What is known on this subject
• The Somali community in Birmingham represents a significant proportion of the growing black African
population which has the lowest preschool immunisation rates.
• Previous research conducted in Somalia has highlighted the importance of perceptions about immunisations
which are shaped by cultural factors.
• Little is known about the views of the Somali population in the UK regarding preschool immunisation,
and how their beliefs shape immunisation practices.
What this paper adds
• Opinions among the Somali community are generally positive, although there are specific concerns and
anxieties about the MMR vaccine, most notably due to its purported link with autism.
• The perceptions and immunisation practices of Somali women are shaped by culture, religious
interpretation and personal experience.
• There is a lack of reliable and culturally appropriate information that addresses the Somali community’s
specific concerns and anxieties about childhood vaccinations. This should be addressed in order to
improve community confidence and trust in immunisation programmes.
Key words
attitudes, beliefs, ethnicity, immunisation,
preschool, Somali
Introduction
The first vaccination programme in the UK was
launched in 1940, with the immunisation of children
against diphtheria (Salisbury et al, 2006). Immunisation
rates across England today are monitored by the
Health Protection Agency (HPA), and have steadily
increased over the last 50 years. TheHPArecommends
that 80–95% coverage of a population is needed in
order to achieve immunity against particular diseases.
The term herd immunity is used to refer to ‘the
protection of populations from infection which is
brought about by the presence of immune individuals’
(Fine, 1993). By 2010, 95.3% of children across theUK
had received DTP3 by their second birthday, yet only
88.2% were up to date with the measles, mumps
and rubella (MMR) vaccine (National Health Service,
2010). Childhood vaccination remains one of the
most important public health interventions of the
21st century, and is thought to avert between two
and three million deaths worldwide per year (World
Health Organization, 2012). A highly controversial
publication in the Lancet by Wakefield and colleagues
in 1998 sparked national and international debate by
claiming a link between the MMR vaccine and the
development of autistic behaviours (Wakefield et al,
1998). Despite the fact that the research was subsequently
discredited, this accusation has had a significant
impact on the willingness of parents in the UK to
vaccinate their children against MMR, and as a result
the uptake of vaccination has decreased. There is little
information about whether migrants who are parents
share the views of the host population about MMR
vaccination.
Background
Birmingham is the second largest city in England, and
has a very diverse population of over one million people
that includes a growing number of black Africans
(Birmingham City Council, 2009). A health equity
profile of childhood immunisation across Birmingham
showed that black Africans have the lowest uptake of preschool immunisations and are the fastest growing
ethnic minority (Pickard, 2005; Birmingham City
Council, 2009). The Somali community has contributed
significantly to this growth, and currently stands at
approximately 40 000 (Jones, 2007). This may be
attributable to a range of factors, such as cultural
issues and the possible impact of pre-migration parental
experiences, but there is no evidence to support
these or any other possible explanations for the low
uptake of immunisation. It is possible that the views
of Somali mothers may have been influenced by the
Wakefield publication, which generated confusion
and mistrust among many parents and healthcare
professionals, regardless of their ethnic and cultural
backgrounds. It is therefore important to gain a better
understanding of the health beliefs of the Somali
community in Birmingham with regard to preschool
immunisation in order to improve uptake and help to
achieve herd immunity.
LaFond (1993) explored the views of mothers in
Somalia about preschool immunisation using
community-based focus groups and informal interviews.
The study aimed to understand why Somalia
had some of the lowest national immunisation rates in
the world, despite joining a pledge to achieve universal
child immunisation by 1990 (UNICEF, 1996). The
study uncovered the belief that immunisation was not
effective against diseases such as polio and neonatal
tetanus, which were believed to have spiritual causes.
Forced vaccination campaigns in Somalia also had a
negative effect on mothers’ confidence in the safety of
vaccinations; many mothers believed that the tetanus
vaccine given to women of childbearing agewas a form
of contraception and was being used by the government
to arrest population growth. A more recent
study conducted in Somalia addressed various aspects
of health, including preschool immunisation. It found
that a lack of belief in the effectiveness of immunisations,
particularly among fathers, led to poor uptake
of immunisation services (Food Security Analysis
Unit, 2007).
Twenty years of political and civil unrest in Somalia
have led to one of the highest rates of emigration in
the world (Central Intelligence Agency, 2012). Many
migrants travel considerable distances through several countries, such as Holland, Sweden and Norway,
before they arrive in the UK, where they face new
challenges in integrating into a foreign society while
trying to maintain traditional customs and practices.
Condon (2002) used focus group methodology and
semi-structured interviews to explore attitudes to
preschool immunisation among 21 minority ethnic
women in Bristol, England. She found that Pakistani,
Somali and African Caribbean mothers had a positive
attitude towards immunisation, although they differed
in their desire for increased provision of information.
Research conducted by Kulane et al (2007)
with migrant Somali communities in Sweden explored
the specific views of Somali parents in Stockholm with
regard to acceptance of the vaccine against measles,
parotitis and rubella. They found that Somali parents
recognised the importance of immunisation, but were
fearful of the MPR vaccine as a result of media reports
of its supposed link with autism.
Aim of this project
Little is known about the Somali population in the UK
or about the views of Somalis with regard to preschool
immunisation. The aim of the study reported here was
to explore these views as a basis for ensuring a culturally
appropriate service.
Methods
As this study was broadly exploratory in nature, we
adopted an idiographic approach with a view to
describing individual participants’ accounts of their
experiences of and perspectives on childhood immunisation
from within their own framework of
understanding and meaning. This community-based
qualitative study drew on the insights into strategies
that respond to sensitivities in relation to ethnicity and
culture (Elam and Fenton, 2003), paying particular
attention to working with individuals in the community
who could act as cultural brokers, building
trust and providing clear explanations of the possible
benefits of the study for the community.
The study was reviewed by the Internal Ethics
Committee at the University of Birmingham. This
committee is responsible for the ethical review of
student projects. A favourable ethical opinion was
received.
