Keywords
Carcinoma, Hepatocellular; Hepacivirus; Hepatitis B virus; Pancreatic Carcinoma; Pancreatic Neoplasms; Risk Factors
INTRODUCTION
Pancreatic adenocarcinoma is a very aggressive disease with a poor prognosis and an overall fiveyear survival less than 5% [1], accounting for about 250,000 deaths worldwide yearly [2]. Advanced stage at presentation, aggressive behavior, early metastatic dissemination and lack of effective systemic therapies explain the dismal outcome of this neoplasia [3, 4]. To date, causes of this malignancy are not yet completely understood [4]. Cigarette smoking habit [5] and family history strongly increase the risk of this tumor [6] as well as a more elevated incidence of pancreatic adenocarcinoma has been observed in patients with high dietary fat consumption [7], alcohol abuse [8], diabetes mellitus [9], metabolic syndrome [10, 11] and chronic pancreatitis history [12]. Therefore, a better knowledge of risk factors for pancreatic adenocarcinoma development is absolutely required. Epidemiological and experimental researches suggest that about 15-20% of human cancers are associated in some way with chronic infection [13].
Bacteria- and Viral-Related Infections and Risk of Pancreatic Cancer
In the last decade, a large series of studies reported that both bacteria and viruses may play a role as risk factors for pancreatic carcinogenesis. In particular, concerning infections induced by bacteria, a recent meta-analysis has considered six observational studies, suggesting that Helicobacter pylori infection increases risk of pancreatic cancer development [14]. According to previous studies, it has been already reported that this pathogen is involved in the pathogenesis of peptic ulcer disease [15] as well as of gastric carcinoma and lymphoma [16]. Additional researches proposed a possible relationship between oral pathologies, such as periodontitis, and a higher risk of pancreatic cancer [17, 18]. It has been also suggested that an association exists between variations of patients’ oral flora (in particular some species of salivary microorganisms, such as Neisseria elongate and Streptococcus mitis) and an enhanced incidence of pancreatic diseases, such as neoplasia in this organ [19]. Nevertheless, it is not yet completely understood whether oral microbiota has a causative role in the process of pancreatic carcinogenesis.
Some studies have underlined an association between some viral infection and an increased probability of pancreatic adenocarcinoma. In particular, it has been reported that patients with HIV-related infection, during highly active antiretroviral therapy (HAART) [20, 21], present a significantly higher risk of this tumor in comparison with general population, although other studies did not confirm this relationship [22]. Furthermore, it has been shown an association between exposure to poultry oncogenic viruses and an increased probability of pancreatic adenocarcinoma. Recent reports have suggested that hepatitis B virus (HBV) and hepatitis C virus (HCV) may be involved in the process of oncogenesis in the pancreas. One of the pathogenetic mechanisms by means of which these pathogens promote cancer initiation and progression is represented by the development of a persistent local inflammation, at sites where chronic infection is established [23].
