed toxicity. Extensive fibrosis primarily at the tumor site was found in the 5 patients who underwent exploratory laparotomy 6-9 months after completion of CAP-XRT for possible resection of the tumor. Adjacent vascular structures could be compromised as a result of this process.
The prolonged use of CAP beyond CAP-XRT treatment and higher median doses of CAP distinguishes our study from others in which GI bleeding was not a significant problem. Although we cannot define the exact mechanism of the observed GI bleeding, each case was likely multifactorial. Both fatal cases occurred in the context of locally invasive disease, and the nonfatal case involved a patient with a markedly abnormal INR secondary to coumadin. Hematologic toxicity did not appear to play a contributing role. The timeframe of the incidents of GI bleeding is instructive. The two fatal cases occurred 8-9 months after CAP-XRT, with the other case occurring 1.5 months after CAP-XRT. Vigilance in looking for this serious side effect must therefore continue long after the completion of CAP-XRT. This is especially true if the patient is predisposed to bleeding for any reason. Therefore, we recommend that prolonged use of CAP after concurrent CAPXRT be undertaken with caution.
References
- Longley DB, Harkin DP, Johnston PG. 5- fluorouracil: mechanisms of action and clinical strategies. Nat Rev Cancer 2003; 3:330-8. [PMID 12724731]
- Lewis NL, Meropol NJ. Oral fluoropyrimidines in cancer treatment. Cancer Invest 2000; 18:747-60. [PMID 11107445]
- Miwa M, Ura M, Nishida M, Sawada N, Ishikawa T, Mori K, et al. Design of a novel oral fluoropyrimidinecarbamate, capecitabine, which generates 5-fluoruracil selectively in tumours by enzymes concentrated in human liver and cancer tissue. Eur J Cancer 1998; 34:1274-81. [PMID 9849491]
- Ishikawa T, Utoh M, Sawada N, Nishida M, Fukase Y, Sekiguchi F, Ishitsuka H. Tumor selective delivery of 5-fluorouracil by capecitabine, a new oral fluoropyrimidinecarbamate, in human cancer xenografts. BiochemPharmacol 1998; 55:1091-7. [PMID 9605432]
- Schuller J, Cassidy J, Dumont E, Roos B, Durston S, Banken L, et al. Preferential activation of capecitabine in tumor following oral administration to colorectal cancer patients. Cancer ChemotherPharmacol 2000; 45:291-7. [PMID 10755317] 6. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA 2000; 284:3043-5. [PMID 11122593]
- 6. World Medical Association Declaration ofHelsinki: ethical principles for medical researchinvolving human subjects. JAMA 2000; 284:3043-5.[PMID 11122593]
- Emami B, Lyman J, Brown A, Coia L, Goitein M, Munzenrider JE, et al. Tolerance of normal tissue to therapeutic irradiation. Int J RadiatOncolBiolPhys 1991, 21; 109-22. [PMID 2032882]
- Lawrence TS, Davis MA, Tang HY, Maybaum J. Fluorodeoxyuridine-mediated cytotoxicity and radiosensitization require S-phase progression. Int J RadiatOncolBiolPhys 1996; 70:273-80. [PMID 8800198]
- Grem JL. 5-Fluoropyrimidines In: Chabner BA, Longo DL, eds. Cancer Chemotherapy and Biotherapy:Principles and Practice. 2nd Ed. Philadelphia, PA, USA: Lippencott, 1996:149-211.