Data collection
Data were collected using semi-structured interviews
that facilitated the exploration of the participants’
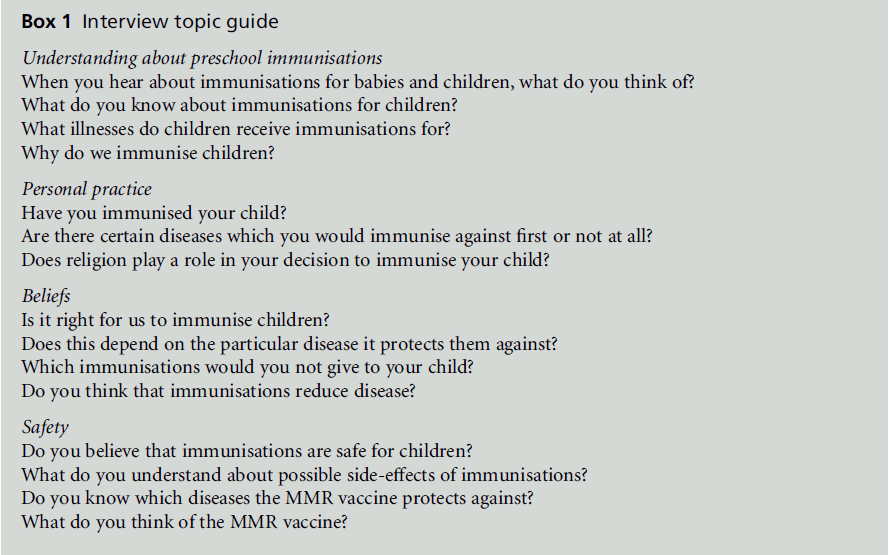
health beliefs. A topic guide was developed from the
results of previous research as well as lessons learned
from a pilot interview. The guide allowed for further
questions to emerge from the dialogue to enable
clarification and exploration of particular views or
opinions (DiCicco-Bloom and Crabtree, 2006) (see
Box 1). Women were invited to take part if they were
over 18 years old, born in Somalia, the mother of at
least one child under 5 years old (no minimum age)
and resident in Birmingham. These criteria were used
to guide purposive sampling of participants. This
refers to systematic, non-random sampling whereby
‘informants are identified because they will enable
exploration of a particular aspect of behaviour’ (Mays
and Pope, 1995, p. 110). Snowball sampling was also
employed; this method is often used in research being
undertaken among a population that is normally hard
to reach (Penrod et al, 2003). Purposive sampling is
usually based on the judgement of the researcher and
the given resources in terms of cases available for
sampling (Mason, 2002). According to Teddlie and
Yu (2007), purposive sample sizes are typically below
30. In our study, a sample size of 20–25 participants
was estimated to be sufficient to reach data saturation,
that is, the point at which additional data are unlikely
to yield new information or require revisions to be
made to findings that have already been developed
(Holloway andWheeler, 2010).However,we also used
snowball sampling by inviting the women to identify
suitable potential participants from their social networks
(Faugier and Sargeant, 1997).
Centres were accessed via telephone numbers provided
by Birmingham City Council (2012). Contact
was made with those in leadership roles in the centres
who then provided access to the Somali women.
Potential participants were approached at the centres
and verbally informed of the purpose of the study, as
well as being given an information sheet in both
English and Somali. The women then had time to
consider whether to participate, and an interview was
scheduled at a later date with those who agreed to take
part. Participants were not asked to sign a written
consent form, as such formalisation of the consent
process could be perceived as alienating, as well as
undermining the rapport that had been developed
with participants (Redwood et al, 2012). Instead,
participants were provided with written information
as well as being given the opportunity to ask questions
or withdraw from the study. Verbal consent was
audio-recorded.
Interviews lasted around 20–30 minutes and took
place at the centres that had facilitated the recruitment
of participants. Lay interpreters were made available
for participants whose English-language skills were
insufficient. Participants were also asked to consent to
the interview being recorded on a digital audio recorder.
The participants’ travel expenses were reimbursed
and they received a shopping voucher in
appreciation of their participation.
Analysis
Interviews were recorded and transcribed verbatim.
Data collection and data analysis were carried out
concurrently in order to inform sampling as well as
to indicate when data saturation had been reached
(Hammersley, 2001). Data were examined using inductive
thematic analysis (Braun and Clarke, 2006),
with the development of the themes being driven by a
concern for identifying participants’ experiences, perspectives
and beliefs that had the potential to influence
decisions to vaccinate their children. Initially, a subset
of interviews was read independently by both researchers
to search for meanings and salient issues in
and across the data. Subsequently, initial codes were
identified, such as ‘immunisation as protection from
potential disease’, ‘risks associated with non-vaccination’,
‘risks associated with vaccination’, ‘fears about
autism’ and ‘personal experiences of vaccination
practices in Somalia.’ All of the transcripts were then
coded by the first author and a subset was checked for
consistency by the second author. In joint discussions, codes were grouped into themes and checked for
similarities and differences, emerging patterns and
variability. Through a process of reading and rereading,
the themes were refined. This approach to
analysis allowed the Somali women’s unique perspective
to be explored and themes to be grounded in the
data.
Findings
In total, 23 participants were recruited for interviews
which took place between February and April 2012
at two centres (A and B). Three women interpreters
assisted the interviewer with seven of the interviews.
The letter i is used to denote a direct quote taken from
an interview that was conducted with the aid of an
interpreter.
The data were organised around three broad themes
which facilitated insight into the factors that influence
Somali mothers’ decision making:
1 perceptions about preschool immunisations
2 personal beliefs and practices
3 knowledge and understanding of preschool immunisations.
Specific quotes from participants have been used to
demonstrate the themes outlined above. Additional
verbatim quotes can be found in Boxes 2, 3 and 4.
These serve to direct the reader to further quotes that
support the themes which are further explored below.
Perceptions of preschool
immunisations
Understanding mothers’ perceptions of preschool
immunisations is crucial to appreciating the reasons
that drive vaccination practice. This theme describes
views about the importance of preschool immunisations,
beliefs specific to the MMR vaccine, and the
influence of personal experience on immunisation
practices.