HBV and HCV Oncogenic Role
HBV and HCV are liver-tropic pathogens with wellknown oncogenic properties. It has been estimated that these microorganisms infect approximately 400 and 180 million people, respectively. Therefore, they represent a serious public health problem in the world. HBV and HCV may cause a necroinflammatory hepatic disease with different patterns of severity and course. Persistent liver injury represents a high risk condition for developing cirrhosis and hepatocellular carcinoma [24, 25]. Furthermore, a relationship between HBV/HCV and intrahepatic cholangiocarcinoma [26] and some forms of non-Hodgkin lymphoma have been reported [27, 28]. However, antigens and replicative sequences of both pathogens have been also detected in different extra-hepatic tissues, including pancreas [29, 30]. It is well-known that an association exists between HBV- and HCV-related hepatitis and acute pancreatitis [31, 32]. These pathogens might replicate in pancreas, inducing persistent inflammation and injury in this organ. Experimental data suggest that the establishment of a chronic damage may induce the development of metaplasia in tissues where an inflammatory process occurs [33]. This event represents a high risk condition for malignant transformation in involved organs, as well as in pancreas, because it promotes a permissive microenvironment for carcinogenic stimuli [34]. In addition it has to be considered that, according to available data, liver and pancreas originate from common multipotent cells of endoderm origin [35, 36] and that experimental studies have suggested that hepatocytes may trans-differentiate into pancreatic cells and vice versa, when they are cultured upon definite conditions [37, 38]. These data suggest the hypothesis that pancreas is not merely a reservoir of HBV and HCV, but it might support their replication. Therefore, both viruses may have a role not only in liver cancer development, but also in the initiation and progression of pancreatic carcinogenesis. Nevertheless, although in the last decade of the twentieth century some researchers have detected antigens and/or intermediate replicative forms of HBV [39, 40, 41] and HCV [32] in pancreas, no further studies have been performed soon afterwards with the aim of investigating the possible oncogenic activity of both pathogens in this organ. Recently, the interest in the study of the possible association between HBV or HCV infection and pancreatic cancer development, has progressively increased and some researchers have been designed to investigate this topic. In addition, the possible mechanisms involved in the process of HBV- or HCV-induced malignant transformation have been synthesized in a recent paper [42].
