Keywords
Bronchiolitis Obliterans Organizing Pneumonia; gemcitabine; Pancreatic Neoplasms; Pneumonia
Abbreviations
CONKO: Charité Onkologie; ESPAC: European Study Group for Pancreatic Cancer; RTOG: Radiation Therapy Oncology Group
INTRODUCTION
Pancreatic carcinoma is a lethal disease with an annual incidence rate almost identical to the mortality rate. Cancer of the exocrine pancreas is the fourth most common malignancy in the United States and most newly diagnosed individuals will die within a year [1]. Surgical resection offers the only chance of cure, but only 15 to 20 percent of cases are potentially resectable at presentation. Even in patients who undergo compete (R0) resection, the prognosis is poor; the reported five-year survival rates following pancreaticoduodenectomy for node-negative and node-positive disease are 25% and 10%, respectively [1].
Gemcitabine is the current standard of care in the adjuvant treatment of pancreatic cancer. Based on CONKO-001 and RTOG9704 clinical trials, gemcitabine improves diseasefree survival in pancreatic cancer patients after pancreaticoduodenectomy, and shows a trend towards improvement in survival, with a median overall survival of 20-22 months, and 3-year overall survival of 31-34% [2, 3]. Results from the CONKO-001 trial showed a median disease-free survival of 14.4 months in the gemcitabine group compared to 6.9 months in the control group [2]. An update at the American Society of Clinical Oncology 2008 Annual Meeting updated the results of CONKO-001 reporting an estimated diseasefree survival at 3 and 5 years to be 23.5% and 16% in the gemcitabine group compared to 8.5% and 6.5% in the control group, respectively. Gemcitabine showed significant improvement in the overall survival reported to be 22.8 months versus 20.2 months in the control group. The estimated survival at 3 and 5 years was 36.5% and 21% for gemcitabine patients and. 19.5% and 9% for the control group patients, respectively [4].
In advanced or metastatic pancreatic cancer, although the objective response rate to gemcitabine is minimal, gemcitabine confers a clinical benefit over fluorouracil (5-FU), and is considered the standard of care for these patients. Gemcitabine also leads to a modest improvement in median survival over 5-FU (5.6 vs. 4.4 months) and one-year survival rates (18% vs. 2%) [5]. Unfortunately, combination therapy with other cytotoxic agents has either failed to provide significant benefit or has done so at the expense of intolerable toxicities.
Pulmonary toxicities due to gemcitabine have been reported. Common dyspnea occurs in approximately 25% of patients treated with gemcitabine, whereas serious pulmonary toxicities are much less common, approximately 0.3% [6, 7]. Here we present a case of gemcitabine-induced pneumonitis encountered during adjuvant treatment of pancreatic cancer, and review the literature of this rare, but dangerous complication.
CASE HISTORY
A 68-year-old male with a 75-pack year history of cigarette smoking presented with jaundice and pruritus in November 2007, and was diagnosed with ampullary pancreatic cancer. He underwent a pancreaticoduodenectomy (Whipple procedure) in December 2007, and pathology showed a poorly differentiated adenocarcinoma invading into the muscularis propria and pancreatic parenchyma. He was staged as a pT3N0, Stage IIA pancreatic cancer, with no evidence of metastasis.
His post-operative course was complicated by wound dehiscence. Two months later, he began adjuvant chemotherapy with gemcitabine 1,000 mg/m2 on days 1, 8, and 15 every 28 days based on the CONKO-001 study [2]. After his first dose of gemcitabine, he developed methicillin-resistant Staphylococcus aureus of his wound and was treated with a course of intravenous vancomycin, with resolution
One week after his second dose of gemcitabine, he presented with shortness of breath, and was dyspneic at rest (grade 4 based on NCI Common Terminology Criteria for Adverse Events (CTCAE) version 3.0 criteria (https://ctep.cancer.gov/forms/CTCAEv3.pdf) [8]). He was afebrile. His oxygen saturation was 85% on room air which improved to 92% with 4 L/min of oxygen by face mask. His baseline oxygen saturation had been 95%. On physical exam, patient had diffuse crackles involving both lung fields. He was ruled out for pulmonary embolism with a high resolution computed tomography scan, however, in addition to baseline emphysematous changes, he was noted to have new ground glass opacities bilaterally, predominately in the upper lobes (Figure 1ab). Direct fluorescent antibody testing for viral infections was negative. An echocardiogram was normal. He was treated with a ceftriaxone and doxycycline for community-acquired pneumonia and was discharged on home oxygen.
