Kankana De*
Vidyasagar University, Medinipur, West Bengal, India
*Corresponding Author:
Kankana De
Vidyasagar University, Medinipur
West Bengal, India
Tel: 9474714273
E-mail: dekankana@gmail.com
Received date: March 21, 2017; Accepted date: April 25, 2017; Published date: April 27, 2017
Citation: Kankana De. Growth Pattern and Relation with Age at Menarche. Ped Health Res 2017, 2:1. doi: 10.2176/2574-2817.100012
Back ground: Body composition assessment helps to growth pattern in adolescent, for body composition measurement research measures weight, height, different kind of circumferences. Chronic Energy Deficiency (CED) has been defined as a state of ‘steady’ or body energy stores. A BMI < 18.5 kg/m2 is widely used as a practical measure underweight.
Methodology: This study is carried out in outpatient of sub-centre of a rural hospital of Medinipur district; some girls are school dropout and some are regular school goers, Study group girls are 10-19 years old,100 girls in each group, Anthropometry are used to take measurement of height (Anthropometry rod) weight (weighing machine), harpendent to take skinfold measurement.
Results: Table 1 represents that mean height, weight, MUAC of study group is 151.02 cm (4.81), 44.56 (5.07), weight (kg) MUAC21.71 cm (2.85). Table 2 represent comparison of anthropometric value of pre-menarcheal and menarcheal girls. The Figures 1-3 represent age wise pre-menarcheal, post-menarcheal, combined status of adolescent girls, whereas the Table 3 represent age wise standard deviation and mean of height, weight and BMI. Results revealed that boys were significantly heavier than girls from age 16 onwards.
Conclusion: Girls have poor knowledge on hygiene, they take bath in pond, which causes reproductive health related issues, like white discharge; they have poor concept on menstrual hygiene. To overcome all this they need counselling on their health, nutrition hygiene, how to cure reproductive tract infection.
Keywords
Body mass index; Nutritional status; Diet; Hygiene
Introduction
The word ‘anthropometry’ was first used in the seventeenth century by a German physician, Sigismund Elsholtz in his graduation thesis entitled “Anthropometrica”. Anthropometry, as a scientific discipline, however, began with Johann Friedrich Blumenbach and Singh and Bhasin. Body composition assessment helps to growth pattern in adolescent; for body composition measurement research measures weight, height, and different kinds of circumferences. For adults, as for example, Body Mass Index (BMI) expressed as body weight (in kilogram) divided by height (in meter2) is widely used as a study of body fat in both developed and developing countries.
Chronic Energy Deficiency (CED) has been defined as a state of ‘steady’ or body energy stores. A BMI <18.5 kg/m2 is widely used as a practical measure underweight in which an individual is in energy balance irrespective of a loss in body weight. Different kind of morbidity factors is associated with underweight. CED is happens due to inadequate protein and energy intake even it happens when subjects suffer from different infectious disease.
Materials and Methods
Area of study
This study is carried out in outpatient of sub centre of a rural hospital of Medinipur district, some girls are school dropout and some are regular school goers, study group girls are 10-19 years old,100 girls in each group, Anthropometry are used to take measurement of height (anthropometre rod) weight (weighing machine), harpendent to take skinfold measurement.
Methods of the study
The present research investigation was cross-sectional in nature and fieldworks were carried out during the period of January-December 2011. The requite data were collected by structured and scheduled methods. Separate pre-tested” interview-schedule (form is utilized for participant. sociodemographic status.
Methodology
This study is done in rural hospital of Salboni block of Paschim Medinipur, to complete this study different anthropometry measurements are taken Anthropometre rod is used to measure height; weight is measured by weighing machine, Harpenden Caliper help in measuring skinfold of triceps and biceps and different circumferences are measured by measuring tape. To complete this study verbal consent of subjects are taken.
Sample size: To complete this study 1009 adolescent girls are interviewed; those girls are regular visitors of adolescent health centre; age range varies from 10-19 years girls. In every age group, there are 100 girls in every group. With help of software package for social science 19 analysis of data is done.
Results
Table 1 represents that mean height, weight, MUAC of study group is 151.02 cm (4.81), 44.56 (5.07), weight (kg) MUAC21.71 cm (2.85). Table 2 represents comparison of anthropometric value of pre-menarcheal and menarcheal girls. Figures 1-3 represent age wise pre-menarcheal, postmenarcheal, combined status of adolescent girls, Table 3 represents age wise standard deviation and mean of height, weight, and BMI.