Epidemiological Researches on HBV and HCV Oncogenic Role in the Pancreas
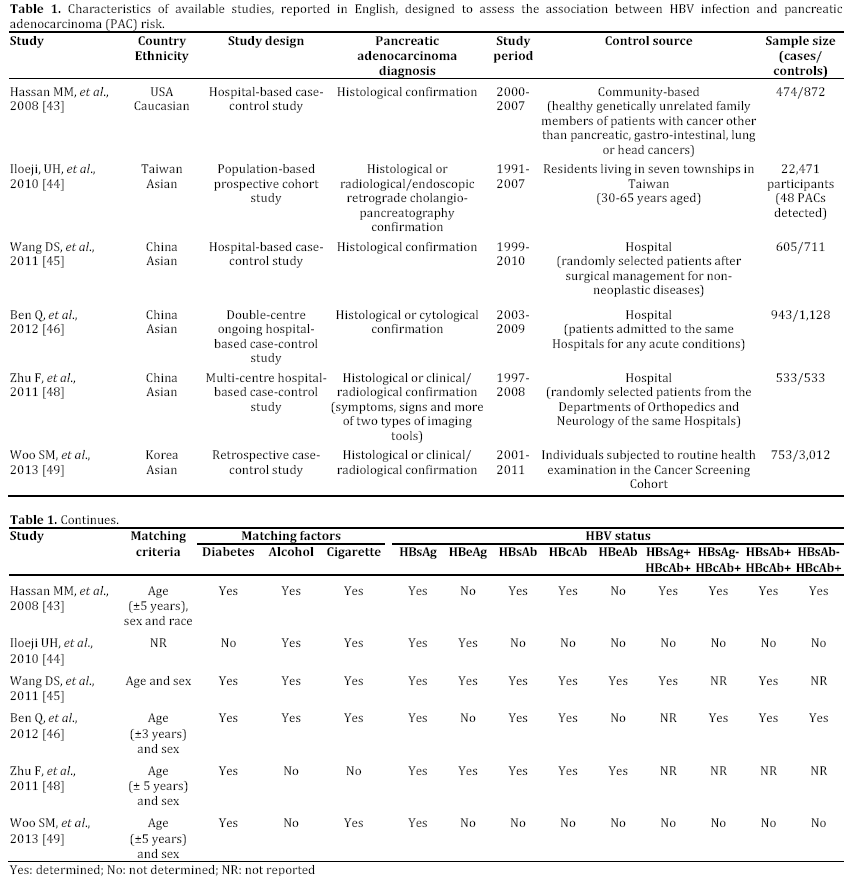
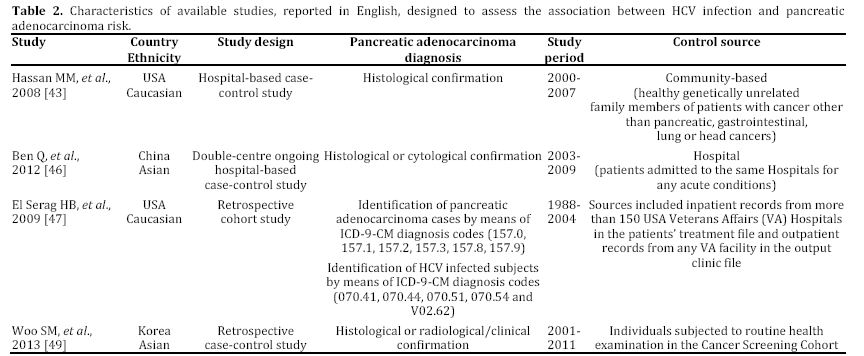
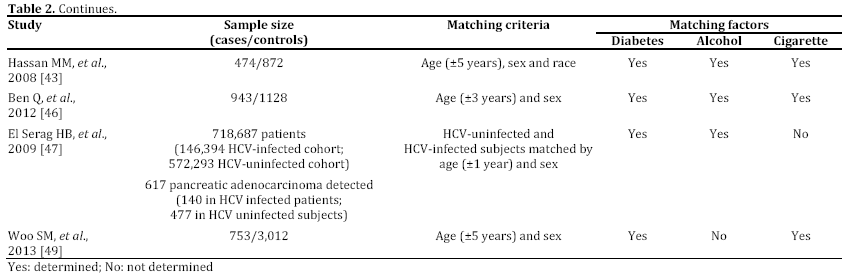
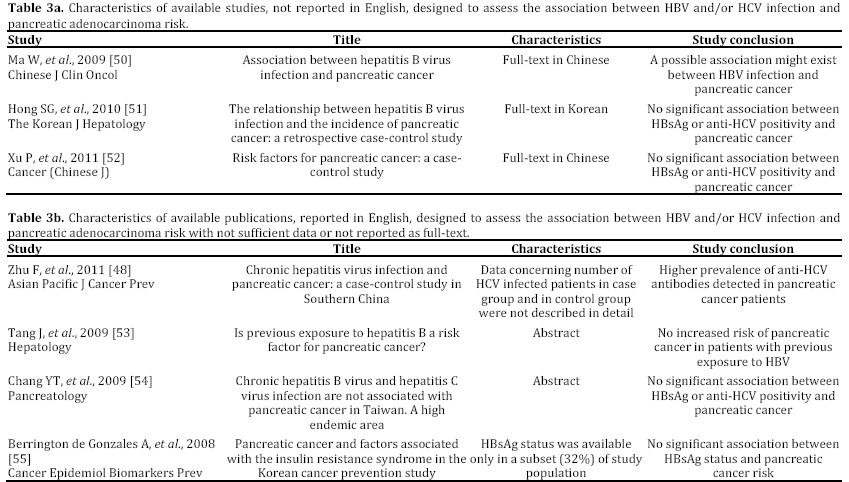
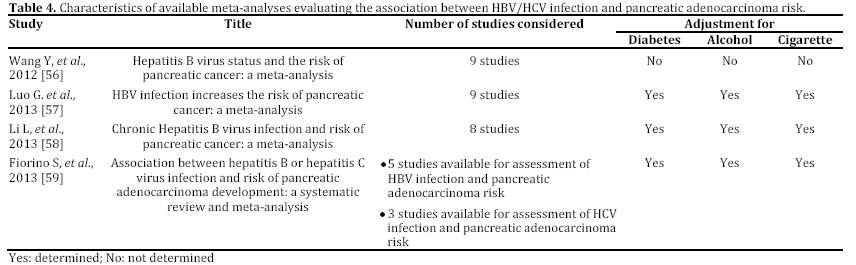
In the last years, some epidemiological studies have been published, suggesting that HBV and HCV may be risk factors not only for liver, but also for pancreatic cancer. Most of these studies, both casecontrol or cohort trials, have been reported in English and performed in a period ranging from 2008 to 2012 and mainly carried out in China [43, 44, 45, 46, 47, 48, 49] (Tables 1 and 2). Some publications are in Chinese or in Korean [50, 51, 52], or in English but not in full-text, or with insufficient data [53, 54, 55] (Table 3). In the last two years, between the end of 2012 and the beginning of 2013, almost 4 meta-analyses, examining the possible association between HBV and HCV infection and pancreatic carcinogenesis, have been published (Table 4). The results of these pooled-analyses support the hypothesis that both viruses may be risk factors also for pancreatic cancer [56, 57, 58, 59] and that patients with signs of persistent HBV or HCV infection have an increased probability to develop this malignancy in comparison to controls without previous contact with both viruses. On the whole, presence of HBsAg is associated with a higher incidence of pancreatic adenocarcinoma in comparison with individuals never exposed to HBV [56, 57, 58, 59]. Furthermore, although no statistically significant relationship has been found between anti-HCV positivity and risk of carcinogenesis in pancreas, a borderline value has been observed in this analysis [59]. The small number of available studies (n=3) assessing this association accounts for this indefinite result. Additional investigations are required to confirm this possible correlation. Therefore, the results from these recent researches provide for the first time very interesting insights on the possible role of hepatotropic viruses in pancreatic adenocarcinoma initiation and progression as well as they may contribute to develop a new field of study. Nevertheless, several questions and uncertain points, requiring a better definition and explanation, remain. In particular, the following problems have to be underlined.
a) Available studies, concerning this topic, are still few, heterogeneous in design, and, in some cases, underpowered.