Figure 1. a. Axial image from a CT angiogram of the chest to
exclude pulmonary embolus. There was no pulmonary
embolus. There is ground glass opacity in both apices
interspersed between changes of emphysema (white
arrows), which was not there previously.
b. Coronal reformatted image from the same CT scan as
in a.. The ground glass opacities are seen in both upper
lobes (white asterisk) and within the right middle lobe
(black asterisk). The lower lobes (black arrows) are
spared. This distribution of ground glass opacity can be
seen with edema, infection, drug reaction, or less likely
hemorrhage.
c. Axial CT three weeks later. The diffuse ground glass
opacities have coalesced into a more focal
consolidation. There were scattered other similar
consolidations in the right upper lobe. This was
interpreted as consistent with cryptogenic organizing
pneumonia (secondary to drug toxicity) versus
infectious pneumonia.
After three more weeks his symptoms still had not completely resolved and he was still requiring oxygen. Pulmonary function testing showed a moderate obstructive process, and a diminished diffusing capacity of 37%, consistent with emphysema. An arterial blood gas revealed mild hypoxemia and showed a normal alveolar-arterial gradient. A repeat CT scan of his chest showed new multiple bilateral patchy airspace opacities, predominantly distributed in the right upper lobe, findings consistent with cryptogenic organizing pneumonia formerly bronchiolitis obliterans organizing pneumonia (Figure 1c). The differential diagnosis consisted of: infection such as viral or bacterial pneumonia, for which he was treated with antibiotics, though he was afebrile, and direct florescent antibody testing was negative; congestive heart failure, though echocardiogram was normal; and gemcitabine-induced pulmonary toxicity. Suspecting gemcitabine-induced pneumonitis, gemcitabine was discontinued and the patient was treated with steroids. A lung biopsy was planned but the patient’s symptoms improved after steroids, and a follow up CT scan showed improvement, so this was not done. Due to concerns of gemcitabine-induced pulmonary toxicity, his chemotherapy was changed to capecitabine monotherapy based on the known activity of fluoropyrimidine monotherapy in pancreatic cancer [9, 10]. The ESPAC-1 trial suggested that adjuvant 5-FU confers a survival advantage over no chemotherapy [10]. The 5- year survival rate was 21% among patients who received chemotherapy and 8% among those who did not receive chemotherapy. In our case, the patient opted for the convenience of oral capecitabine instead of bolus 5-FU. He has had no evidence of disease recurrence 4 months after discontinuing gemcitabine, and his pulmonary issues have completely resolved.
DISCUSSION
Gemcitabine is a fluorine-substituted analog of deoxycytidine which has shown clinical activity in pancreatic, breast, ovarian, nonsmall- cell lung, and bladder cancer. It works by incorporation of its active nucleotide metabolite into DNA resulting in chain termination, and inhibition of DNA synthesis [11]. Gemcitabine further acts as an effective inhibitor of DNA repair which was specifically demonstrated with regard to DNA damage induced by radiation or alkylating agents.
Although gemcitabine is generally well tolerated, myelosuppression is its doselimiting toxicity. Pulmonary toxicities due to gemcitabine have been reported including bronchospasm, capillary leak syndrome, noncardiogenic pulmonary edema, hypersensitivity reaction, acute respiratory distress syndrome, diffuse alveolar damage, pleural effusion and interstitial pneumonitis. In a review of clinical trials with gemcitabine as a single-agent, pulmonary and allergic toxicities were assessed using World Health Organization recommended toxicity grading in 2,704 patients: 7.4% of patients had mild symptoms (grade 1), 7.6% patients experienced dyspnea on exertion (grade 2), dyspnea at rest (grade 3) occurred in 3.1% of treated patients, and complete bed rest (grade 4) was required in 0.8% of patients [6].
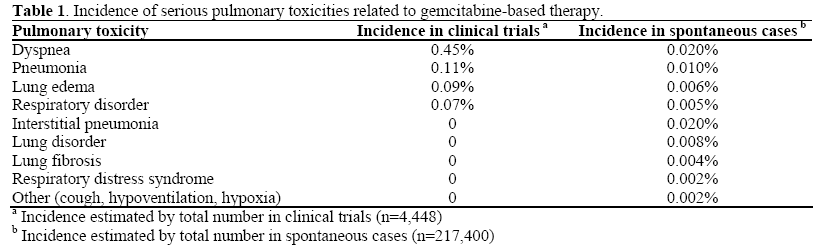
Roychowdhury, et al., reviewed serious pulmonary toxicities that occurred due to gemcitabine within a large clinical trial database [7]. This study reviewed serious pulmonary toxicities such as dyspnea, interstitial pneumonitis, lung disorders, pulmonary edema, lung fibrosis, pneumonia, respiratory disorders, and respiratory distress syndrome, that were likely due to gemcitabine administration. serious pulmonary toxicities were relatively uncommon events (Table 1). Among 4,448 cases within the database, only 0.45% experienced serious dyspnea, and 0.27% experienced serious pulmonary toxicities other than dyspnea. For instance, pulmonary edema was reported in 0.09% of cases, and pneumonia in 0.11%, though none were interstitial pneumonia. Interstitial pneumonia, however, was reported in nonclinical trial spontaneous cases in 0.02% of cases. This indicates that despite large clinical trial databases, some serious toxicities can occur in the post-marketing setting, and may be underreported. In addition, as more patients are treated, the incidence of pulmonary side effects may increase.
