Keywords
Adenoma; Adenomatous Polyps; Brunner Glands; Duodenal Obstruction; Intussusception; Pancreatic Neoplasms; Pancreaticoduodenectomy
INTRODUCTION
Benign tumors of the duodenum are rare. Brunner’s gland adenoma, also known as brunneroma or Brunner’s gland hamartoma constitutes only 10.6% of these tumors [1]. In the literature, only 150 cases of Brunner’s gland adenoma have been reported to date [2]. Most of these adenomas are small and asymptomatic, and are found incidentally during endoscopy. The large or giant variety is uncommon and may present with problems related to their size or location. When symptomatic, they usually present with intestinal obstruction or gastrointestinal bleeding [3]. In rare cases, these giant adenomas may simulate pancreatic or duodenal malignancy, leading to a diagnostic and therapeutic challenge regarding their management [4].
We herein describe a case of giant Brunner’s gland adenoma arising from the duodenal bulb which presented as a malignancy of the uncinate process of the pancreas along with duodenal and ampullary obstruction.
CASE REPORT
A 65-year-old female presented with a two-month history of upper abdominal pain, early satiety, nausea, retrosternal burning pain and 3 kg weight loss. There was no history of vomiting, melena, jaundice, anemia or anorexia. Physical and abdominal examinations were unremarkable. Blood investigation revealed elevated serum alkaline phosphatase (418 IU/dL; reference range: 0-270 IU/dL) and gamma-glutamyl transpeptidase (GGT, 209 IU/dL; reference range 0-50 IU/dL) with normal serum bilirubin, serum glutamic oxaloacetic transaminase (SGOT) and serum glutamic pyruvic transaminase (SGPT). Other blood parameters, including hemoglobin and tumor markers, such as carcinoembryonic antigen (CEA) and carbohydrate antigen 19-9, were within the normal limits.
Abdominal ultrasonography showed a distended gallbladder without any calculi, prominent intrahepatic biliary radicals, dilated (10 mm) common bile duct till its lower end with no calculi, prominent main pancreatic duct and a 2.8x1.9 cm hypoechoic mass near the distal end of the common bile duct. An abdominal computed tomography (CT) scan confirmed the dilatation of the common bile duct and the main pancreatic duct, and revealed an ill-defined hypodense mass 6.5x5.5 cm in size arising from the uncinate process of the pancreas (Figure 1). The mass involved the duodenum with an extension to the duodenojejunal flexure. The proximal duodenum was found to be dilated. The CT scan suggested the diagnosis of a pancreatic mass with duodenal infiltration. Upper gastrointestinal endoscopy was performed showing esophagitis and extraneous compression in the duodenal bulb. A side-viewing endoscopy was performed and showed a long pedicle-like structure extending from the duodenal bulb into the distal duodenum along the medial wall of the second part of the duodenum (Figure 2). The distal end of this structure, the ampulla and the distal duodenal lumen could not be visualized. An attempt was made to pull the distal end of the structure using biopsy forceps but without success. Besides these findings, no ulcer, stricture or growth was found in the duodenum. In view of the endoscopic findings, the CT scan was reviewed carefully. The mass initially described as originating from the uncinate process was suspected to be intraluminal within the distal duodenum with a smooth outline at the distal end. However, this mass could not be defined as separate from the pancreas. In addition, a characteristic sign of “duodenal wall invagination” was observed in the dilated first part of the duodenum (Figure 3). Barium meal examination of the upper digestive tract showed a well defined smooth lobular filling defect in the dilated first part of the duodenum (Figure 4). Given the above findings, a duodenal polypoid mass of unknown nature was suspected. A side-viewing endoscopy was repeated and endoscopic ultrasonography (EUS) was also performed. During this examination, a large polypoid mass with normal overlying mucosa was seen in the proximal duodenum (Figure 5a). The ampulla was seen as separate from the polyp and was found to be normal as was the visualized distal duodenum (Figure 5b). Endoscopic ultrasonography revealed a homogenous echogenic mass occupying the submucosa in the duodenal bulb with a normal pancreas which was not involved by the mass (Figure 