b) Nearly all researches have been performed in Asian populations and, in particular, in China, where viral liver infections are more prevalent. To date, no studies have been carried out in Europe and in Africa, whereas only two trials have been accomplished in Northern America (USA) [43, 47]. Therefore, the validity of the available researches and meta-analyses is limited to Asian peoples and it may be erroneous to extend their results to non Asian peoples.
c) Concerning HBV infection, it should be considered that in high HBV endemic regions worldwide, such as China and Taiwan, HBsAg prevalence is about 8%, whereas in low HBV endemic countries [60], including USA or Northern Europe, global HBsAg prevalence is less than 2% in general population [61]. In these areas, most of subjects with a previous contact with HBV have a serum profile characterized by absence of HBsAg and by presence of HBcAb with or without HBsAb. Therefore, these individuals present two different types of serum HBV antigen/antibody markers, including HBsAg-/HBcAb+/HBsAb- or HBsAg- /HBcAb+/HBsAb+ patterns. In the past these profiles have been considered as signs of complete recovery from a past exposure to HBV infection without or with natural immunity. Recently, progressive advancement in molecular biology and introduction of highly sensitive techniques for HBV genotyping allowed us to understand that this virus is able to persist and replicate at low level also in individuals with or without presence of serum HBcAb and/or HBsAb. In these HBsAg negative subjects, HBV-DNA is detectable in hepatic tissue, although it may be absent in serum. This condition is defined as “occult” HBV infection [62]. This term underlines the circumstance that this microorganism has not been completely eradicated, but it persists in the infected host. The biological and clinical significance of this serum and tissue pattern “in vivo” is uncertain and it has not yet been definitively understood. Therefore, presence of both antigen/antibody profiles (HBsAg-/HBcAb+/HBsAband HBsAg-/HBcAb+/HBsAb+) might be associated with a significant increased probability to develop pancreatic cancer, even if both viral profiles would mark the complete resolution of HBV infection. Unfortunately, to date, only 3 studies investigated this potential relationship. Therefore, no definitive conclusions may be drawn.
d) It is unclear whether some HBV or HCV genotypes may be associated with an increased risk of developing pancreatic cancer in comparison to different genotypes, according also with difference in their geographical distribution.
e) It has not be definitively explained whether some risk factors for pancreatic cancer, such as smoking status, history of diabetes and alcohol use, in association with HBV and/or HCV infection, may increase the risk to develop this type of malignancy.