General attitudes towards immunisation
All of the participants were positive about preschool
immunisations, regarding them as ‘very important’
for their children’s health (Interview B19). Immunisations
were viewed as a ‘good option for the children’
(Interview B3i), with several mothers adding that they
‘always make sure that they get it on time’ (Interview
B7).
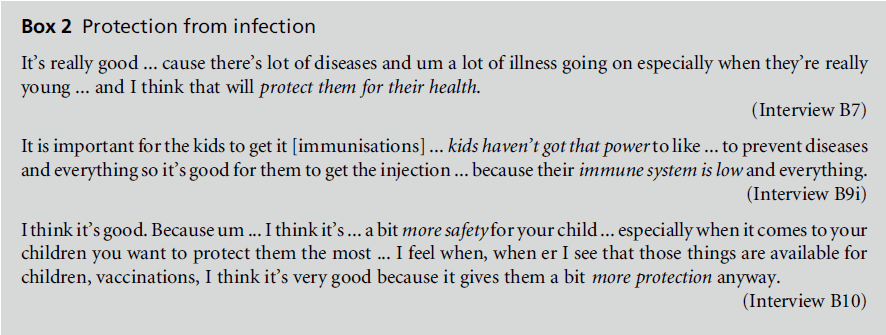
Protecting children from infection
The participants viewed preschool immunisations as
important because of their perceived role in protecting
children from disease (see Box 2). Some women
regarded young children as a vulnerable group who
‘don’t have power to prevent diseases for themselves’
(Interview B20i). Immunisations were seen as providing
long-term protection from infection, not just
protection when their children were young. One participant
explained that immunisations were ‘good for
your children because maybe when they grow up they
sick and maybe they died if they hasn’t had the ...
injections’ (Interview B18).
However, the majority of the participants made a
clear distinction between the MMR vaccine and all
other preschool immunisations. One participant
highlighted this distinction at the start of the interview:
‘I think some of them it’s good ... my children
have had all of them ... except one, but I’ve done all of
them for them and it’s really good.’ She then explained
that ‘the one I haven’t done is MMR’ (Interview B5).
Other participants talked at the beginning about their
positive perceptions of preschool immunisations, but
explained their fears about the MMR vaccine later in
the interview: ‘OnlyMMRI very afraid ... but the other
injections I don’t have any problem’ (Interview B6).
Another woman mentioned that she ‘didn’t give the one for one years old [MMR]’, despite later saying that
‘all injections is important for the children’ (Interview
B11).One mother explained that the distinction between
the vaccines was due to her belief that the MMR
vaccine was more powerful than the other immunisations,
and therefore more likely to cause harm to her
children.
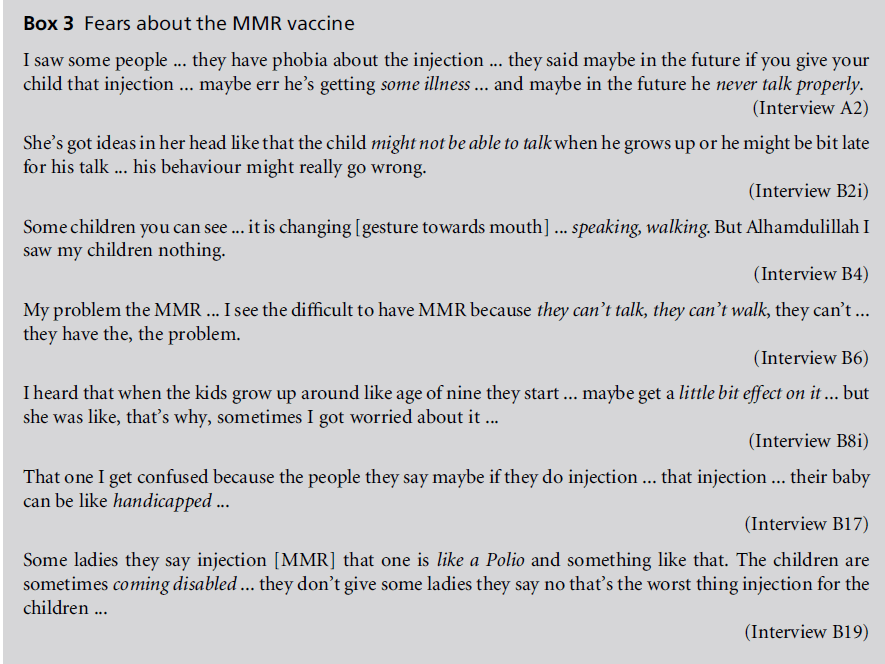
The perceived risks of the MMR vaccine
The distinction between the MMR vaccine and other
preschool immunisations was primarily due to anxiety
about a link with autism (see Box 3). One mother
explained that the MMR vaccine is the one she is ‘not
sure about’ due to her fear that ‘it gives speech
problems’ (Interview B9i). This mother allowed her
child to receive the MMR vaccine, but only because
she heard the rumours afterwards. The majority of the
participants mentioned the fear among the Somali
community: ‘a lot of people around me say because of
theMMRthere is a lot of diseases ... especially they are
saying about the autism’ (Interview A1). This suspicion
was fuelled by further rumours about possible
risks associated with the vaccination, with women
reporting how their ideas were affected by the views
of others. One participant described this phenomenon
and the effect that it had on her willingness to
vaccinate her child:
Loads of Somali women told me if you give your child that
one he’ll turn into disability ... he will not function the
same ... when you hear those things you go – ohmy God –
I don’t want to give him something that ... is actually going
to harm him because the whole point of this is actually to
improve him, to protect him.
(Interview B1)
This fear had caused five of the participants to refuse
theMMR vaccine for their child, even though many of
them readily accepted all of the other preschool
immunisations. One mother explained that ‘sometimes
... you are afraid ... you bring your healthy son in
[to see] the GP and they give you injection and some
day he become ... handicapped’ (Interview B11).