5c). A biopsy taken from the polyp showed non-specific changes in the mucosa. At laparotomy, the duodenum was found to be dilated as far as the third part with a polypoid mass palpated in the proximal duodenum. A duodenotomy at the junction of the first and second parts of the duodenum revealed a large, firm, pedunculated polyp with normal overlying mucosa arising from the posterosuperior aspect of the duodenal bulb (Figure 6a). The pancreas and the duodenum were found to be normal. A transduodenal polypectomy was performed. On gross examination, a 6x5x3 cm large, firm, polypoidal mass with multiple tiny dimple-like depressions in the overlying mucosa oozing thick mucoid secretion and having a solid lobulated pattern on cut section was observed (Figure 6b). Histopathological examination revealed the presence of hyperplastic Brunner’s glands arranged in a lobulated pattern with intervening fibrous septa, suggesting a diagnosis of Brunner’s gland adenoma. There was no evidence of malignancy in this adenoma. The postoperative period was uneventful and she is well after a two year follow-up with normalization of the liver enzymes and resolution of the dilated biliary and pancreatic ductal systems on ultrasonography.
Figure 1. CT scan showing hypodense mass involving the distal
duodenum and the uncinate process of the pancreas, and extending to
the duodenojejunal flexure (arrow), causing dilatation of the
proximal duodenum.
Figure 2. Side-viewing endoscopy. a. Long pedicle-like structure
(arrow) extending from the first part of the duodenum (D1) to its
third part (D3) with non-visualization of the ampulla.
b. Hemorrhagic areas are seen on the distal aspect of the pedicle
resulting from a failed attempt to pull the distal end of the pedicle.
S: scope
Figure 3. CT scan showing the dilated first part of the duodenum (D)
along with the thickening and characteristic invagination of the
anterior duodenal wall (arrows: invagination sign).
Figure 4. Barium study showing a well-defined lobular filling defect
with smooth outline (arrows) in the first part of the duodenum.
Figure 5. Repeat side-viewing endoscopy along with EUS. a. Large polyp (P) in its original position within the proximal duodenum with a wide
pedicle and normal overlying mucosa. b. The ampulla was normal and bile was seen coming through it. c. EUS showing well-defined echogenic
mass confined to the submucosa (arrows) in the first part of the duodenum with no invasion beyond this layer.
Figure 6. a. Intraoperative photograph showing a large polyp (P) arising from the first part of the duodenum as seen after its removal by means of a
duodenotomy (arrow). b. Resected specimen showing lobulated architecture on cut section.
DISCUSSION
Brunner’s gland adenoma arises from Brunner’s glands which are located in the deep mucosa and submucosa of the duodenum. As these glands are found predominantly in the proximal duodenum, Brunner’s gland adenomas usually (57-70%) develop in the duodenal bulb [3, 5]. They most commonly occur in the fifth and sixth decades of life with no sex predominance. Development of these lesions may be related to chronic renal failure [6], chronic pancreatitis [7], peptic ulcer disease [8] or Helicobacter pylori infection [9].
They are usually asymptomatic and are discovered incidentally during endoscopy. Symptomatic cases most commonly present with gastrointestinal bleeding and obstruction [3]. Bleeding is often chronic and may be manifested as chronic anemia. Obstructive symptoms usually occur when they are larger than 2 cm [10]. Brunner’s gland adenoma may present with gastric outlet obstruction [11], duodenal obstruction, as in our case, or occasionally with the intussusception of the duodenal wall [12, 13, 14, 15]. The present case had chronic intermittent duodenal obstruction at the duodenojejunal flexure due to the intermittent prolapse of the polyp. This was evidenced by the presence of a dilated duodenum and the symptoms of gastroesophageal reflux. This obstruction was related to the large size of the polyp and, probably, also to duodenal intussusception. Our patient was having recurrent episodes of duodenal intussusception which were present at the time of the initial endoscopy as well as during the CT scan, as evidenced by the invagination of the duodenal wall (Figure 3). However, it was in the early stage and had already been reduced at the time of surgery.