Conclusions
In conclusion, new interesting insights are emerging from epidemiological studies, assessing the possible relationship between HBV/HCV infection and risk of pancreatic cancer development. However, several problems and uncertain points remain and they have to be accurately investigated and explained. Therefore, the planning of well-designed studies, focusing on populations of different regions in the world and enrolling a larger number of patients, is indispensable. This approach may help to establish the real impact of both viruses in pancreatic carcinogenesis and eventually define pathogenetic mechanisms involved in this process.
Acknowledgements
The Authors thanks Dr. Simonetta Righi (Integrate Library, S. Orsola- Malpighi Hospital, “Alma Mater Studiorum” - University of Bologna, Bologna, Italy) for her support in the search of scientific bibliography
Conflict of interest
None declared
References
- Jemal A, Siegel R, Ward E, Murray T, Xu J, Thun MJ. Cancer statistics, 2007. CA Cancer J Clin. 2007;57:43-66.
- Krejs GJ. Pancreatic cancer: epidemiology and risk factors. Dig Dis 2010;28:355-8.
- Schnelldorfer T, Ware AL, Sarr MG, Smyrk TC, Zhang L, Qin R, Gullerud RE, Donohue JH, Nagorney DM, Farnell MB. Long-term survival after pancreatoduodenectomy for pancreatic adenocarcinoma: is cure possible? Ann Surg. 2008;247(3):456-62.
- Hidalgo M. Pancreatic cancer. N Engl J Med 2010 29;362:1605-17.
- Li D, Day RS, Bondy ML, Sinha R, Nguyen NT, Evans DB et al. Dietary mutagen exposure and risk of pancreatic cancer. Cancer Epidemiol Biomarkers Prev. 2007;16:655-61.
- Jacobs EJ, Rodriguez C, Newton CC, Bain EB, Patel AV, Feigelson HS et al. Family history of various cancers and pancreatic cancer mortality in a large cohort. Cancer Causes Control. 2009;20:1261-69.
- Larghi A, Verna EC, Lecca PG, Costamagna G. Screening for pancreatic cancer in high-risk individuals: a call for endoscopic ultrasound. Clin Cancer Res 2009;15:1907-14.
- Apte M, Pirola R, Wilson J. New insights into alcoholic pancreatitis and pancreatic cancer. J Gastroenterol Hepatol. 2009;24:S51-56.
- Chari ST, Leibson CL, Rabe KG, Timmons LJ, Ransom J, de Andrade M et al. Pancreatic cancer-associated diabetes mellitus: prevalence and temporal association with diagnosis of cancer. Gastroenterology 2008;134:95-101.
- Rosato V, Tavani A, Bosetti C, Pelucchi C, Talamini R, Polesel J et al. Metabolic syndrome and pancreatic cancer risk: a case-control study in Italy and meta-analysis. Metabolism 2011; 60: 1372-8.
- Johansen D, Stocks T, Jonsson H, Lindkvist B, Björge T, Concin H et al. Metabolic factors and the risk of pancreatic cancer: a prospective analysis of almost 580,000 men and women in the Metabolic Syndrome and Cancer Project. Cancer Epidemiol Biomarkers Prev 2010; 19: 2307-17.
- Lowenfels AB, Maisonneuve P, Lankisch PG. Chronic pancreatitis and other risk factors for pancreatic cancer. Gastroenterol Clin North Am 1999; 28:673-85.