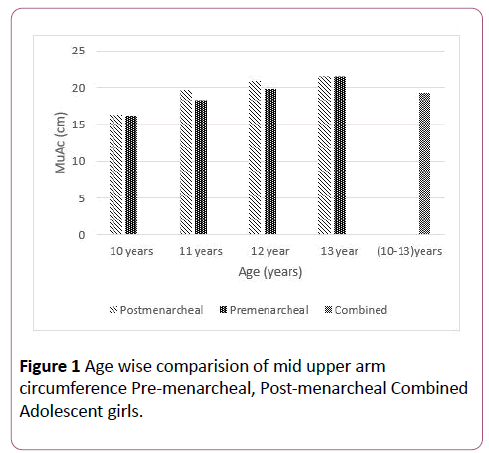
Figure 1: Age wise comparision of mid upper arm circumference Pre-menarcheal, Post-menarcheal Combined Adolescent girls.
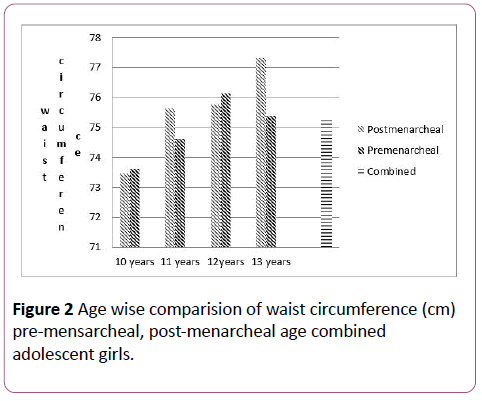
Figure 2: Age wise comparision of waist circumference (cm) pre-mensarcheal, post-menarcheal age combined adolescent girls.
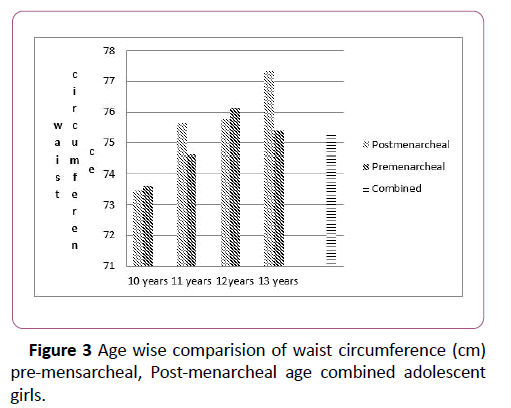
Figure 3: Age wise comparision of waist circumference (cm) pre-mensarcheal, Post-menarcheal age combined adolescent girls.
| Variable |
Mean (SD) |
25thPercentile |
50thPercentile |
95thPercentile |
| Height (cm) |
151.02 (4.81) |
147.9 |
151.3 |
158.2 |
| Weight (kg) |
44.56 (5.078) |
42.8 |
44.7 |
53.45 |
| Mid upper Arm Circumference (cm) |
21.71 (2.851) |
20.55 |
22.68 |
24.9 |
| Chest Circumference (cm) |
74.48 (7.07) |
70 |
74.7 |
86.65 |
| Waist Circumference (cm) |
78.32 (6.35) |
74.3 |
77.3 |
89.75 |
| Hip Circumference (cm) |
84.85 (6.57) |
80.5 |
85.4 |
95 |
Table 1: Mean, SD, percentiles of different anthropometric characteristics of adolescent Bengalee girls (n=1009).
| Age |
Mean |
N |
| 10 |
Post-menarcheal |
10.310000 |
50 |
| Pre-menarcheal |
9.000000 |
2 |
| Total |
10.259615 |
52 |
| 11 |
Post-menarcheal |
10.734286 |
70 |
| Pre-menarcheal |
9.000000 |
7 |
| Total |
10.576623 |
77 |
| 12 |
Post-menarcheal |
11.420000 |
80 |
| Total |
11.420000 |
80 |
| 13 |
Post-menarcheal |
11.939773 |
88 |
| Pre-menarcheal |
9.000000 |
1 |
| Total |
11.906742 |
89 |
| 14 |
Post-menarcheal |
12.433696 |
92 |
| Total |
12.433696 |
92 |
| 15 |
Post-menarcheal |
11.985567 |
97 |
| Total |
11.985567 |
97 |
| 16 |
Post-menarcheal |
12.224000 |
100 |
| Total |
12.224000 |
100 |
| 17 |
Post-menarcheal |
11.955556 |
99 |
| Pre-menarcheal |
9.000000 |
1 |
| Total |
11.926000 |
100 |
| 18 |
Post-menarcheal |
12.180808 |
99 |
| Pre-menarcheal |
9.000000 |
1 |
| Total |
12.149000 |
100 |
| 19 |
Post-menarcheal |
12.741284 |
109 |
| Total |
12.741284 |
109 |
| Total |
Post-menarcheal |
11.921267 |
884 |
| Pre-menarcheal |
9.000000 |
12 |
| Total |
11.882143 |
896 |
Table 2: Age wise comparison of anthropometric status of adolescence girls.