Rare presentations of Brunner’s gland adenoma include acute pancreatitis [16], biliary fistula [17] and biliary obstruction. Only 4 cases of biliary obstruction have been reported to date [4, 18]. In another case of Brunner’s gland adenoma with obstructive jaundice reported by Hol et al. [2], associated jaundice was secondary to ampullary obstruction caused by a synchronous ampullary carcinoma rather than by Brunner’s gland adenoma. In our case, the Brunner’s gland adenoma originated from the duodenal bulb. Its intermittent prolapse into the distal duodenum led to intermittent obstruction of the ampulla by the stretched out pedicle passing along the medial wall of the second part of the duodenum. Upstream dilatation of both the biliary and the pancreatic ductal systems led to the assumption of periampullary malignancy on initial evaluation.
Brunner’s gland adenoma is the rarest of three types of Brunner’s gland hyperplasia or hamartoma [19]. The other two types are circumscribed nodular hyperplasia and diffuse nodular hyperplasia. Brunner’s gland adenoma is a benign lesion with a favorable long term outcome. Malignant changes are very rare with only 7 cases reported in the literature [2]. Brunner’s gland adenomas are usually small in size. Although large adenomas are uncommon, they are clinically more important as they are more likely to be symptomatic. Specifically, the giant variety is diagnostically challenging due to their large size. Most importantly, these lesions may mimic pancreaticoduodenal malignancy on imaging, or even intraoperatively, leading to difficulty in management [4, 20, 21, 22, 23] (Table 1).
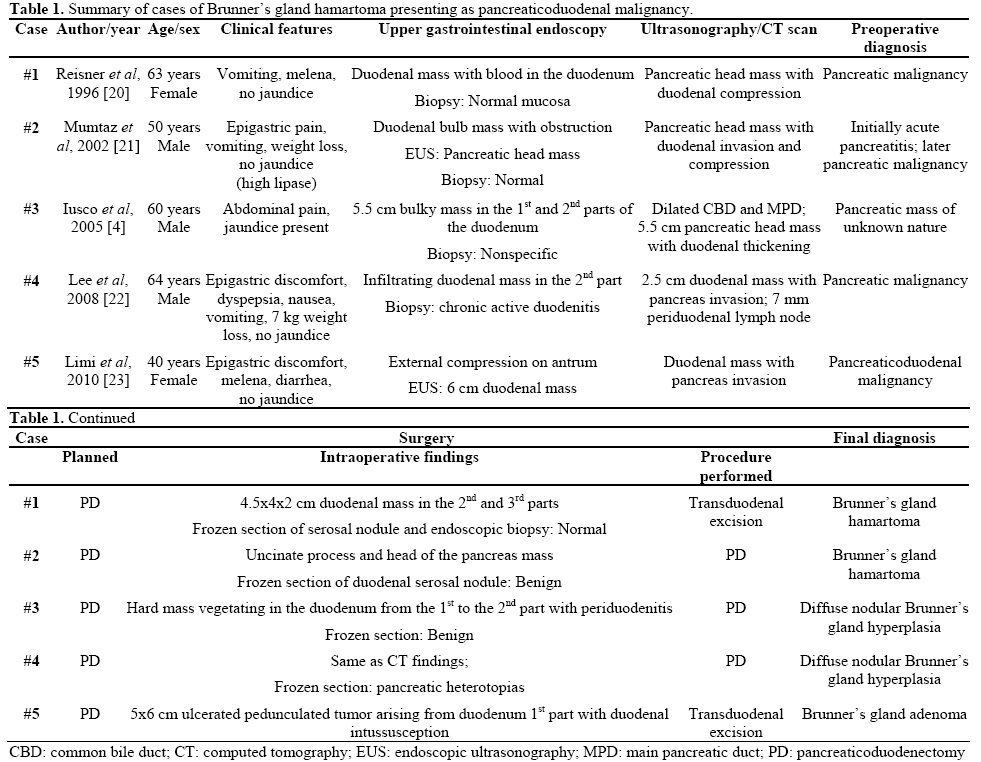
In all the cases reported, pancreatic malignancy with duodenal infiltration or vice versa was suspected preoperatively. In four cases, even endoscopic biopsy and intraoperative frozen section analysis of the suspected neoplastic tissue failed to identify the true nature of the lesion. In three cases, a correct diagnosis of Brunner’s gland hyperplasia could be established only after a pancreaticoduodenectomy while in the remaining two cases transduodenal excision of the duodenal mass was performed instead of the pancreaticoduodenectomy which was originally planned. In two instances [4, 22], the pancreaticoduodenal mass was found to be diffuse nodular variant of Brunner’s gland hyperplasia on histopathology. This variety may be more difficult to differentiate from pancreaticoduodenal malignancy than the adenomatous hyperplastic type which usually presents as a welldefined polyp.