Another participant explained that, in her opinion,
MMR has ‘got more strong things inside’ (Interview
B5).
Participants claimed to have witnessed the detrimental
effects of the MMR vaccine on other children,
and cited this as one of the reasons for not vaccinating
their own children. One mother explained how her
neighbour had a daughter who ‘had a brain damage
because of that [MMR vaccine].’ She therefore felt
unable to take her child to the GP for the MMR
vaccine: ‘when you see those kids, I feel like I don’t
wanna takemy children to let somebody give them an
injection.’ The mother talked about her shock that the
MMRvaccine was able to have that effect on a child: ‘I
didn’t believe that injection could do that ... it’s
something strong obviously!’ (Interview B5). Another
participant also talked about her ‘phobia’ of theMMR
vaccine due to the fact that her neighbour’s son
received the MMR vaccine and is now autistic: ‘he
can’t speak ... and his mum she tells me when he was
one and a half years she give that injection. It’s the
second person I heard ...’ (Interview B11).
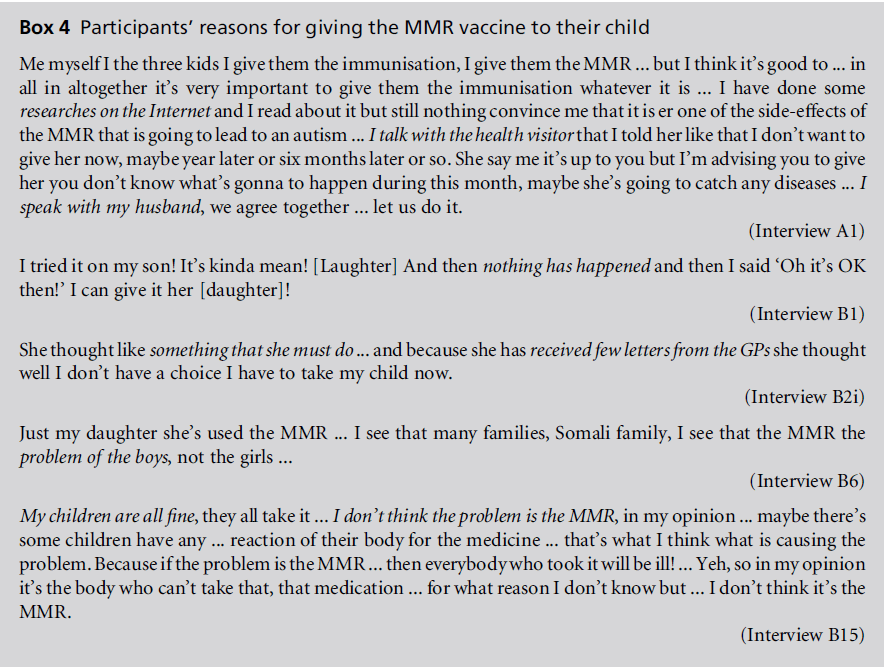
Anticipated guilt also played a role in decision
making about the MMR vaccine. One mother who
refused to vaccinate her child talked about how she
would blame herself if her child was to become
autistic: ‘you’re just gonna ask yourself every time,
why did I do this? You’re just going to regret every
time ...’ (Interview B5). She further explained that it
would be her responsibility and not that of the GP, as
‘taking them to their GP is my fault! ... and have them
the injection and sign for them is gonna be my fault’
(Interview B5). Despite this apprehension about the
MMR vaccine, 18 mothers had allowed their children
to be immunised. Their reasons for doing so are listed
in Box 4.
The perceived importance of specific
immunisations
Despite the anxiety and suspicion about the MMR
vaccine, some participants identified other immunisations
as particularly important, including those protecting against tuberculosis, polio and measles. Beliefs
about their importance were based on the perception
that childhood diseases, against which these vaccines
provide protection, can be placed along a spectrum of
severity. The position of a disease on this spectrumwas
determined by the perceived danger of permanent
disability or death. These beliefs were often based on a
mother’s recollection of witnessing the consequences
of certain childhood diseases in Somalia:
The most important one ... polio! Because in our country
we used to have a lot of kids ... I know some of my cousins
because they didn’t immunise them ... now they have a
problem with their walking.
(Interview A1)
Several mothers attached great importance to the
immunisations received during early childhood, due
to the perceived increased vulnerability of very young
babies to infection:
If somebody got flu ... it’s easy for them to get everything
... they’re quite young and can’t tell you anything ... the
child can just cry.
(Interview B5)
I think ... those in the two, three, four months ... those are
very important ... they’re so small and so vulnerable at that
age ... the fact that everyone who’s walking around them ...
they could give it to him ... and I think ... yeh definitely.
Maybe because inmyeyes how smaller they are, how more
vulnerable ... that’s why I think those are more important.
(Interview B10)
One participant attached much importance to ‘the
one in three to four years when they starting school’
due to the fact that before the child started school they
were ‘only with you, not for another children’, and so
were less likely to acquire infections. However, once
the child started school they were viewed as being
more susceptible to infection, due to their increased
interaction with other children: ‘when she start at
school she need protect more flu ...’ (Interview B19).
The influence of personal experience
The attitudes of many of the participants towards
preschool immunisations were shaped by their personal
experiences during childhood. One mother
believed that the vaccine against tuberculosis is the
most important vaccination, as ‘that’s the only important
one that they do back home ...’ (Interview
B2i). Several participants related their own positive
experience of immunisation to their current views on
preschool immunisations. One woman talked about
how her father took ‘care to immunise us as kids’ and
therefore she has ‘an idea about immunisations for the
kids ... I think it’s a good idea’ (Interview A1). Another
participant believed that ‘it’s really a good opportunity
that we have it [preschool immunisation], [be]cause I think back home a lot of people they don’t
get it ... when they have small virus ... they get really
poorly and they die quickly’ (Interview B10).
Conversely, other participants believed that immunisations
are ‘not really that important because we
never had that back home’ (Interview B2i). One
woman explained the manner in which her own
experience had shaped her belief in the need for
preschool immunisations: ‘we [Somali women] don’t
believe that it’s gonna help them [children] anything
... basically we don’t believe all injections does anything.