- Kuper H, Adami HO, Trichopoulos D. Infections as a major preventable cause of human cancer. J Intern Med. 2000;248(3):171-83.
- Trikudanathan G, Philip A, Dasanu CA, Baker WL. Association between Helicobacter pylori Infection and Pancreatic Cancer. A Cumulative Meta-Analysis. J Pancreas 2011; 12: 26-31.
- Marshall BJ. Helicobacter pylori. Am J Gastroenterol 1994; 89(8 Suppl):S116-28.
- Correa P, Houghton J. Carcinogenesis of Helicobacter pylori. Gastroenterology 2007; 133: 659-72.
- Michaud DS, Joshipura K, Giovannucci E, Fuchs CS. A prospective study of periodontal disease and pancreatic cancer in US male health professionals. J Natl Cancer Inst 2007; 99: 171-5.
- Stolzenberg-Solomon RZ, Dodd KW, Blaser MJ, Virtamo J, Taylor PR, Albanes D. Tooth loss, pancreatic cancer and Helicobacter Pylori. Am J Clin Nutr 2003; 78: 176-81.
- Farrell JJ, Zhang L, Zhou H, Chia D, Elashoff D, Akin D et al. Variations of oral microbiota are associated with pancreatic diseases including pancreatic cancer. Gut 2012; 61: 582-88.
- Serraino D, Dal Maso L, De Paoli A, Zucchetto A, Bruzzone S, Camoni L et al. On changes in cancer mortality among HIV-infected patients: is there an excess risk of death from pancreatic cancer? Clin Infect Dis 2009; 49: 481-482.
- Engels EA, Biggar RJ, Hall HI, Cross H, Crutchfield A, Finch JL, et al. Cancer risk in people infected with human immunodeficiency virus in the United States. Int J Cancer 2008; 123: 187-94.
- Simard EP, Pfeiffer RM, Engels EA. Spectrum of cancer risk late after AIDS onset in the United States. Arch Intern Med. 2010; 170: 1337-45.
- Hussain SP, Harris CC. Inflammation and cancer: an ancient link with novel potentials. Int J Cancer 2007;121(11):2373-80.
- Dandri M, Locarnini S. New insight in the pathobiology of hepatitis B virus infection. Gut 2012; 2012;61 Suppl 1:i6-17. doi: 10.1136/gutjnl-2012-302056.
- Poynard T, Ratziu V, Charlotte F, Goodman Z, McHutchison J, Albrecht J. Rates and risk factors of liver fibrosis progression in patients with chronic hepatitis C. J Hepatol 2001; 34: 730-9.
- Zhou Y, Zhao Y, Li B, Huang J, Wu L, Xu D, Yang J, He J. Hepatitis viruses infection and risk of intrahepatic cholangiocarcinoma: evidence from a meta-analysis. BMC Cancer. 2012 Jul 16;12:289. doi: 10.1186/1471-2407-12-289.
- Jeong SH. HBV infection as a risk factor for non-Hodgkin lymphoma. Lancet Oncol. 2010;11(9):806. doi: 10.1016/S1470-2045(10)70182-0.
- Fiorilli M, Mecucci C, Farci P, Casato M. HCV-associated lymphomas. Rev Clin Exp Hematol. 2003;7(4):406-23.
- Jin Y, Gao H, Chen H, Wang J, Chen M, Li G, Wang L, Gu J, Tu H. Identification and impact of hepatitis B virus DNA and antigens in pancreatic cancer tissues and adjacent non-cancerous tissues. Cancer Lett. 2013. pii: S0304-3835(13)00224-3. doi: 10.1016/j.canlet.2013.03.001.
- Yan FM, Chen AS, Hao F, Zhao XP, Gu CH, Zhao LB et al. Hepatitis C virus may infect extrahepatic tissues in patients with hepatitis C. World J Gastroenterol. 2006:805-11.