Mumtaz et al. [21] reported a case in which acute pancreatitis was initially suspected due to high serum lipase levels. Upper gastrointestinal endoscopy combined with EUS, performed because of the features of gastric outlet obstruction, showed a pancreatic head mass. Although intraoperative assessment suggested a pancreatic mass, a 6.6x4.5 cm fungating, circumferential mass was found in the area of main duodenal papilla with a normal pancreas on examination of the resected specimen. This mass was found to be a Brunner’s gland hamartoma on histopathology.
Skellenger et al. [24] also had a similar diagnostic dilemma with three patients and suggested an intraoperative biopsy to confirm the diagnosis. All these case studies suggest that Brunner’s gland hamartoma can be very difficult to identify and differentiate from a malignant neoplasm of the pancreas and the duodenum on preoperative or even intraoperative assessment, and may lead to “overtreatment”.
Preoperative endoscopy and biopsy may help in making a correct diagnosis but with limitations (72- 89% sensitivity) [4] as these lesions are submucosal and may be missed by a mucosal pinch biopsy. Endoscopic ultrasound may also be helpful. On EUS, Brunner’s gland hamartoma is characterized by a heterogeneous solid and/or cystic or multicystic mass [25], or a homogenous echogenic mass located in the submucosa [26]. On barium examination of the upper digestive tract, these lesions produce a characteristic “cobblestone” appearance or a well defined filling defect [26]. Although intraoperative biopsy has a sensitivity of 83-92% [4], serious complications (e.g. pancreatitis, pancreatic fistula or bleeding) may occur in addition to the possibility of sampling error. However, major surgery, such as a pancreaticoduodenectomy, may be resorted to if there remains a strong suspicion of malignancy, even after an extensive work-up, provided such surgery is performed at a specialized center with low morbidity and mortality rates [4]. In our case, we were able to correctly rule out the pancreaticoduodenal malignancy by performing more extensive evaluation with a barium study, repeat endoscopy and endoscopic sonography.
Management of these lesions includes a conservative approach in asymptomatic patients. Only symptomatic cases require treatment. Conservative treatment, in the form of controlling of gastric acidity, rarely leads to regression of these lesions [4]. Therefore, endoscopic [27, 28] or surgical removal is the treatment of choice. Endoscopic removal is feasible in most of the cases as Brunner’s gland adenomas are usually small. However, large adenomas have also been successfully removed endoscopically [29]. Larger lesions, especially diffuse nodular hyperplasia, need surgical excision; options include laparoscopic [30] or open polypectomy, segmental resection, pancreas sparing duodenectomy [31] and, occasionally, pancreaticoduodenectomy with an excellent long term outcome.