When considering risk factors for gemcitabine-induced pulmonary toxicities, one might hypothesize that pre-existing pulmonary disease, prior or concurrent radiation therapy or other anti-neoplastic agents play a role. Many cases of gemcitabine pulmonary toxicity have been in lung and pancreatic cancer; therefore, smoking and prior lung pathology also may be contributing factors. Because of the rarity of serious complications, it is not known whether these comorbidities increase the risk of pulmonary toxicity from gemcitabine. It has been suggested that the risk of gemcitabineinduced pulmonary toxicity increases after repeated dosages [12], however the dosage of gemcitabine does not seem to be playing a role in the development of non-cardiogenic pulmonary edema [13].
Among the case reports published about gemcitabine-induced pneumonitis, three types of pneumonitis have been described: capillary leak syndrome, diffuse alveolar damage, and alveolar hemorrhage. The mortality rate can be as high as 20%. Therefore, it is an important entity to recognize since treatment with corticosteroids has been shown to be effective [14].
The diagnosis of chemotherapy-induced pneumonitis can be made when pneumonitis develops shortly after initiation of treatment, lack of an alternative explanation of respiratory failure, and the resolution of symptoms after corticosteroid treatment and withdrawal of the presumed agent [14]. Gemcitabine-induced pulmonary toxicity is a diagnosis of exclusion after ruling out infectious pneumonia, cardiogenic pulmonary edema and diffuse alveolar hemorrhage. Antibiotics and diuretics are often started empirically. However, once gemcitabine lung toxicity is suspected, discontinuation of the drug, administration of corticosteroids and pulmonary support are the mainstay of treatment and have been successful in treating patients with pulmonary toxicity. Missing the diagnosis can have potentially fatal outcomes. Macroscopically, the findings of gemcitabineinduced pneumonitis include heavy and stiff lungs [15]. Histologically, widespread type 2 pneumocyte hyperplasia with hyaline formation, areas of fibrous thickening of the alveolar wall and patchy alveolar hemorrhage have been described [16].
The pathophysiology of lung injury remains unclear. Several mechanisms have been suggested. Direct injury to pneumocytes, i.e. chemical alveolitis, has been hypothesized. Another proposed mechanism of alveolar damage induced by gemcitabine suggests that it is a cytokine-mediated inflammatory response leading to activation of lymphocytes and alveolar macrophages. The end result is increased vascular permeability with extravasation of fluids and proteins into the air space, resulting in myofibroblast proliferation and collagen deposits [17, 18, 19]. The timing of clinical manifestations is unpredictable; they can present during the first cycle of treatment or following subsequent cycles.
The common radiological findings for gemcitabine induced pneumonitis have been described. On chest X-ray reticulonodular interstitial infiltrates are often present. On computed tomography, one can see diffuse ground glass attenuation involving all lung fields with thickened septal lines, and reticular opacities that are usually bilateral and symmetrical but can be asymmetrical. An open lung biopsy is the only procedure to confirm the diagnosis of drug-induced pneumonitis [16].