- Canman CE, Lawrence TS, Shewach DS, Tang HY, Maybaum J. Resistance to fluorodeoxyuridine – induced DNA damage and cytotoxicity correlates with an elevation of deoxyuridinetriphosphatase activity and failure to accumulate deoxyuridine triphosphate. Cancer Res 1993; 53:5219-24. [PMID 8221659]
- Grem JL, Mulcahy RT, Miller EM, Allegra CJ, Fischer PH. Interaction of deoxyuridine with fluorouracil and dipyridamole in human colon cancer cell line. BiochemPharmacol 1989; 38:51-9. [PMID 2462882]
- Houghton JA, Tillman DM, Harwood FG. Ratio of 2’-deozyadenosine-5’-triphosphate/thymidine-5’- triphosphate influences the commitment of human colon carcinoma cells to thymidineless death. Clin Cancer Res 1995; 1:723-30. [PMID 9816038]
- Jones S, Willmore E, Durkacz BW. The effect of 5-fluoropyrimidines on nascent DNA synthesis in Chinese hamster ovary cells monitored by pH-step alkaline and neutral elution. Carcinogenesis 1994; 15:2435. [PMID 7955087]
- Sawada N, Ishikawa T, Sekiguchi F, Tanaka Y, Ishitsuka H. X-ray irradiation induces thymidine phosphorylase and enhances the efficacy of capecitabine (Xeloda) in human cancer xenografts. Clin Cancer Res 1999; 5:2948-53. [PMID 10537364]
- Cartwright TH, Cohn A, Varkey JA, Chen YM, Szatrowski TP, Cox JV, Schulz JJ. Phase II study of oral capecitabine in patients with advanced or metastatic pancreatic cancer. J ClinOncol 2002; 20:160-4. [PMID 11773165]
- Crane CH ,EllisLM, Oreilly M, Ho L, Abbruzzese JL, Evans DB, et al. RhuMab VEGF (bevacizumab) with concurrent radiotherapy and capecitabine in locally advanced pancreatic cancer: An active, well tolerated regimen. Int J RadiatOncolBiolPhys 2004; 60(Suppl 1):S149.
- Hess V, Salzberg M, Borner M, Morant R, Roth AD, Ludwig C, Herrmann R. Combining capecitabine and gemcitabine in patients with advanced pancreatic carcinoma: a phase i/ii trial. J ClinOncol 2003; 21:66- 8. [PMID 12506172]
- Vaishampayan UN, Ben-Josef E, Philip PA, Vaitkevicius VK, Du W, Levin KJ, Shields AF. A single-institution experience with concurrent capecitabine and radiation therapy in gastrointestinal malignancies. Int J RadiatOncolBiolPhys 2002; 53:675-9. [PMID 12062611]
- Reese T, Tanner J, Frings S, Dunst J. Capecitabine combined with simultaneous radiotherapy in rectal cancer: A phase I study (Abstr.). Int J RadiatOncolBiolPhys 2000; 48:120-1.
- Ngan S, Zalcberg J, Kell A, Michael M, MacKay J, Lim Joon, et al. A phase I study of capecitabine combined with radiotherapy locally advanced potentially operable rectal cancer (Abstract). Proc ASCO 2001; 20:591, 104a.
- Yoon WH, Choi JH, Kim JR, Kim T, Lim K, Hwang B, et al. Enhanced tumoricidal effect of preoperative chemoradiation using capecitabine for locally advanced rectal cancer (Abstract). Proc ASCO 2001; 20:2165, 104b.
- Ortmann E, Hohenberg G. Treatment side effects. Case 1. Radiation recall phenomenon after administration of capecitabine. J ClinOncol 2002; 20:3029-30. [PMID 12089233]
- Jeffrey G, Truss C, Saif MW. Radiation recall syndrome associated with capecitabine. The Journal of Applied Research. 2004; 4:495-8.
- Ishii H, Okada S, Tokuuye K, Nose H, Okusaka T, Yoshimori M, et al. Protracted 5-fluorouracil infusion with concurrent radiotherapy as a treatment for locally advanced pancreatic carcinoma. Cancer 1997; 79:1516- 20. [PMID 9118032]
- Brown MC. Multisite mucous membrane bleeding due to a possible interaction between warfarin and 5- fluorouracil. Pharmacotherapy 1997; 17:631-633. [PMID 9165571]
- Okusaka T, Ito Y, Ueno H, Ikeda M, Takezako Y, Morizane C, et al. Phase II study of radiotherapy combined with gemcitabine for locally advanced pancreatic cancer. Br J Cancer 2004; 91:673-7. [PMID 15226765]
- Pipas JM, Mitchell SE, Barth RJ Jr, Vera-Gimon R, Rathmann J, Meyer LP, et al. Phase I study of twice-weekly gemcitabine and concomitant external-beamradiotherapy in patients with adenocarcinoma of thepancreas. Int J RadiatOncolBiolPhys 2001; 50:1317-22. [PMID 11483344]
- Talamonti MS, Catalano PJ, Vaughn DJ,Whittington R, Beauchamp RD, Berlin J, Benson AB3rd. Eastern cooperative oncology group phase i trial ofprotracted venous infusion fluorouracil plus weeklygemcitabine with concurrent radiation therapy inpatients with locally advanced pancreas cancer: aregimen with unexpected early toxicity. J ClinOncol2000; 18:3384-9. [PMID 11013279]