To conclude, Brunner’s gland adenoma of the duodenum may present as pancreaticoduodenal malignancy especially when it is large. It may even cause jaundice due to ampullary obstruction and duodenal obstruction as may occur in pancreatic malignancy. Preoperative differentiation on CT scan may be difficult, and diligent evaluation with combined endoscopy and endoscopic sonography aided by barium examination may be helpful in reaching a correct diagnosis. If required, these investigations should be repeated to exclude the malignant process, the treatment and outcome of which is totally different from benign disease, such as Brunner’s gland adenoma.
Financial Support
Nil
Conflicts of interest
The authors have no potential conflicts of interest
References
- Osborne R, Toffler R, Lowman RM. Brunner's gland adenoma of the duodenum. Am J Dig Dis 1973; 18:689-94. [PMID 4721129]
- Hol JW, Stuifbergen WN, Teepen JL, van Laarhoven CJ. Giant Brunner's hamartomas of the duodenum and obstructive jaundice. An overview of the literature and suspicion of malignancy in a case. Dig Surg 2007; 24:452-5. [PMID 18025786]
- Levine JA, Burgart LJ, Batts KP, Wang KK. Brunner's gland hamartomas: clinical presentation and pathological features of 27 cases. Am J Gastroenterol 1995; 90:290-4. [PMID 7847303]
- Iusco D, Roncoroni L, Violi V, Donadei E, Sarli L. Brunner's gland hamartoma: 'over-treatment' of a voluminous mass simulating a malignancy of the pancreatic-duodenal area. JOP. J Pancreas (Online) 2005; 6:348-53. [PMID 16006686]
- Silverman L, Waugh JM, Huizenga KA, Harrison EG Jr. Large adenomatous polyp of Brunner's glands. Am J Clin Pathol 1961; 36:438-43. [PMID 13912933]
- Paimela H, Härkönen M, Karonen SL, Tallgren LG, Stenman S, Ahonen J. Relation between serum group II pepsinogen concentration and the degree of Brunner's gland hyperplasia in patients with chronic renal failure. Gut 1985; 26:198-202. [PMID 3967837]
- Sáenz de Santa María J, Pajuelo F, Lozano F, Cordero R, Pérez Miranda M. Diffuse hyperplasia of Brunner's glands in relation to pancreatic and/or renal disease. Med Clin (Barc) 1983; 80:646. [PMID 6876924]
- Fuse Y, Tsuchihashi Y, Takamasu M, Kawamoto K, Kodama T, Fujita S, Kashima K. Thickness of Brunner's glands and its clinical significance in peptic ulcer diseases. Gastroenterol Jpn 1989; 24:512- 8. [PMID 2806830]
- Kovacevic I, Ljubicic N, Cupic H, Doko M, Zovak M, Troskot B, et al. Helicobacter pylori infection in patients with Brunner's gland adenoma. Acta Med Croatica 2001; 55:157-60. [PMID 12398018]
- deNes LC, Ouwehand F, Peters SH, Boom MJ. A large Brunner's gland hamartoma causing gastrointestinal bleeding and obstruction. Dig Surg 2007; 24:450-2. [PMID 18025785]
- Lingawi SS, Filipenko JD. Brunner's gland hamartoma causing gastric outlet obstructive symptoms. South Med J 1998; 91:964-5. [PMID 9786295]
- Lempke RE. Intussusception of the duodenum: report of a case due to Brunner's gland hyperplasia. Ann Surg 1959; 150:160-6. [PMID 13661844]
- Kellogg EL. Intussusception of the duodenum caused by adenoma originating in Brunner's glands. Med J Record 1931; 134:440-2.