- Alvares-Da-Silva MR, Francisconi CF, Waechter FL. Acute hepatitis C complicated by pancreatitis: another extrahepatic manifestation of hepatitis C virus? J Viral Hepat. 2000;7(1):84-6.
- Yuen MF, Chan TM, Hui CK, Chan AO, Ng IO, Lai CL. Acute pancreatitis complicating acute exacerbation of chronic hepatitis B infection carries a poor prognosis. J Viral Hepat. 2001;8(6):459-64.
- Parsa I, Longnecker DS, Scarpelli DG, Pour P, Reddy JK, Lefkowitz M. Ductal metaplasia of human exocrine pancreas and its association with carcinoma. Cancer Res. 1985;45(3):1285-90.
- Reichert M, Rustgi AK. Pancreatic ductal cells in development, regeneration, and neoplasia. J Clin Invest. 2011;121(12):4572-8. doi: 10.1172/JCI57131.
- Zaret KS. Genetic programming of liver and pancreas progenitors: lessons for stem-cell differentiation. Nat Rev Genet. 2008;9(5):329-40.
- Wandzioch E, Zaret KS. Dynamic signaling network for the specification of embryonic pancreas and liver progenitors. Science 2009;324(5935):1707-10.
- Dabeva MD, Hwang SG, Vasa SR et al. Differentiation of pancreatic epithelial progenitor cells into hepatocytes following transplantation into rat liver. Proc Natl Acad Sci U S A. 1997;94(14):7356-61.
- Wang RY, Shen CN, Lin MH, Tosh D, Shih C. Hepatocyte-like cells transdifferentiated from a pancreatic origin can support replication of hepatitis B virus. J Virol. 2005;79(20):13116-28.
- Shimoda T, Shikata T, Karasawa T, Tsukagoshi S, Yoshimura M, Sakurai I. Light microscopic localization of hepatitis B virus antigens in the human pancreas. Possibility of multiplication of hepatitis B virus in the human pancreas. Gastroenterology 1981;81(6): 998-1005.
- Dejean A, Lugassy C, Zafrani S, Tiollais P, Brechot C. Detection of hepatitis B virus DNA in pancreas, kidney and skin of two human carriers of the virus. J Gen Virol. 1984;65 (Pt 3): 651-5.
- Hohenberger P. The pancreas as target organ for hepatitis B virus-immunohistological detection of HBsAg in pancreatic carcinoma and chronic pancreatitis. Leber Magen Darm. 1985;15(2):58-63.
- Fiorino S, Lorenzini S, Masetti M, Deleonardi G, Grondona AG, Silvestri T, Chili E, Del Prete P, Bacchi-Reggiani L, Cuppini A, Jovine E. Hepatitis B and C virus infections as possible risk factor for pancreatic adenocarcinoma. Med Hypotheses. 2012, 79: 678-97.
- Hassan MM, Li D, El-Deeb AS, Wolff RA, Bondy ML, Davila M et al. Association between hepatitis B virus and pancreatic cancer. J Clin Oncol 2008; 26:4557-62.
- Iloeje UH, Yang HI, Jen CL, Su J, Wang LY, You SL, Lu SN, Chen CJ. Risk of pancreatic cancer in chronic hepatitis B virus infection: data from the REVEAL-HBV cohort study Liver Int. 2010; 30 (3): 423–9.
- Wang DS, Chen DL, Ren C, Wang ZQ, Qiu MZ, Luo HY, Zhang DS, Wang FH, Li YH, Xu RH. ABO blood group, hepatitis B viral infection and risk of pancreatic cancer. Int J Cancer. 2012;131(2):461-8.
- Ben Q, Li Z, Liu C, Cai Q, Yuan Y, Wang K, Xiao L, Gao J, Zhang H. Hepatitis B virus status and risk of pancreatic ductal adenocarcinoma: a case-control study from China. Pancreas. 2012; 41(3):435-40.