Because in our country we didn’t have one
injection ... and as you can see we are healthy and
everything!’ (Interview B5). This opinion was reiterated
by another participant who ‘never got it done’
and ‘never had any harms’ (Interview B12i).
The UK urban environment as a potential
threat to health
Several participants drew a clear distinction between
the importance of vaccinating children in Somalia
compared with vaccinating them in the UK: ‘it’s
different you know, compared to our country it’s
different in here [UK]’ (Interview B5). Another participant
stated that ‘I think the problem – where do
you live? [Be]cause when you live the tropical city like
my country, it’s different ... when you live here it’s ...
different’ (Interview B6). The environment in the UK
was viewed as a potential threat to their children’s
health, as it was perceived as overpopulated and dirty,
thus increasing their children’s vulnerability to disease.
As one participant explained, ‘when it was our
country [Somalia] ... you’ve got big country ... it was
healthy, every day what you eating, it’s healthy ... and
we don’t do injection, but if you come here you have to
do it because the environment ... the ground is small
and the people, population is big ... and here it’s cold
country – you have to!’ (Interview B11). This participant
emphasised that, in the UK, ‘the roads is more ...
and too much cars ... [this part of the city], it’s not a
clean place when you go to there, it’s the dirtiest place
in [this city]!’ (Interview B11).
Personal beliefs and practices
This theme addresses the personal beliefs and practices
of the Somali mothers, and the way in which they
mediated beliefs about health and illness. The data
suggest that these beliefs are shaped by the social and
cultural interpretations of Islam and practices associated
with them.
The role of ideas related to Islam
Many of the participants reported that religious belief
per se did not play a critical role in the decision to
immunise their child, as ‘our religion don’t prevent ... anything that has to do with improving your health’
(Interview B3i). Another participant explained that
‘religion doesn’t really play a role in my decision.’ This
was due to the fact that ‘in our religion it says whatever
that’s good for your health ... just do it’ (Interview
B14i). Indeed, maintaining one’s health and the
family’s health is seen as an obligation in Islam, and
the prevention of illness is highly valued (Brooke and
Omeri, 1999). However, although most of the women
were not against preschool immunisations, they did
not necessarily believe in the capacity of vaccines to
prevent disease, believing instead ‘in God and whatever
happens to that child, [be]cause God gave it to
her’ (Interview B2i). Many of the participants believed
that it was Allah who protected their children, and
therefore it was ultimately in Allah’s gift as to whether
or not their child became sick: ‘I do believe it [immunisations]
... reduce diseases. But God knows – he can
bring the kids to be sick or not to be sick basically’
(Interview B8i). This attitude to health and illness,
which might be characterised as fatalistic, was evident
in several of the interviews, and was most clearly
expressed as ‘if something’s going to happen, then
it’s gonna happen’ (Interview B2i). Fatalism is the
belief that all events are predetermined and therefore
inevitable, so that there is an unavoidable tension
between fatalism and autonomous behaviour (Esposito,
2003). However, in this study, such an attitude did not
necessarily prevent mothers from vaccinating their
children, but it did appear to affect their confidence in
the ability of immunisations to avert disease. As one
participant explained, ‘it’s our responsibility to check
our kids and they’re in good health and we do as much
as we can ... if after I protect them something happens,
so that’s out of my control, nothing I can do about it’
(Interview A1). Another participant explained that
‘whatever is going to happen is going to happen ... you
just have to believe in these kind of things’ (Interview
B7).
Gelatine as a constituent part of the
vaccine
Interpretations of religious texts also played a role in
the participants’ trust in the ingredients of vaccines.
This was particularly evident with regard to the MMR
vaccine and their anxiety that it contained gelatine, a
pig-based product forbidden in Islam. Their response
to this fear varied. Some women held the view that ‘it’s
only injection’ and that it is not a major concern
because ‘it’s not food every day’ (Interview B19).
Another participant explained that ‘if somebody
sometimes they are really sick and maybe they need
that medicine from gelatine ... it’s permitted’ (Interview
B17).
Nevertheless, several other participants regarded
gelatine as a significant barrier to immunisation: ‘it
got haram things like the pig ... that’s the most of thing we don’t like’ (Interview B5). One woman stated that
her anxiety about the vaccine containing gelatine
prevented her from immunising her child: ‘if there
wasn’t the gelatine in it ... shewould have got it done as
well. Because of the gelatine ... definitely she wouldn’t
get it done’ (Interview B12i). For several participants,
the presence of gelatine was mentioned as a factor as
significant as their fear of autism in preventing them
from vaccinating their child against MMR.
Knowledge and understanding
The mothers’ confidence in the immunisation programme
was based on their knowledge and understanding
of the immunisations and the benefit of these
to their children’s health. This theme explores their
situated understanding, which was a product of community
narratives and personal experience, the lack of
specific biomedical knowledge among the Somali
community, and the lay interpretations of preschool
immunisations.
Lay interpretations of immunisation
The participants’ understanding of immunisation was
shaped by their personal experience and social interactionswith
others from their community, rather than
by biomedical knowledge. Many women attributed
the lack of scientific knowledge among the Somali
community to the fact that many of them had to leave
Somalia before they had completed their education.
One mother explained that ‘when I finished secondary
school, the war started, I didn’t go to college and most
of the Somali woman they didn’t go to school ... they
don’t have a knowledge’ (Interview B11). Another
participant added that many of her friends ‘don’t have
a good idea about immunisation’, and so many
mothers ‘didn’t do the immunisation up to date to
their kids’ (Interview A1).
One participant talked about her own lack of
biomedical knowledge and how she ‘hasn’t got a
much explanation’ about preschool immunisations,
which causes her to be fearful of vaccinations. She
explained that ‘as soon as I take my child there [to the
GP] they start injecting the child and I don’t know
what that is ... and then at night time he might just
have a fever or anything ...’ The mother explained that
‘I don’t understand what they just did to my child and
whether my child in the future will be [disabled]’
(Interview B2i).