- Chuang JH, Chen WJ. Duodenojejunal intussusception secondary to hamartomatous polyp of Brunner's glands. J Pediatr Gastroenterol Nutr 1991; 13:96-100. [PMID 1919957]
- Peetz ME, Moseley HS. Brunner's gland hyperplasia. Am Surg 1989; 55:474-7. [PMID 2662841]
- Stermer E, Elias N, Keren D, Rainis T, Goldstein O, Lavy A. Acute pancreatitis and upper gastrointestinal bleeding as presenting symptoms of duodenal Brunner's gland hamartoma. Can J Gastroenterol 2006; 20:541-2. [PMID 16955152]
- Hedges AR. Hamartoma of Brunner's gland causing pyloric obstruction and a biliary fistula. Case report. Acta Chir Scand 1988; 154:475-6. [PMID 3263743]
- Shorrock K, Haldane JS, Kersham MJ, Leach RD. Obstructive jaundice secondary to carcinoma arising in Brunner's glands. J R Soc Med 1986; 79:173-4. [PMID 3701756]
- Feyter F. OuberWucherun gender BrunnerschenDrusen. Virchow Arch Path Anat 1934; 293:509.
- Reisner RM, Nava HR. Large Brunner's gland hamartoma simulating a pancreatic mass with obstruction and bleeding. Surg Endosc 1996; 10:341-3. [PMID 8779074]
- Mumtaz R, Shah IA, Ramirez FC. Brunner's gland hamartoma simulating a pancreatic mass with duodenal obstruction. Gastrointest Endosc 2002; 56:932-4. [PMID 12447318]
- Lee WC, Yang HW, Lee YJ, Jung SH, Choi GY, Go H, et al. Brunner's gland hyperplasia: treatment of severe diffuse nodular hyperplasia mimicking a malignancy on pancreatic-duodenal area. J Korean Med Sci 2008; 23:540-3. [PMID 18583897 23.]
- Limi L, Liew NC, Badrul RH, Faisal MJ, Daniel YPK. Duodenal intussusception of Brunner's gland adenoma mimicking a pancreatic tumor. Med J Malaysia 2010; 65:313-4.
- Skellenger ME, Kinner BM, Jordan PH Jr. Brunner's gland hamartomas can mimic carcinoma of the head of the pancreas. Surg Gynecol Obstet 1983; 156:774-6. [PMID 6857456]
- Hizawa K, Iwai K, Esaki M, Suekane H, Inuzuka S, Matsumoto T, et al. Endosonographic features of Brunner's gland hamartomas which were subsequently resected endoscopically. Endoscopy 2002; 34:956-8. [PMID 12471538]
- Patel ND, Levy AD, Mehrotra AK, Sobin LH. Brunner's gland hyperplasia and hamartoma: imaging features with clinicopathologic correlation. AJR Am J Roentgenol 2006; 187:715-22. [PMID 16928936]
- Rajagopalan S, al-Arrayed S, Dhiman RK. Brunner's gland polyp with upper gastrointestinal bleeding managed by endoscopic polypectomy: a report of two cases. Trop Gastroenterol 2003; 24:133-4. [PMID 14978987]
- Chen YY, Su WW, Soon MS, Yen HH. Hemoclip-assisted polypectomy of large duodenal Brunner's gland hamartoma. Dig Dis Sci 2006; 51:1670-2. [PMID 16927147]
- Rocco A, Borriello P, Compare D, De Colibus P, Pica L, Iacono A, Nardone G. Large Brunner's gland adenoma: case report and literature review. World J Gastroenterol 2006; 12:1966-8. [PMID 16610009]
- Baladas HG, Borody TJ, Smith GS, Dempsey MB, Richardson MA, Falk GL. Laparoscopic excision of a Brunner's gland hamartoma of the duodenum. Surg Endosc 2002; 16:1636. [PMID 12196895]
- Gupta V, Singh V, Kalra N, Vaiphei K. Pancreas sparing resection for giant hamartoma of Brunner's glands. JOP. J Pancreas (Online) 2009; 10:196-9. [PMID 19287118]