- El-Serag HB, Engels EA, Landgren O, Chiao E, Henderson L, Amaratunge HC et al. Risk of hepatobiliary and pancreatic cancers after hepatitis C virus infection: A population-based study of U.S. veterans. Hepatology 2009;49:116-23.
- Zhu F, Li HR, Du GN, Chen JH, Cai SR. Chronic hepatitis B virus infection and pancreatic cancer: a case-control study in southern China. Asian Pac J Cancer Prev. 2011;12(6):1405-8.
- Woo SM, Joo J, Lee WJ, Park SJ, Han SS, Kim TH et al. Risk of pancreatic cancer in relation to ABO blood group and hepatitis C virus infection in Korea: a case-control study. J Korean Med Sci. 2013;28(2):247-51. doi: 10.3346/jkms.2013.28.2.247.
- Ma W, Xie D, Cao W, Yang Q, Jiang Z, Chen D et al. Association between hepatitis B virus infection and pancreatic cancer. Chinese Journal of Clinical Oncology 2009 36:24 (1388-1390).
- Hong SG, Kim JH, Lee YS, Yoon E, Lee HJ, Hwang JK et al. The relationship between hepatitis B virus infection and the incidence of pancreatic cancer: a retrospective case-control study. Korean J Hepatol. 2010;16(1):49-56.
- Xu P, Huang Q, Liu C, Xie F, Shao F, Zhu C et al. Risk factors for pancreatic cancer: a case-control study. Cancer (Chinese J) 2011; 31: 653-7.
- Tang J, Lamerato L, Sheehan MJ, Krajenta R, Gordon SC. Is previous exposure to hepatitis B a risk factor for pancreatic cancer? Hepatology 2009; 50: 988A.
- Chang YT, Hsu C, Wei SC, Huang GT, Hsu JC, Wong JM et al. Chronic hepatitis B and hepatitis C virus infection are not associated with pancreatic cancer in Taiwan-A high endemic area. Pancreatology 2009; 9: 518A.
- Berrington de Gonzalez A, Yun JE, Lee SY, Klein AP, Jee SH. Pancreatic cancer and factors associated with the insulin resistance syndrome in the Korean cancer prevention study. Cancer Epidemiol Biomarkers Prev 2008;17:359-64.
- Wang Y, Yang Sl, Song FJ, Cao SY, Yin X, Xie J. et al. Hepatitis B virus status and the risk of pancreatic cancer: a meta-analysis. Eur J Cancer Prev 2012.
- Luo G , Hao NB , Hu CJ , Yong X , Lü MH , Cheng BJ, et al. HBV infection increases the risk of pancreatic cancer: a meta-analysis. Cancer Causes Control 2013; 24: 529-37.
- Li L, Wu B, Yang LB, Yin GC, Liu JY. Chronic Hepatitis B virus infection and risk of pancreatic cancer: a meta-analysis. Asian Pac J Cancer Prev. 2013; 14: 275-279.
- Fiorino S, Chili E, Bacchi-Reggiani L, Masetti M, Deleonardi G, Grondona AG, et al. Association between hepatitis B or hepatitis C virus infection and risk of pancreatic adenocarcinoma development: A systematic review and meta-analysis. Pancreatology 2013; 2: 147-60.
- Liang X, Bi S, Yang W, Wang L, Cui G, Cui F, et al. Epidemiological serosurvey of hepatitis B in China--declining HBV prevalence due to hepatitis B vaccination. Vaccine. 2009; 27(47):6550-7.
- Centers for Disease Control and Prevention (CDC). Screening for chronic hepatitis B among Asian/Pacific Islander populations--New York City, 2005. MMWR Morb Mortal Wkly Rep. 2006;55(18):505-9.
- Larrubia JR. Occult hepatitis B virus infection: a complex entity with relevant clinical implications. World J Gastroenterol. 2011;17(12):1529-30.