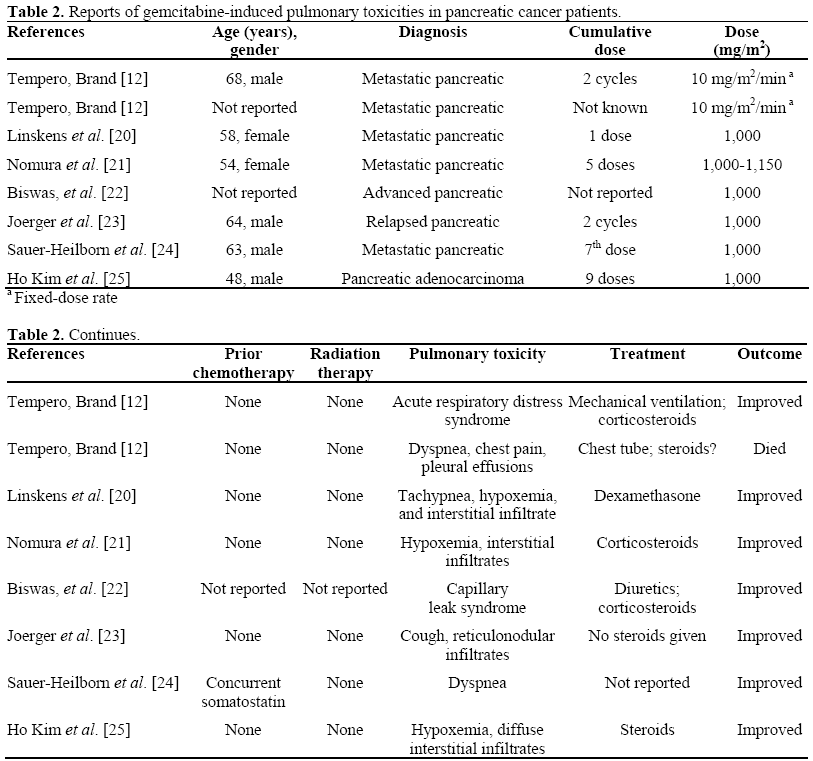
Table 2 summarizes the cases of gemcitabineinduced pulmonary toxicity in patients with pancreatic cancer. Our patient experienced grade 3 dyspnea, and interstitial pneumonia, findings that according to the above studies are relatively rare. What makes this case noteworthy, is that the pulmonary toxicity occurred during adjuvant treatment of pancreas cancer. All of the previously reported cases were in advanced or metastatic pancreatic cancer. This case report highlights the fact that gemcitabine given in the adjuvant setting can cause potentially serious pulmonary toxicities. These pulmonary toxicities are reversible; the signs and symptoms of such toxicity quickly resolve when the drug is stopped, and are successfully treated with steroids.
As the use of gemcitabine has now extended to the adjuvant setting in addition to the palliative setting of pancreatic cancer, oncologists should be aware of the various pulmonary toxicities. Dyspnea occurs in approximately 25% of patients treated with gemcitabine, and serious pulmonary toxicities occur in 0.3% of patients. Oncologists need to be aware of these rare but potentially serious pulmonary side effects. Indeed, what makes diagnosis difficult is that it is often a diagnosis of exclusion. There are some radiographic clues that can help in establishing a diagnosis, and a lung biopsy may be required. A delay in diagnosis and a delay in treatment can lead to potentially fatal outcomes. Severe pulmonary toxicity, such as pneumonitis, or cryptogenic organizing pneumonia, encountered during the adjuvant treatment of pancreatic cancer requires discontinuation of gemcitabine, and prompt initiation of steroids. Upon recovery, discontinuation of gemcitabine may compromise the benefit of adjuvant therapy based on the results of the CONKO-001 study, which showed a modest benefit in disease-free and overall survival. If gemcitabine is discontinued due to untoward side effects, we recommend a change to a fluoropyrimidine such as 5-FU or capecitabine to complete adjuvant therapy.
Conflict of interest
The authors have no potential conflicts of interest
References
- Steer M. Clinical manifestations, diagnosis, and surgical staging of exocrine pancreatic cancer. UpToDate. 2008; version 16.2.
- Oettle H, Post S, Neuhaus P, Gellert K, Langrehr J, Ridwelski K, et al. Adjuvant chemotherapy with gemcitabine vs observation in patients undergoing curative-intent resection of pancreatic cancer: a randomized controlled trial. JAMA 2007; 297:267-77. [PMID 17227978]
- Regine WF, Winter KA, Abrams RA, Safran H, Hoffman JP, Konski A, et al. Fluorouracil vs gemcitabine chemotherapy before and after fluorouracil-based chemoradiation following resection of pancreatic adenocarcinoma: a randomized controlled trial. JAMA 2008; 299:1019-26. [PMID 18319412]
- Neuhaus P, Riess H, Post S, Gellert K, Ridwelski K, Schramm H, et al. CONKO-001: Final results of the randomized, prospective, multicenter phase III trial of adjuvant chemotherapy with gemcitabine versus observation with resected pancreatic cancer. J Clin Oncol 2008; 26(20 Supplement):LBA4504.ASCO Annual Meeting Proceedings.