Unable to draw on biomedical information about
the mechanisms of immunisation, the participants
were anxious about the possibility of causing harm
to their small children. One mother explained that ‘if
you ask all the Somali woman [about preschool
immunisation] ... they will go ‘‘No, very bad!’’ To
them it’s like, why would I interfere something if my child already doesn’t have it? ... Why put something in
them?’ (Interview B1). Another participant described
how some women view the vaccine as containing ‘five
different diseases in one injection, in one needle.’ This
scares many mothers, who think ‘he’s a baby, he’s very
small, he cannot take five different doses in five
different diseases in one. So it’s going to hurt him
instead of taking benefit from him’ (Interview A1).
Social obligation
The participants stated that mothers in the UK have a
social obligation to vaccinate their children. This was
cited as one of the reasons for immunising their own
children, irrespective of whether they believed they
were doing the right thing. One mother feared that an
incomplete vaccination history would be detrimental
to her child’s future educational prospects: ‘when your
child starts school they check the red book ... if the
child doesn’t have all these immunisations then obviously
the school is not going to take them.’ She then
talked about the problems her child might face ‘when
he grows up or when he decides to go to university ...
they might just check up on his past health and if they
see there on his record that the child didn’t have the
MMR or any ... he might have a problem’ (Interview
B2i).
The participants also described their perceptions of
the extent to which preschool immunisations are
mandatory in the UK. One participant talked about
the fact that ‘the GP has sent out letters saying that she
must bring her child’ and so ‘she thought well I don’t
have a choice I have to take my child now’ (Interview
B2i). Another participant explained that ‘it feels like
we have to have it, all the others ... but you can say no
to MMR!’ (Interview B5).
The need for the provision of information
Many women were aware that they had insufficient
knowledge about how immunisation works in children
and howimmunisation policies are implemented
in the UK, and they attributed this to the poor
provision of information to the Somali community.
The majority of the participants stated that they had
not received any written information in Somali about
preschool immunisations. One participant asked
whether ‘the GPs could bring out more information
... other people who can speak the language ...’ in order
to ‘help them understand ...’ (Interview B7).
Several mothers also mentioned communication as
a ‘big barrier’ for them to ‘know what we need or what
exactly this thing is going to be, the benefit of this
service for us’ (Interview A1).One participant explained
that ‘it would be nice if you could just pass it and tell
anyone from the NHS if they could just explain to
them and then the fear that they’ve got at the moment
[would disappear]’ (Interview B2i).
Discussion
This is the first study to specifically address the health
beliefs of migrant Somali communities in the UK with
regard to preschool immunisation. It explored the health
beliefs of Somali women residing in Birmingham, and
provided some insights into the views of this growing
minority ethnic community.
It is evident that perceptions of risk were mediated
by three main factors, namely women’s social network,
their knowledge and understanding about the
relative risk of infection versus vaccination, and their
own experience. These factors highlighted the way
that the women shaped decision making in terms of
balancing the potential harm to their children as a
result of infection and the harm that might arise from
vaccination.
The participants’ social network played a significant
role in their beliefs about preschool immunisations.
There was a strong emotional component to the
decision-making process, which was characterised by
mistrust and fear. This was especially evident when
considering the potential side-effects of vaccines, and
it was further exacerbated by frightening stories circulating
among the Somali community which many
participants believed strongly enough for this to affect
their immunisation practice. The influence of the
social network was particularly evident in relation to
attitudes towards the MMR vaccine.
Fear surrounding the MMR vaccine was fuelled by
both a lack of relevant biomedical knowledge and the
influence of rumours about the possibility of damage.
These rumours persist despite publicity which discredited
the study by Wakefield et al (1998). Previous
research (Brownlie and Howson, 2005; Brown et al,
2012) explored the considerable influence of friends
and family on mothers’ decision making about the
MMR vaccine. Participants often mentioned the MMR
vaccine, the controversy surrounding its link with
autism, and the subsequent effect that this had had
on their willingness to vaccinate their child. They cited
second or third-hand experience of a link between
MMR and autism, and the subsequent effects that this
had had on their own opinions about the safety of the
vaccine. This phenomenon was also evident in our
study, in which several mothers talked about family
members or friends whose children appeared to have
become autistic after receiving theMMR vaccine. The
validity of these claims is impossible to verify. However,
what is obvious is the extent towhich this fear has
penetrated the Somali community and continues to
influence decision making about the MMR vaccine.
Appropriate information that explicitly addresses
anxieties and suspicions, as well as a closer relationship
between the local Somali community and healthcare
professionals, are essential for improving the uptake of immunisation against measles, mumps
and rubella.
Ehreth (2003) discusses the idea that the decision to
vaccinate is often made on a vaccine-by-vaccine basis,
a phenomenon that was evident in the specific fear and
apprehension among the participants about theMMR
vaccine and its purported link to autism. Individuals
often had limited knowledge, which added to their
dilemma of balancing the risk of infection against the
fear of the long-term consequences of vaccination.
This sense of conflict between harm and benefit was a
theme explored by Brownlie and Howson (2005),
whose study participants discussed their fear of making
the wrong decision and exposing their child to
potentially harmful diseases or to the risk of autism.
Parents felt directly responsible and feared subsequent
feelings of guilt, a view that was also expressed by
participants in our study.
It is important that parents receive the necessary
information to enable them to make an informed
decision about preschool vaccination. The evidence
suggests that parental decision making about preschool
immunisation involves seeking both formal
and informal information (Marshall and Swerissen,
1999). Similarly, the participants in our study used a
variety of sources to obtain information about
preschool immunisation and reach a decision about
their child. These included discussions with friends,
family and religious advisers, as well as research on the
Internet. However, several participants mentioned a
lack of written information in Somali about preschool
immunisations, and a general lack of knowledge among
the community. This is a serious issue which arguably
affects the ability of mothers to give informed consent
with regard to their child’s preschool immunisations.