| Age |
Mean |
Std. Deviation |
| 10 |
Height |
146.01 |
4.94 |
| weight |
38.86 |
4.65 |
| BMI |
18.23 |
2.034 |
| 11 |
Height |
148.07 |
3.76 |
| weight |
41.63 |
5.29 |
| BMI |
18.96 |
2.19 |
| 12 |
Height |
149.800 |
3.82 |
| weight |
42.06 |
4.25 |
| BMI |
18.720 |
1.70 |
| 13 |
Height |
150.44 |
3.76 |
| weight |
43.30 |
4.09 |
| BMI |
19.125 |
1.57 |
| 14 |
Height |
151.53 |
4.41 |
| weight |
45.084 |
4.035 |
| BMI |
19.65 |
1.76 |
| 15 |
Height |
152.18 |
3.67 |
| weight |
45.99 |
3.92 |
| BMI |
19.86 |
1.60 |
| 16 |
Height |
152.48 |
3.52 |
| weight |
46.53 |
4.45 |
| BMI |
20.00 |
1.68 |
| 17 |
Height |
152.80 |
4.78 |
| weight |
46.86 |
3.56 |
| BMI |
20.02 |
1.21 |
| 18 |
Height |
153.15 |
4.97 |
| weight |
47.35 |
4.45 |
| BMI |
20.16 |
1.29 |
| 19 |
Height |
153.55 |
4.41 |
| weight |
47.62 |
3.62 |
| BMI |
20.17 |
1.0512 |
| Total |
Height |
151.02 |
4.81 |
| weight |
44.56 |
5.07 |
| BMI |
19.50 |
1.752 |
Table 3: Age wise comparison of height, weight, BMI of adolescence girls.
Discussion
Results revealed that boys were significantly heavier than girls from age 16 onwards [1]. In earlier study of adolescence rural girls have shown that their nutritional status does not relate their parent’s economic status the overall prevalence of under-nutrition was (48.3%) [2]. Menarcheal girls have shown higher anthropometric because of initiation menarche [3], santal girls of Bolpur 30.46% underweight previous study of earlier study has shown Salboni girls are underweight 35.4% (3) but Table 2 shows that BMI are under normal range, in this study upto 13 years anthropometric status is higher on postmenarcheal girls that’s prove to initiation menarche girls need to reach optimal height, weight, BMI for their menarche. In Meghalaya girls menarche ranges between 11 years to 17 years, 1 in 7 girls has knowledge about menarche prior to their experience, study. Present study girls’ mean age menarche is 12 years. Girls aware lack of aware about menstrual hygiene they do not clean public area scientifically use pond water to wash their underwear, this cause them more susceptible skin disease sexual infection, as time of men’s they do not clean them it causes monthly white discharge, unhealthy body, unprotect premartital relation influence of abortion without proper medical help causes severe condition. Adolescent girls of 10 years of age are all underweight on basis of MUAC (mid upper arm circumference) [4]; in adolescence period mid upper arm circumference, triceps all increases with age [3]. Urgent nutritional intervention programme should be given to them which shows that skilled labour parents’ girls mean weight is 44.54 (5.08) and mean height is 151.02 (4.82) [5]. Mean age at menarche is influenced by hip circumference and waist circumference [6,7]. Girls have poor knowledge on hygiene, they take bath in pond, which cause reproductive health related issue, like white discharge; they have poor concept on menstrual hygiene. To overcome all this, Government has taken initiative to start an adolescent friendly clinic where they get counselling on nutrition, health and hygiene.
Conclusion
In rural area nurse and counsellors do outreach programme where in a meeting with adolescents they deliver health talk which help them to fight against all difficulties. in respect to health, psychosocial issue.
References
- Bisai S, Bose K, Ghosh D, De K (2011) Growth pattern and prevalence of underweight and stunting among rural adolescents. J Nepal peadtrsoc 31: 17-24.
- De K, Das S, Bose K, Chakraborty R (2013) Nutritional status of rural Bengalese girls aged 10-18 years of Salboni, PaschimMedinipur, West Bengal, India. Asian J Biol life Sci 2: 1.
- De K (2016) Nutritional status and menarcheal age of rural adolescent girls of salboni block ofPaschimMedinipur, West Bengal, India. J Child AdolescBehav 4: 1-5.
- De K (2016) Assessment of nutritional status of adolescent girls by mid-upper arm circumferences of PaschimMedinipur, India. Primary Health Care: Open Access 4: 10.
- De K (2016) Influence of socio-economic status on the nutritional status of rural adolescent girls. Anthropol 4: 1-5.
- De K (2016) Physical growth and relation of menarche with anthropometry. Anthropol 4: 172.
- De K(2017) Measurement of body composition by upper arm anthropometry.CurrPediatr Res 21: 112-115.