- Burris HA 3rd, Moore MJ, Andersen J, Green MR, Rothenberg ML, Modiano MR, et al. Improvements in survival and clinical benefit with gemcitabine as firstline therapy for patients with advanced pancreas cancer: a randomized trial. J Clin Oncol 1997; 15:2403-13. [PMID 9196156]
- Prescribing information, Gemzar (Gemcitabine HCL), for Injection, 1998.
- Roychowdhury DF, Cassidy CA, Peterson P, Arning M. A report on serious pulmonary toxicity associated with gemcitabine-based therapy. Invest New Drugs 2002; 20:311-5. [PMID 12201493]
- National Cancer Institute, U.S. National Institute of Health. Common Terminology Criteria for Adverse Events v3.0 (CTCAE). https://ctep.cancergov/reporting/ ctc_v30.html (Publish date August 9, 2006).
- Boeck S, Wilkowski R, Bruns CJ, Issels RD, Schulz C, Moosmann N, et al. Oral capecitabine in gemcitabine-pretreated patients with advanced pancreatic cancer. Oncology 2007; 73:221-7. [PMID 18424886]
- Neoptolemos JP, Stocken DD, Friess H, Bassi C, Dunn JA, Hickey H, et al. A randomized trial of chemoradiotherapy and chemotherapy after resection of pancreatic cancer. N Engl J Med 2004; 350:1200-10. [PMID 15028824]
- Chu E, DeVita VT. Physicians' Cancer Chemotherapy Drug Manual 2008. E. Chu, VT DeVita Jr (eds). Jones and Bartlett Publishers.
- Tempero MA, Brand R. Fatal pulmonary toxicity resulting from treatment with gemcitabine. Cancer 1998; 82:1800-1. [PMID 9576306]
- Vermorken JB, Guastalla JP, Hatty SR, Seitz DE, Tanis B, McDaniels C, Clavel MD. Phase I study of gemcitabine using a once every 2 weeks schedule. Br J Cancer 1997; 76:1489-93. [PMID 9400947]
- Vahid B, Marik PE. Pulmonary complications of novel antineoplastic agents for solid tumors. Chest 2008; 133:528-38. [PMID 18252919]
- Marruchella A, Fiorenzano G, Merizzi A, Rossi G, Chiodera PL. Diffuse alveolar damage in a patient treated with gemcitabine. EurRespir J 1998; 11:504-6. [PMID 9551762]
- Barlesi F, Villani P, Doddoli C, Gimenez C, Kleisbauer JP. Gemcitabine-induced severe pulmonary toxicity. FundamClinPharmacol 2004; 18:85-91. [PMID 14748759]
- Briasoulis E, Pavlidis N. Noncardiogenic pulmonary edema: an unusual and serious complication of anticancer therapy. Oncologist 2001; 6:153-61. [PMID 11306727]
- Ciotti R, Belotti G, Facchi E, Cantu A, D'Amico A, Gatti C. Sudden cardio-pulmonary toxicity following a single infusion of gemcitabine. Ann Oncol 1999; 10:997. [PMID 10509166]
- Pavlakis N, Bell DR, Millward MJ, Levi JA. Fatal pulmonary toxicity resulting from treatment with gemcitabine. Cancer 1997; 80:286-91. [PMID 9217042]
- Linskens RK, Golding RP, van Groeningen CJ, Giaccone G. Severe acute lung injury induced by gemcitabine. Neth J Med 2000; 56:232-5. [PMID 10821980]
- Nomura M, Inoue Y, Fujita S, Sakao J, Hirota M, Souda S. A case of drug-induced interstitial pneumonitis after gemcitabine treatment for advanced pancreatic cancer. GanTo Kagaku Ryoho 2006; 33:123-7. [PMID 16410712]
- Biswas S, Nik S, Corrie PG. Severe gemcitabineinduced capillary-leak syndrome mimicking cardiac failure in a patient with advanced pancreatic cancer and high-risk cardiovascular disease. Clin Oncol (R CollRadiol) 2004; 16:577-9. [PMID 15630853]
- Joerger M, Gunz A, Speich R, Pestalozzi BC. Gemcitabine-related pulmonary toxicity. Swiss Med Wkly 2002; 132:17-20. [PMID 11901447]
- Sauer-Heilborn A, Kath R, Schneider CP, Höffken K. Severe non-haematological toxicity after treatment with gemcitabine. J Cancer Res Clin Oncol 1999; 125:637-40. [PMID 10541971]
- Ho Kim D, Shiozawa S, Tsuchiya A, Usui T, Inose S, Aizawa M, et al. A case of drug-induced interstitial pneumonitis after adjuvant chemotherapy with gemcitabine for pancreatic cancer. GanTo Kagaku Ryoho 2008; 35:133-6. [PMID 18195543]