It is therefore important that accurate, reliable and upto-
date information is provided to the Somali community,
and that healthcare professionals work closely
with religious advisers so that mothers can be appropriately
counselled.
Many of the participants explained that their previous
experience had influenced their opinions and
practice with regard to preschool immunisation. The
decision to vaccinate is made in the context of life
experience, and is a dynamic process that changes over
time (Marshall and Swerissen, 1999). This was evident
in the extent to which personal experiences in Somalia
influenced the attitude of participants towards preschool
immunisation; several women recalled high
levels of morbidity and mortality among unvaccinated
children in Somalia, and so attached increased importance
to preschool vaccination. Others believed
that preschool immunisations were not necessary, as
they had no recollection of being vaccinated as children
and yet had remained healthy, which affected
their confidence in the ability of immunisations to
prevent disease. Vaccination programmes in Somalia are not as robust as those in the UK, and access would
not necessarily have been uniform across the country,
with additional variation between rural and urban
areas (Cassell et al, 2006; Macassa et al, 2011). The
participants’ own experiences of vaccinations could
therefore have been shaped by where they lived in
Somalia. However, it is important that, despite their
own experiences, Somali mothers are made aware of
the importance of preschool immunisations in improving
child health beyond their own family and
community. This might include information about
herd immunity and the consequences of suboptimal
vaccination.
Despite the various health beliefs expressed by the
participants, most of the mothers did vaccinate their
children. However, their decision was not necessarily
based on rational information, but on the fear that an
incomplete immunisation history would be detrimental
to their child’s future educational prospects. Other
reasons for vaccination included a perceived social
obligation as well as a belief that the environment in
the UK posed a greater threat to their child’s health
than that in Somalia.
Limitations of the study
There are both methodological and ethical challenges
when conducting cross-cultural research, especially in
relation to interviewing (Redwood et al, 2012). These
include differences in the social position of the participants
and the researcher, as well as in their educational
background and understanding of the topic
under investigation.
Building and maintaining trusting relationships
with the organisations that provided services for
potential participants was an important part of the
recruitment stage, and enabled staff in community
organisations to help to bridge the gap between the
researcher and potential participants.
Face-to-face interviews are inherently subject to
social desirability bias, that is, the tendency for participants
to answer questions in a manner they view as
socially acceptable (Garrett, 2010). In our study, social
desirability bias could result in over-reporting of
vaccination uptake and positive views about preschoolimmunisations
leading to a false representation
of attitudes among Somali mothers. However, the
range of opinions and health beliefs expressed during
this study indicates that this formof bias may not have
had a significant effect on the data collected. The
participants discussed non-adherence to certain vaccinations
and mentioned their suspicion of the MMR
vaccine, issues that they would not have discussed if
they had wanted to answer questions in a socially
acceptable manner.
A further issue relates to the reliability of the data, as
the study was conducted by a white non-Muslim
researcher who explored the participants’ views on a
topic that appeared to be influenced by religious belief
and culture. Appropriate dress was therefore important,
as was an open, non-judgemental manner when
potentially sensitive topics were discussed. The researcher’s
lack of religious affiliation may have enabled
the participants to discuss the impact of religious
belief on their decision making without feeling under
pressure to conform to any particular expectations.
Interpreters were required for seven participants,
and were enlisted from the centres at which the participants
were recruited. Although external interpreters
are preferable, the centres involved in this study were
located at the heart of Somali communities. These
communities are very close-knit and take time to trust
outsiders. We considered the use of an external interpreter
inappropriate because it could have negatively
affected the trusting relationship that had been
developed with the participants, and thus limited the
reliability of the data. However, the short time period
allowed for this study meant that we did not account
for the effects of the interpreters on the data, which
may have limited the cross-language trustworthiness
of the translated data (Squires, 2009, p. 285). This
refers to factors that could compromise the credibility
and transferability of translated data.
Conclusions
Our findings indicate that the Somali mothers in this
study generally had positive attitudes towards immunising
their children, but that they had specific
concerns and anxieties about the MMR vaccine. The
participants referred to stories circulating in the local
communities and limiting their confidence in the
safety of the vaccine. Social and cultural interpretations
of Islam and practices associated with them
affected the decision making of some mothers with
regard to both the ingredients used in the MMR
vaccine and their confidence that immunisations
prevent disease. Our study highlights the importance
of women’s understanding and perception of risk and
how these shape decision making in relation to potential
harm to their children as a result of infection on
the one hand, and as a result of vaccination on the
other. Risk perceptions were mediated by the women’s
social networks and social norms, their knowledge and
understanding about the risk of infection versus
vaccination, and their own experience. Their decision
making had a strong emotional component, which
was characterised by mistrust and fear. Appropriate
information that explicitly addresses anxieties and
suspicions, as well as a closer relationship between the local Somali community and healthcare professionals,
will be crucial for future vaccination services
to ensure adequate uptake.
Acknowledgment
We wish to thank the women who participated in this
study and the organisations that helped with recruitment.
We are grateful for their enthusiasm and
kindness.
This study was funded by the University of
Birmingham. SR is funded by the National Institute
for Health Research (NIHR) through the Collaborations
for Leadership in Applied Health Research and
Care for Birmingham and Black Country programme.
The views expressed are those of the authors and not
necessarily those of the NHS, the NIHR or the Department
of Health.
NT and SR developed and designed the study. NT
carried out data collection and analysis, supervised by
SR. NT produced the initial draft of the manuscript,
which was revised and developed by SR. Both authors
agreed the final draft.
CONFLICTS OF INTEREST
None.
References
- Birmingham City Council (2009) Ethnicity of BirminghamResidents.www.birmingham.gov.uk/cs/Satellite?c=Page&childpagename=Planning-and-Regeneration%2FPageLayout&cid=1223096353923&pagename=
BCC%2FCommon%2FWrapper%2FWrapper (accessed 23 March2012).
- Birmingham City Council (2012) ChildrenÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s Centres.www.birmingham.gov.uk/childrens-centres (accessed 6May 2012).
- Braun V and Clarke V (2006) Using thematic analysis inpsychology. Qualitative Research in Psychology 3:77ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â101.
- Brooke D and Omeri A (1999) Beliefs about childhoodimmunisation among Lebanese Muslim Immigrants inAustralia. Journal of Transcultural Nursing 10:229ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â36.
- Brown K, Long S, Ramsay M et al (2012) UK parentsÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢decision-making about measlesÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
âmumpsÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
ârubella (MMR)vaccine 10 years after the MMR-autism controversy: aqualitative analysis. Vaccine 30:1855ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â64.
- Brownlie J and Howson A (2005) ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âLeaps of faithÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ and MMR:an empirical study of trust. Sociology 39:221ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â39.
- Cassell JA, Leach M, Fairhead JR et al (2006) The socialshaping of childhood vaccination practice in rural andurban Gambia. Health Policy and Planning 21:373ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â91.
- Central Intelligence Agency (2012) The World Factbook:Somalia. www.cia.gov/library/publications/the-worldfactbook/rankorder/2112rank.html?countryName=Somalia&countryCode=
so®ionCode=afr&rank=211#so (accessed3 May 2012).
- Condon L (2002) Maternal attitudes to preschool immunisationsamong ethnic minority groups. Health EducationJournal 61:180ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â89.
- DiCicco-Bloom B and Crabtree B (2006) The qualitativeresearch interview. Medical Education 40:314ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â21.
- Ehreth J (2003) The global value of vaccination. Vaccine21:596ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â600.
- Elam G and Fenton KA (2003) Researching sensitive issuesand ethnicity: lessons from sexual health. Ethnicity andHealth 8:15ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â27.
- Esposito JL (2003) Fatalism. In: Oxford Dictionary of Islam.Oxford: Oxford Reference Online, Oxford UniversityPress.
- Faugier J and Sargeant M (1997) Sampling hard to reachpopulations. Journal of Advanced Nursing 26:790ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â97.
- Fine M (1993) Herd immunity: history, theory, practice.Epidemiological Review 15:265ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â302.
- Food Security Analysis Unit (2007) Somali Knowledge Attitudeand Practices Study (KAPS). www.fsnau.org/downloads/FSNAU-Somalia-KAP-Report-Dec-07.pdf(accessed 2 April 2012).
- Garrett P (2010) Attitudes to Language. Cambridge:Cambridge University Press.
- Hammersley M (2001) WhatÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s Wrong with Ethnography?Methodological explorations. Oxford: Routledge.
- Holloway I and Wheeler S (2010) Qualitative Research inNursing and Healthcare (3e). Chichester: Wiley-Blackwell.
- Jones A (2007) The Unexpected Community: the needs andaspirations of BirminghamÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢s Somali community.
- Birmingham: Human City Institute. www.humancity.org.uk/reports/publications
/THE%20UNEXPECTED%20COMMUNITY%20-%20SEPTEMBER%
202007.pdf(accessed 23 April 2012).
- Kulane A, Johansson A, Robleh I et al (2007) Somali ParentsÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢Acceptance of MPR Vaccination for their Children: anexploratory study. Stockholm: KarolinskaInstitutet. www.webbhotell.sll.se/Global/Bhv/Dokument/Rapporter/MPR-study_Rinkeby.pdf (accessed 14 April 2012).
- LaFond A (1993) Deterrents to immunisation in Somalia: asurvey of mothersÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢ attitudes. Development in Practice3:27ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â35.
- Macassa G, Hallqvist J and Lynch JW (2011) Inequalities inchild mortality in sub-Saharan Africa: a social epidemiologicframework. African Journal of Health Sciences18:14ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â26.
- Marshall S and Swerissen H (1999) A qualitative analysis ofparental decision making for childhood immunisation.Australian and New Zealand Journal of Public Health23:543ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â5.
- Mason J (2002) Qualitative Researching (2e). London: Sage.
- Mays N and Pope C (1995) Rigour and qualitative research.British Medical Journal 311:109ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â12.
- National Health Service (2010) NHS ImmunisationStatistics:England 2009ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â10. Leeds: The Health and Social CareInformation Centre. https://catalogue.ic.nhs.uk/publications/public-health/immunisation/nhs-immu-stateng-2009ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â2010/nhs-immu-stat-eng-2009ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â2010-rep.pdf(accessed 18 February 2013).
- Penrod J, Preston DB, Cain RE et al (2003) A discussion ofchain referral as a method of sampling hard-to-reachpopulations. Journal of Transcultural Nursing 14:100ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â7.
- Pickard A (2005) Childhood Immunisation across Birmingham: ahealth equity profile. Birmingham: BirminghamPublic HealthNetwork, Public Health Information Team for Birmingham.
- Redwood S, Gale N and Greenfield S (2012) ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ãâ¹Ã
âYou give usrangoli, we give you talkÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Å¾Ã¢: using an art-based activity toelicit data from a seldom heard group. BMC MedicalResearch Methodology 12:7.
- Salisbury D, Ramsay M and Noakes K (eds) (2006) ImmunisationAgainst Infectious Disease (3e). London: TheStationery Office. Part 2.15, pp. 109ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â26.
- Squires A (2009) Methodological challenges in crosslanguagequalitative research: a research review. InternationalJournal of Nursing Studies 46:277ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â87.
- Teddlie C and Yu F (2007) Mixed methods sampling: atypology with examples. Journal of Mixed Methods Research1:77ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â100.
- UNICEF (1996) Sustainability of Achievements: LessonsLearned from Universal Child Immunization. Report of aSteering Committee. https://immunizationbasics.jsi.com/Docs/BASICS/UCISustainabilityReport.pdf
- Wakefield AJ, Murch SH, Anthony A et al (1998) Ileallymphoid-nodular hyperplasia, non-specific colitis, andpervasive developmental disorder in children. Lancet351:637ÃÆÃâÃââÃÆââ¬Å¡Ã¢ââ¬Å¡Ã¬ÃÆââ¬Å¡Ã¢ââ¬Ã
â41.
- World Health Organization (2012) 10 Facts onImmunization.www.who.int/features/factfiles/immunization/en/index.html (accessed 4 May 2012).

